(UroToday.com) The 2025 South Central AUA annual meeting included a session on prostate cancer, featuring a presentation from Dr. Renil Titus discussing a comparison of cardiovascular events in patients with metastatic castrate sensitive prostate cancer (mCSPC) treated with LHRH agonists to LHRH antagonists in the US. The standard of care for mCSPC is ADT using LHRH agonists (ie. leuprolide, goserelin or triptorelin) or LHRH antagonists (ie. degarelix or relugolix) plus intensification with androgen receptor signaling inhibitors, with or without chemotherapy. Post hoc analyses have suggested that the risk of major adverse cardiovascular events among patients receiving LHRH antagonists may be lower than those receiving LHRH agonists. Using real world, de-identified data from multiple hospitals in the US (TriNetX), Dr. Titus and colleagues examined the association between major adverse cardiovascular events and receipt of LHRH agonists versus LHRH antagonists.
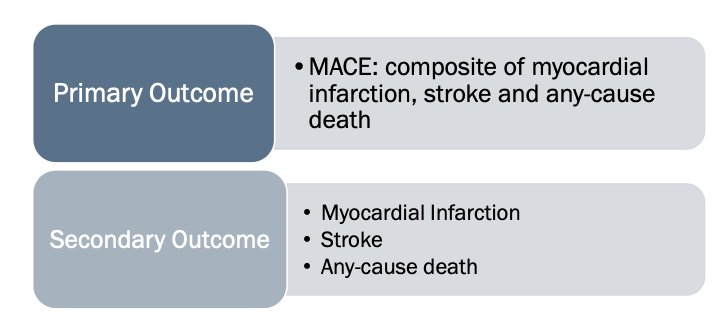
This study was a retrospective cohort study that included adult mCSPC patients who received either an LHRH agonists or LHRH antagonists. The primary outcome was major adverse cardiovascular events (defined as myocardial infarction, stroke, and deaths from any cause). Secondary outcomes were rates of myocardial infarction, rates of strokes, and overall mortality:
Covariates were chosen based on the HERO randomized clinical trial:1
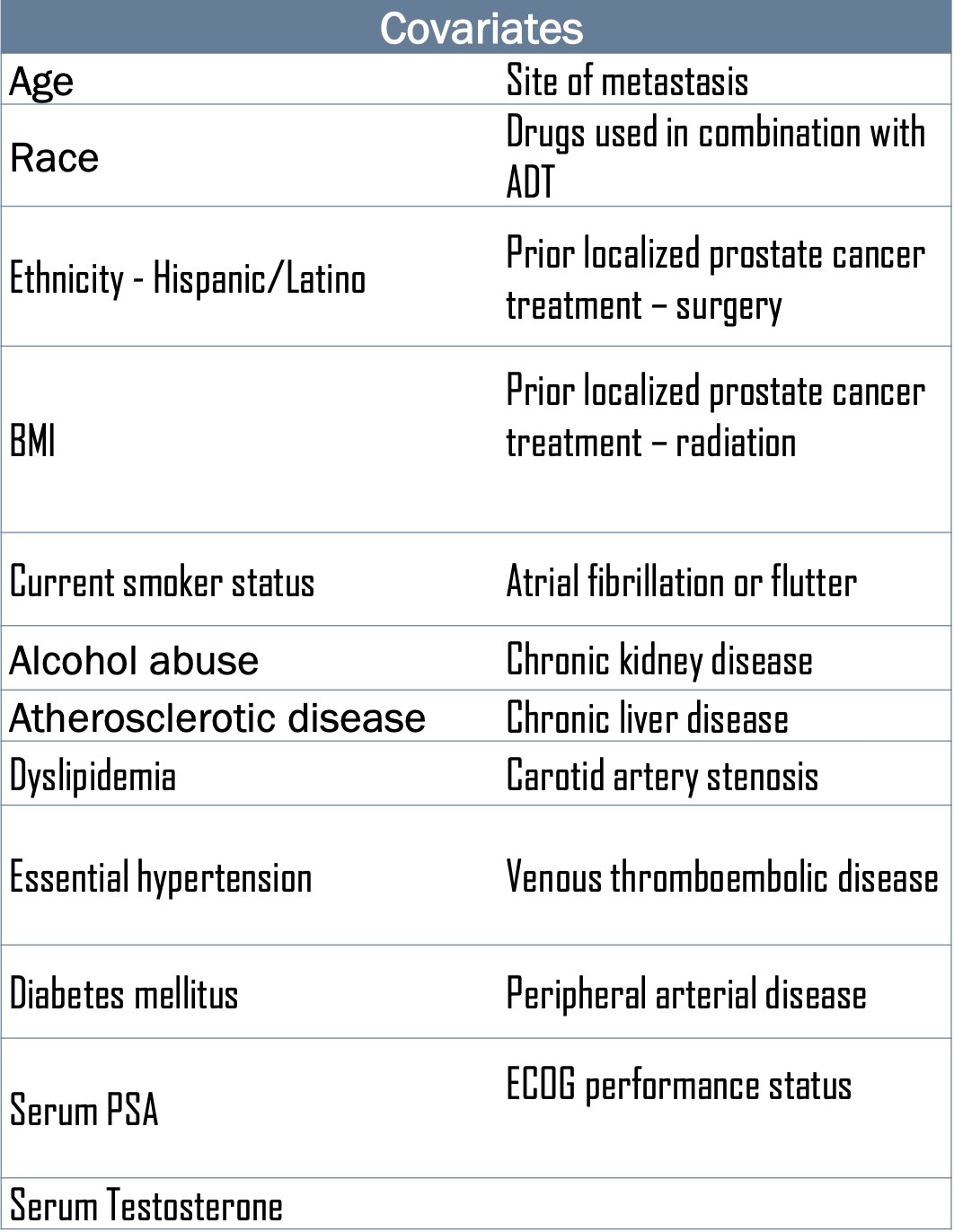
Additional antiandrogen treatments and prior surgical/radiation treatments were balanced for using propensity score matching with a 1:1 ratio between LHRH agonists and LHRH antagonist groups, a caliper of 0.25 SDs, and a standardized mean difference of 0.1 by nearest-neighbor greedy matching. Risk ratios (RR) and 95% confidence intervals were reported for the outcomes.
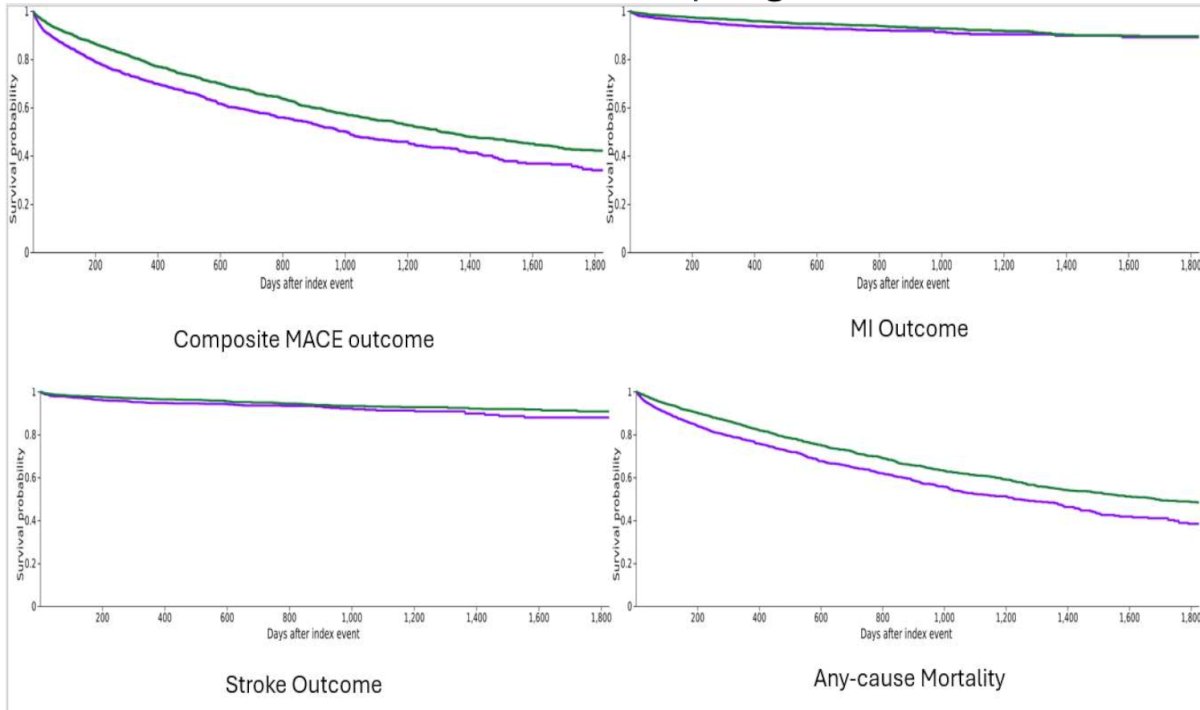
There were 32,816 mCSPC patients receiving ADT: 30,239 patients were on LHRH agonists and 2,577 patients were on LHRH antagonists. The mean duration of follow up after starting LHRH agonists and LHRH antagonists was 1,004.2 and 511.9 days, respectively. In LHRH agonists and LHRH antagonist groups, 7.6% versus 7.9% received abiraterone, 5.2% versus 5% received enzalutamide, 4.4% versus 4% received darolutamide, and 1.9% versus 1.9% received apalutamide, respectively. After propensity score matching, 2,566 patients in each group were compared and were well balanced for all covariates. Patients receiving LHRH agonists had a higher rate of major adverse cardiovascular events than those receiving LHRH antagonists (RR 1.35, 95% CI 1.22-1.49). Additionally, patients receiving LHRH agonists further had increased rates of stroke (RR 1.92, 95% CI 1.41-2.61), MI (RR 1.66, 95% CI 1.24-2.22), and death from any cause (RR 1.32, 95% CI 1.2-1.45):
Dr. Titus concluded his presentation discussing a comparison of cardiovascular events in patients with mCSPC treated with LHRH agonists to LHRH antagonists in the US with the following take home points:
- In a real-world, multi-center cohort, patients receiving LHRH agonists as compared to LHRH antagonists were found to be at 1.4 times higher risk of experiencing a major adverse cardiovascular event, driven by increased risks of MI, stroke, and death from any cause
- This evidence may help guide appropriate patient selection until prospective randomized clinical trials are conducted
Presented by: Renil Titus, Houston Methodist Hospital, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.
References: