(UroToday.com) The 2025 South Central AUA annual meeting included a session on prostate cancer, featuring a presentation from Dr. Abdul Qadar discussing a trial in progress, RENAPCA, a phase IB trial of relugolix and enzalutamide as neoadjuvant/adjuvant to local-regional treatment in patients with high-risk locally advanced prostate cancer. ADT is the backbone of treatment for patients with prostate cancer. Moreover, the combination of ADT with radiation therapy, other systemic therapy, or surgery may improve clinical outcome in patients with locally advanced and/or metastatic prostate cancer. ADT primarily involves medical or surgical castration and androgen receptor blockers, and studies indicate that combining medical castration with antiandrogens improves outcomes. In addition, a retrospective study showed patients with metastatic prostate cancer treated with GnRH antagonist plus androgen inhibitors had significantly longer PSA-based progression-free survival compared to those with GnRH agonist combination group (p < 0.01).
Ongoing trials are exploring new ADT combinations, such as an androgen receptor inhibitor with the GnRH analog abiraterone and prednisone (NCT02949284). However, no studies have assessed the combination of relugolix and enzalutamide. Relugolix, a selective GnRH receptor antagonist, offers faster and more complete testosterone suppression than leuprolide, with fewer cardiovascular side effects [1]. Enzalutamide, an FDA-approved androgen receptor inhibitor, is administered with a GnRH analog. This phase Ib trial evaluates the efficacy, safety, and biomarker response of relugolix and enzalutamide as neoadjuvant/adjuvant ADT in high-risk locally advanced prostate cancer patients undergoing radiation or radical surgery.
This trial is actively enrolling up to 46 patients across four sites over 2-3 years. Key eligibility criteria include:
- Male
- Aged 18 or older
- Histologically or radiologically confirmed high-risk locally advanced prostate adenocarcinoma
- Adequate organ and bone marrow function
- ECOG performance status of 0-2
- Agree to contraception if of reproductive potential
Patients with major comorbidities precluding therapy are excluded.
Patients will receive six months of neoadjuvant treatment with relugolix and enzalutamide, followed by 18 months of adjuvant therapy or until unacceptable toxicity. The median treatment duration is 24 months, with an additional 24-month follow-up for long-term efficacy and safety assessment:
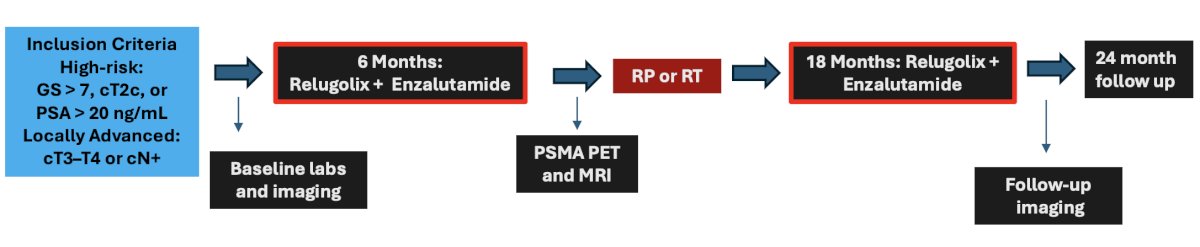
There will be two main cohorts: safety lead-in and dose expansion. In the safety lead-in cohort, the goal is to identify dose-limiting toxicities and determine the highest tolerable dose of the combination. In the dose expansion cohort, the focus is on evaluating the pathologic complete response and minimal residual disease rates after neoadjuvant ADT with relugolix and enzalutamide in patients who are candidates for radical prostatectomy. This study aims to optimize ADT strategies for high-risk locally advanced prostate cancer, potentially improving patient outcomes.
The current status of the trial is that it is open at the University of Oklahoma Stephenson Cancer Center and Banner MD Anderson Cancer Center in Phoenix, AZ. The safety lead in cohort has completed accrual, and complete study accrual is expected to be completed by 2028.
Presented by: Abdul Qadar, MD, University of Oklahoma Medical Center, Oklahoma City, OKWritten by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.
References: