(UroToday.com) The 2022 Southeastern Section of the AUA’s annual meeting included a prostate cancer session and Dr. Christopher Koller discussing a prospective observational prostate cancer study assessing the potential for upgrading on active surveillance among African American men. For several decades, active surveillance has been the preferred management option for patients with localized low risk prostate cancer without high risk of prostate mortality. The hypothesis for this study was that race is not associated with Gleason upgrading on active surveillance, and that active surveillance is a safe management option for both African American and Caucasian American appropriately selected patients.
All patients on active surveillance at the Southeast Louisiana Veterans Health Care System are entered into a prospectively kept database for review. Patients were divided into groups based on race and NCCN risk classification, and Grade Group progression was defined as pathologic upgrading > ISUP Grade Group 1 disease. Mann-Whitney U and Fisher exact tests were used to compare demographics. The protocol used for active surveillance follow-up is as follows:

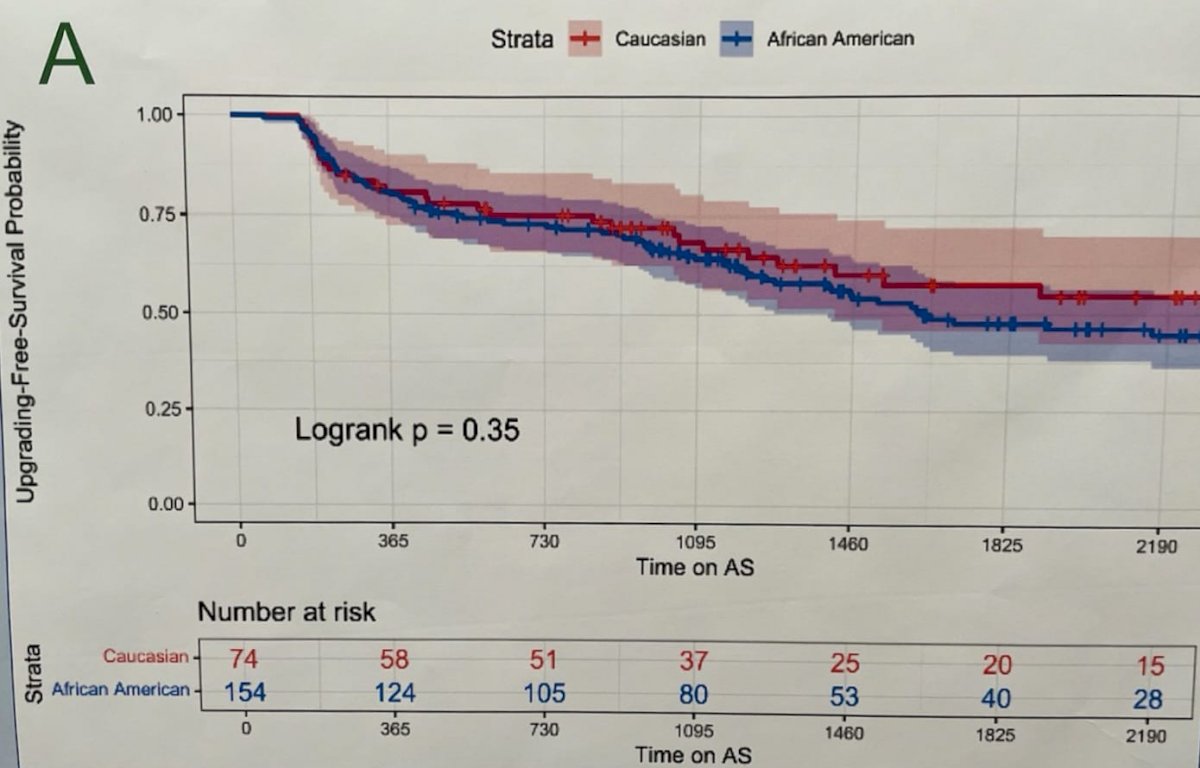
There were 228 patients queried, including 154 African American (67.5%) and 74 Caucasian American patients, for which there was no significant difference in demographics between the African American and Caucasian American groups. Patients were followed for an average of 54.2 months and time on active surveillance of 41.1 months. There was no difference in history of negative biopsy before prostate cancer diagnosis (p = 0.10), National Comprehensive Cancer Network (NCCN) risk category (p = 0.84), PSA (p = 0.40), PSA density (p = 0.84), TRUS volume (p = 0.50), or number of positive cores at diagnosis (p = 0.48). Overall, 48% of African American patients and 36% of Caucasian American patients had Gleason upgrading (p = 0.089), and 48% of African American and 34% of Caucasian American patients received definitive treatment (p = 0.036). Race was not predictive of Grade Group progression (HR 1.01, p = 0.96), active surveillance discontinuation (HR 0.94, p = 0.79), or biochemical recurrence (HR 0.85, p = 0.81). As follows is the Kaplan-Meier curve of Grade Group progression-free survival stratified by race (log-rank p = 0.35):
As follows is the Kaplan Meier curve of Grade Group progression-free survival stratified by race and NCCN risk classification:

Dr. Koller concluded his presentation with the following summary points:
- Active surveillance is a safe treatment option for low and very low risk prostate cancer, regardless of race
- African American and Caucasian American men did not have any significant difference in Gleason upgrading in this cohort, though African American patients did receive definitive treatment more often
- Long term follow-up is needed to track and verify these outcomes
Presented By: Christopher Koller, MD, Department of Urology, Tulane School of Medicine, New Orleans, LA
Co-Authors: Joshua Pincus, Jacob W. Greenberg, Caleb Natale, L. Spencer Krane
Affiliations: Department of Urology, Tulane School of Medicine, New Orleans, LA
Written By: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 86th Annual Meeting of the Southeastern Section of the American Urological Association, San Juan, PR, Mar 16 – 19, 2022