(UroToday.com) The 2025 South Central AUA annual meeting included a session on prostate cancer, featuring a keynote lecture from Dr. Brian Chapin discussing salvage after failed local therapy. Dr. Chapin started his presentation by highlighting that the problem within the context of needing salvage therapies is that whether we treated patients with a radical prostatectomy or primary radiotherapy, there will be patients who have biochemical recurrence. Regardless of initial primary therapy, it is important as the urologist to be the quarterback for the patient and coordinate patient care. This includes:
- Counseling our patients as to what biochemical recurrence is
- Having multidisciplinary discussions/conferences
- Applying salvage procedures when appropriate
- Making referrals, if needed, for directed therapies or systemic therapy
- Resuming or identifying a new quarterback once treatment is completed
- Not overstepping our abilities: doing what we are comfortable with and doing it well
Part of providing transparency is discussing with the patient that there is a lack of data, the results are confounding, there are unknowns of applied therapies, there are risks of treatments, we need to be honest about the likelihood of success of treatments, and we must manage quality of life expectations.
With regards to definitions of biochemical recurrence, for post prostatectomy, this has generally been accepted as two consecutive PSA values > 0.2 ng/mL. After primary radiotherapy, in 1996, the Board of American Society for Therapeutic Radiology and Oncology committee convened to define a standard definition of PSA failure after external beam radiation. From the meeting came the definition of 3 consecutive PSA rises after the nadir with the date of failure being halfway between the nadir and first rise. At the ASTRO and RTOG meeting in Phoenix in 2005, some of the concerns with the ASTRO criteria were discussed including the failure rates of radiation being dependent on follow-up length, the problems and inherent biases of backdating, dealing with PSA bounce after treatment, and the definition’s lack of association with clinical progression. The consensus from this meeting was a statement, now referred to as the Phoenix definition, for biochemical recurrence after radiotherapy: PSA nadir + 2 ng/ml, and a date of failure “at call”.
Dr. Chapin then discussed the natural history of biochemical recurrence, highlighting the classic JAMA paper by Dr. Pound,1 which was a retrospective review of 1,997 men who underwent radical prostatectomy between 1982 and 1997. Of these men, 315 (15%) developed biochemical PSA level elevation, and 11 underwent early hormone therapy after the recurrence and were not included in the study. The 5-year metastatic progression free survival rate was 64% among 304 biochemical recurrence patients who were observed until metastatic progression:
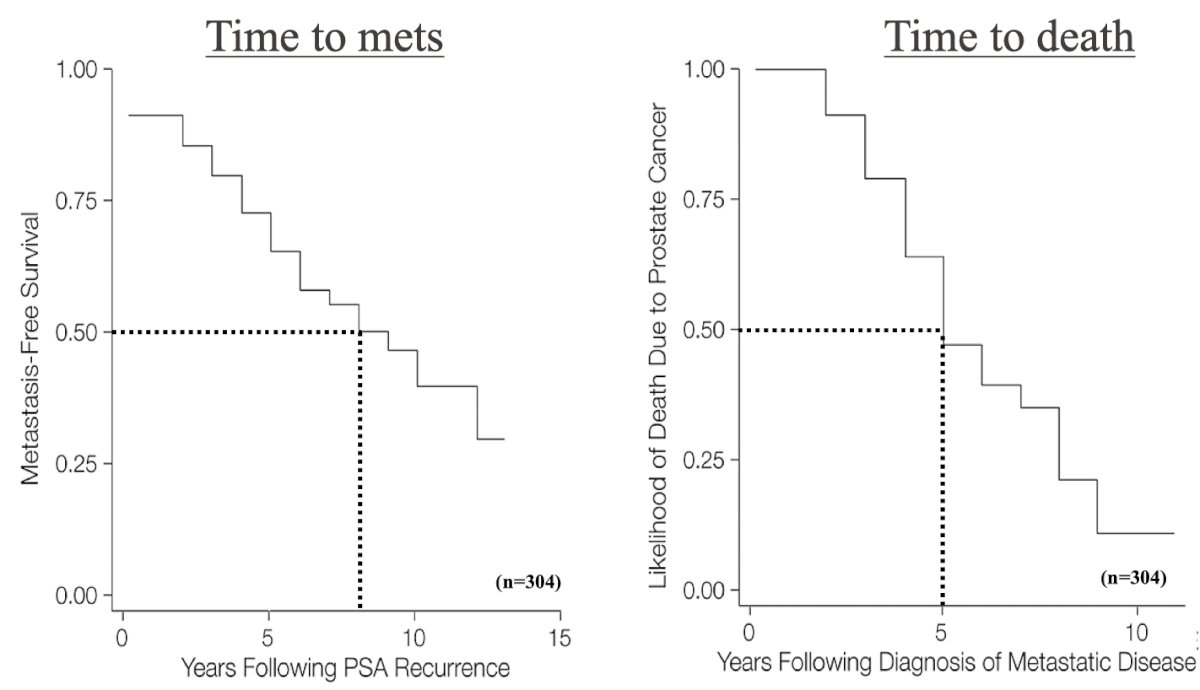
Ultimately, among patients with biochemical recurrence who developed metastatic disease (34%), with no hormone therapy prior to metastasis, the median was 8 years from biochemical recurrence to metastasis and a median of 5 years from metastasis to death.
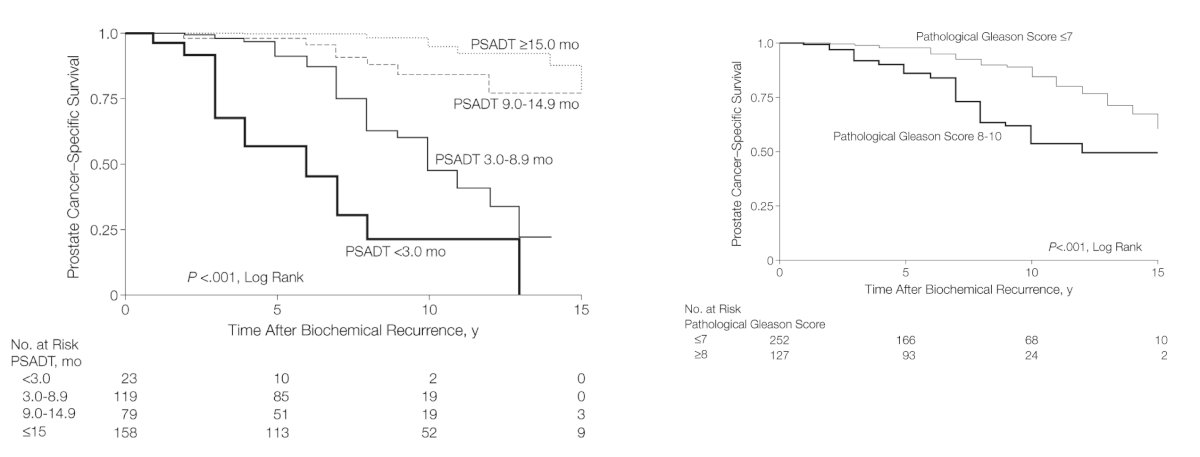
It has become clear that biochemical recurrence is a heterogeneous population of patients with variable prognoses. In addition to Gleason score and time from treatment to biochemical recurrence, PSA doubling time has emerged as a significant predictor of adverse outcomes in this patient population. In a cohort of 379 patients with biochemical recurrence following radical prostatectomy, those with a PSA doubling time <15 months accounted for 90% of all deaths. Significantly, shorter PSA doubling times were associated with progressively worse overall survival outcomes, with those having a PSA doubling time < 9 months having an almost 9-fold increase rate of mortality, compared to those with a PSA doubling time ≥15 months:2
However, there are many questions about how we should handle biochemical recurrence: Can we alter the disease course with an intervention? Is it possible to cure? Can we delay the time to systemic therapy? Can we prolong survival?
Dr. Chapin then discussed the work-up of biochemical recurrence, which should include the following:
- Prostate cancer history: timing, Gleason, PSA, comorbidities
- PSA kinetics: serial checks, PSA doubling time
- Prostate/pelvic MRI + PSMA PET/CT scan
- Prostate Biopsy: standard or fusion + seminal vesicles
- Discuss salvage options
PSMA PET/CT is the new standard for imaging patients with biochemical recurrence. However, there are several outstanding questions/issues with PSMA PET/CT, including (i) cost, (ii) insurance coverage (often recovers pre-approvals), (iii) questions about the timing of when to scan, and (iv) utility (better prognostication versus improved outcomes).
Most importantly, can next generation imaging improve patient outcomes? The EMPIRE-1 trial3 published in The Lancet in 2021 evaluated the role of 18F-fluciclovine-PET/CT in improving cancer control compared with conventional imaging (bone scan and either CT or MRI) alone for salvage post-prostatectomy radiotherapy. There were 165 patients randomly assigned in a 1:1 ratio to radiotherapy directed by conventional imaging alone or to conventional imaging plus 18F-fluciclovine-PET/CT:
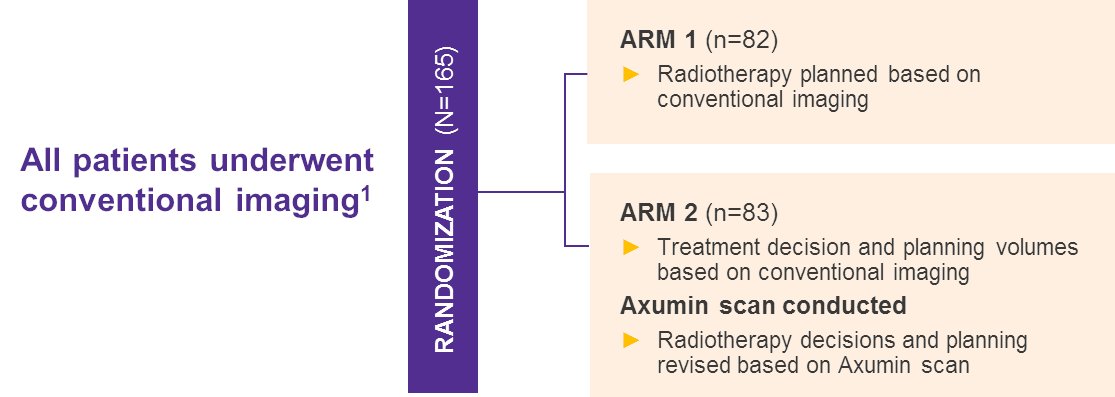
3-year event-free survival was 63.0% (95% CI 49.2-74.0) in the conventional imaging group versus 75.5% (95% CI 62.5-84.6) for 18F-fluciclovine-PET/CT (difference 12.5; 95% CI 4.3-20.8; HR 1.84, 95% CI 0.98-3.47, p = 0.0540). However, Dr. Chapin emphasized that the absence of PET-defined involvement does not equal proof of disease absence, and there is an unknown clinical significance of PET-detected disease lacking conventional imaging correlation.
Whether PET directed interventions alter disease biology is an important question, which Dr. Chapin acknowledges carries many assumptions. When evaluating a study, we should note:
- Standards should not change based on PSA endpoints
- Metastasis free survival is the only valid surrogate endpoint for overall survival
- A change in treatment plan alone is not a valid endpoint
- Without knowing if the change is beneficial
- Delaying time to systemic therapy is not a valid endpoint
- Is it due to a change in biology or a change in behavior?
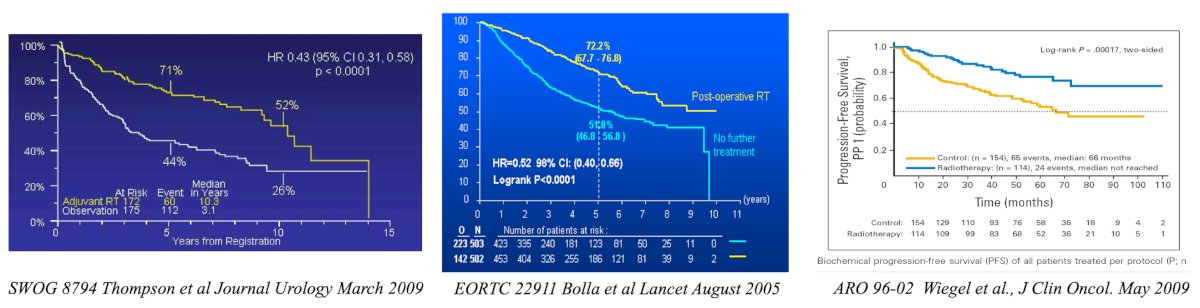
Next, Dr. Chapin discussed post-prostatectomy adjuvant versus salvage radiation therapy. The following European, German, and American trials were all very consistent in their results, demonstrating a ~50% decrease in the risk of biochemical recurrence with adjuvant radiotherapy over surgery alone:
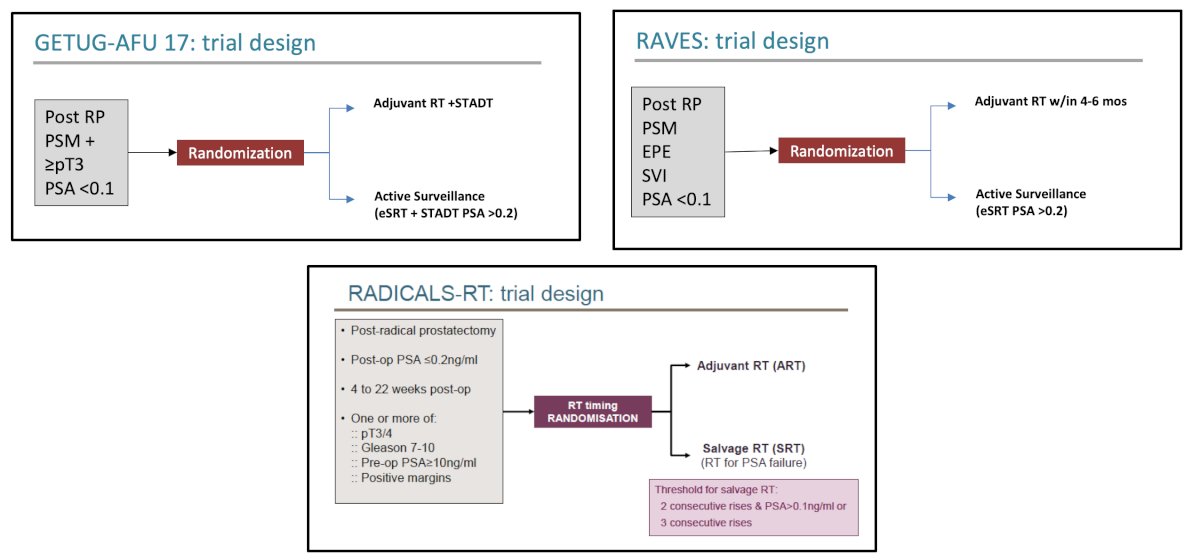
However, Dr. Chapin notes that utilization of adjuvant radiotherapy has been low, likely secondary to ~50% of patients not needing radiotherapy, and it was not known whether salvage radiotherapy, if given early, has similar efficacy to the adjuvant approach. Since these aforementioned early trials, we have seen 3 randomized trials published assessing the utility of adjuvant versus salvage radiation, including RADICALS-RT,4 GETUG-AFU 17,5 and RAVES:6
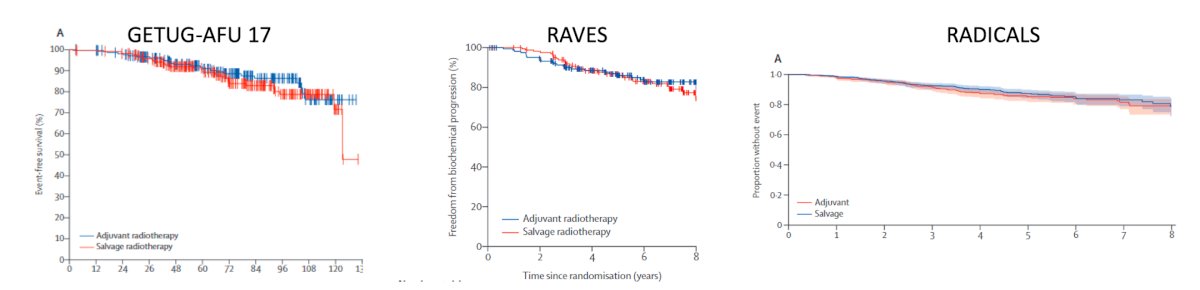
At a median follow-up of 4.9 years (IQR: 3.0 – 6.1) for 1,396 patients, the RADICALS-RT trial showed no differences were seen in the 5-year biochemical progression-free survival rates: 85% for adjuvant and 99% for salvage radiotherapy (HR 0.88, 95% CI 0.58 – 1.33, p = 0.53). At a median follow-up of 6.1 years in the RAVES trial, the 5-year freedom from biochemical progression was non-significantly different (adjuvant: 86% versus salvage: 87%; HR 1.12, 95% CI 0.65 – 1.90). Finally, in the GETUG-17 trial, at a median follow-up of 75 months, there was no significant difference in the primary study outcome of 5-year event-free survival: 92% (95% CI 86 – 95) in the adjuvant arm and 90% (95% CI 85 – 94%) in the early salvage arm (HR 0.81, 95% CI 0.48 – 1.36, log-rank p = 0.42):
Following the completion of these three trials, results from the pre-planned ARTISTIC analysis, which utilized a prospective framework for adaptive meta-analysis, were published.7 This meta-analysis utilized a harmonized definition of event-free survival, defined as the time from randomization until the first evidence of either biochemical progression (PSA ≥0.4 ng/mL and rising after completion of any postoperative radiotherapy), clinical or radiological progression, initiation of a non-trial treatment, death from prostate cancer, or a PSA level of at least 2.0 ng/mL at any time after randomization. With 1,075 patients included at a median follow-up of 60 to 78 months, this meta-analysis demonstrated no significant improvement in event-free survival with adjuvant radiotherapy compared to early salvage treatment (HR 0.95, 95% CI 0.75-1.21, p = 0.70):
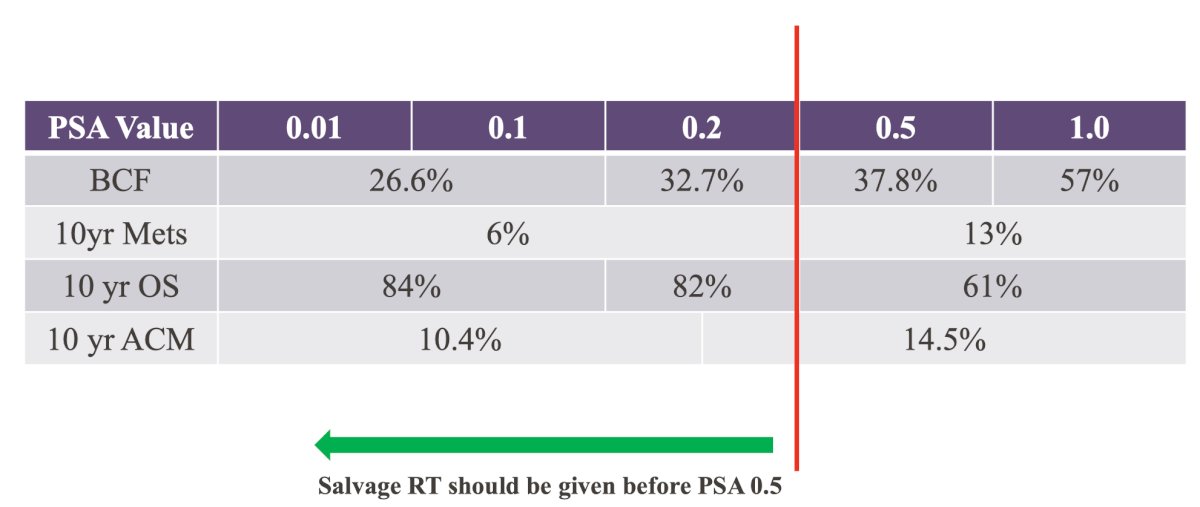
Based on these results, Dr. Chapin emphasized that the PSA threshold for salvage radiotherapy should be < 0.50 ng/mL:
Dr. Chapin also notes that there are several issues with the generalizability of these three randomized clinical trials: (i) the majority of patients had Gleason 7 disease, (ii) <20% had Gleason 8-10 or pT3b disease, and (iii) <5% had pathologic node positive disease.
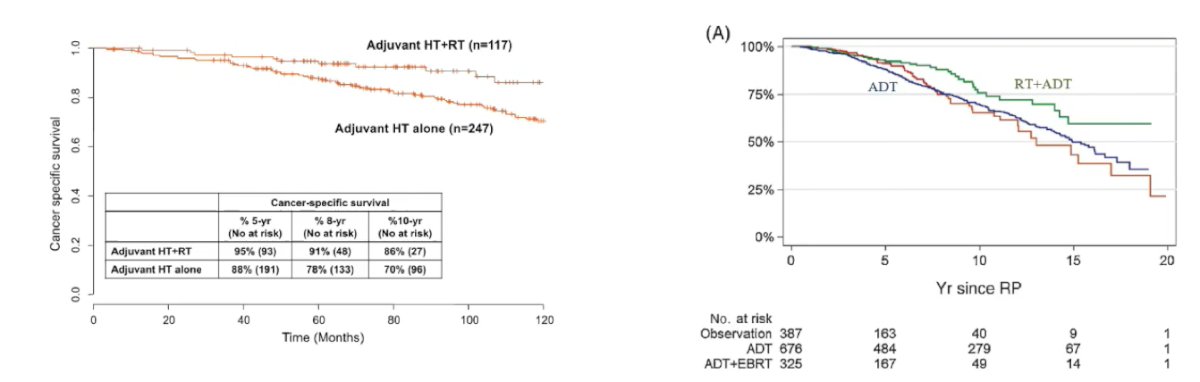
Is there any role for adjuvant radiotherapy? Work from Touijer et al.8 in 2018 evaluated the association between three different management strategies and survival in prostate cancer with lymph node metastasis after radical prostatectomy. Among 1,338 patients, ADT + external beam radiotherapy was associated with better overall survival than ADT alone (HR 0.46, 95% CI 0.32-0.66) or observation (HR 0.41, 95% CI 0.27-0.64). The 10-year mortality risk difference between ADT + external beam radiotherapy, observation, or ADT alone ranged from 5% in low-risk patients to 40% in high-risk patients. Adjuvant ADT + external beam radiotherapy was also associated with better cancer specific survival than observation or ADT alone (p<0.0001), and ADT had better cancer specific survival compared to observation (HR 0.64, 95% CI 0.43-0.95):
There are several salvage radiotherapy knowns and potential unknowns, including: Is salvage pelvic radiation effective in advanced patients? For patients with a negative PSMA PET/CT, there is a 78-85% PSA response in negative scans. For patients with pelvic N+ disease, Dr. Chapin states that there may be a benefit, with a ~55% response, which perhaps may improve with the addition of androgen receptor pathway inhibitor treatment intensification. Finally, for those with M1 disease, the benefit may be ~21-25%. Dr. Chapin provided his current PSMA/salvage radiotherapy recommendations, as follows:
- Post radical prostatectomy biochemical recurrence: trend the PSA and plan for salvage radiotherapy with a PSA <0.5 ng/mL
- Adjuvant radiotherapy consideration when there are pathologic N+ nodes or multiple high risk features
- Imaging when the PSA is 0.2 ng/mL (twice) with an MRI (assessing local recurrence) and PSMA PET/CT
- Salvage radiotherapy if the imaging is negative, including the prostatic fossa or pelvic N+, as needed
- Be the quarterback for the patient and their family: discuss the unknowns of salvage radiotherapy with PSMA PET/CT positive extra-pelvic disease
- Enroll in clinical trials whenever possible
Finally, Dr. Chapin discussed prostate therapy post-radiation and ablation. For patients with post radiotherapy biochemical recurrence evaluation, we must (i) determine comorbidities and discuss eligibility for treatment, (ii) perform a PSMA PET/CT and MRI of the prostate, (iii) perform a prostate biopsy (standard or fusion) to also include the seminal vesicles, and (iv) discuss salvage therapy options.
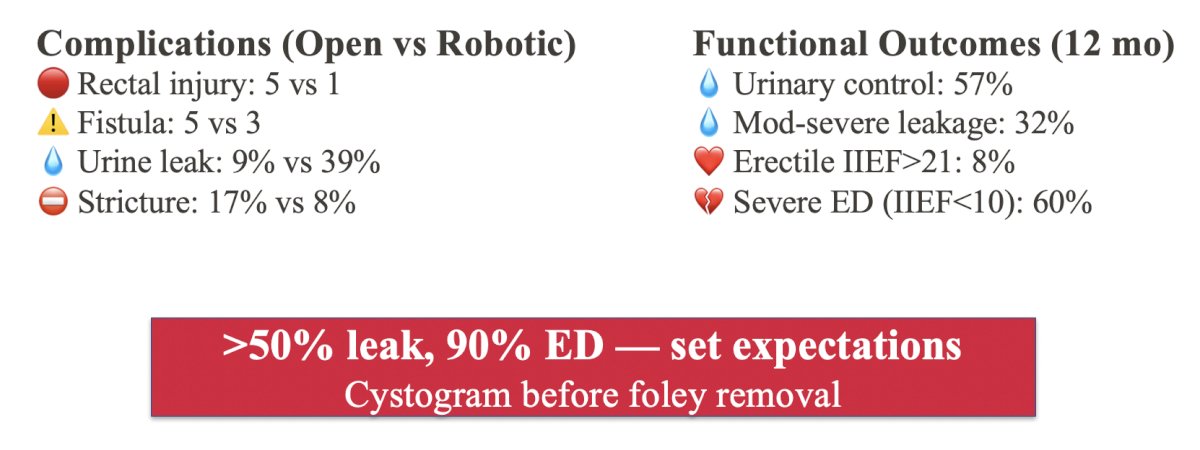
Salvage prostatectomy has historically been associated with a high complication rate, with most studies being retrospective in nature, with heterogeneous inclusion criteria. It is important that we provide our patients with realistic outcomes and strongly consider aborting surgical intervention if the pre-operative PSMA PET/CT is positive. There is currently no data that surgery improves outcomes in metastatic disease, and surgical risks become unacceptable in Dr. Chapin’s opinion. Generally, at 5 years, salvage prostatectomy is associated with a 50% biochemical recurrence free survival, 80% metastasis free survival, and 90% prostate cancer specific survival. Functional outcomes are also important to consider for patients undergoing a salvage prostatectomy, including the following:
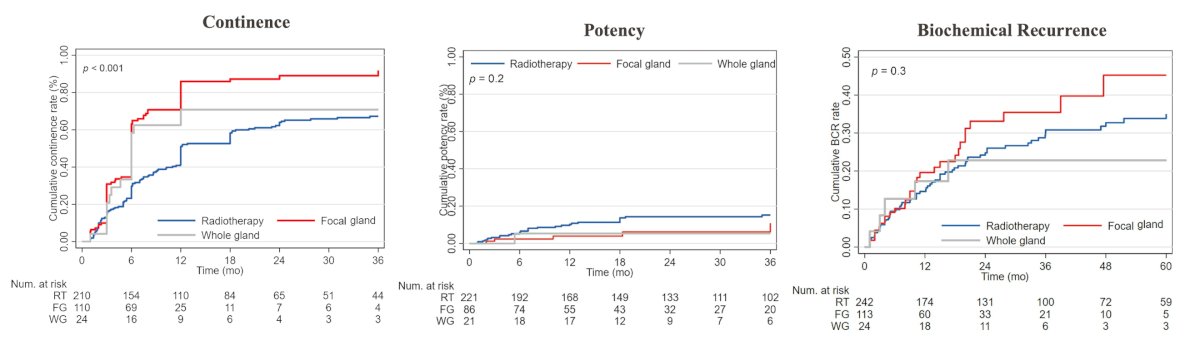
A recent 2025 study from Moschovas et al.9 reported a multicenter (9 centers) assessment of salvage robotic-assisted radical prostatectomy (RALP) outcomes. Overall, 397 patients who underwent salvage RALP from 2008 to 2023 were included and divided into three groups: primary radiation therapy, whole gland ablation, and focal gland ablation. The 5-year cumulative incidence rates of biochemical recurrence were 35%, 45%, and 23% for radiation therapy, focal gland ablation, and whole gland ablation, respectively (p = 0.3). The 3-year cumulative incidence rates of continence were 67%, 92%, and 71% for radiation therapy, focal gland ablation, and whole gland ablation, respectively (p < 0.001). Additionally, the 5-year cumulative incidence rates of potency were 16%, 11%, and 5.3% (p = 0.2), for radiation therapy, focal gland ablation, and whole gland ablation, respectively:
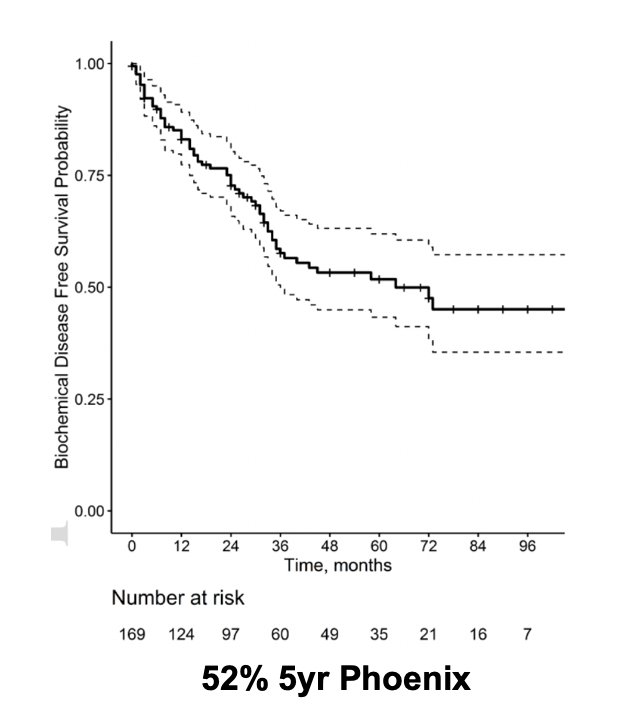
Dr. Chapin notes that there is limited data in the post primary ablation space, with mainly retrospective studies and inherent selection bias. Most studies claim acceptable oncologic and functional outcomes, but there are many anecdotes, and the challenges are real. For salvage cryotherapy post radiation, Exterkate et al.10 assessed 169 patients over a median follow-up of 36 months (IQR 18-66). Among this cohort, the biochemical recurrence free survival after 5 and 8 years was 52% (95% CI 43-62%) and 45% (95% CI 35-57%), respectively.
Overall, 19% of patients had new stress urinary incontinence, 92% had new erectile dysfunction, and 11 patients (6.5%) had a persistent urinary fistula.
Dr. Chapin concluded his presentation discussing salvage therapy after failed local therapy with the following take home messages:
- The natural history of biochemical recurrence is the absence of metastatic disease in ~60% of patients
- PSMA and MRI are recommended for assessing disease recurrence
- Adjuvant and salvage strategies should be individualized:
- Adjuvant therapy may still have a role in high-risk and pathologic N+ patients
- Post RP: consider early interventions when PSA <0.5 ng/mL (perhaps <0.3 ng/mL)
- Post radiotherapy salvage prostatectomy can be a challenge, and we should look for reasons not to operate
- Post radiotherapy salvage ablation is becoming a new standard
Presented by: Brian Chapin, MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.
References:
- Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA 1999 May 5;281(17):1591-1597.
- Freedland SJ, Humphreys EB, Mangold LA, et al. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA. 2005; 294(4):433–9.
- Jani AB, Schreibmann E, Goyal S, et al. 18F-fluciclovine-PET/CT imaging versus conventional imaging alone to guide postprostatectomy salvage radiotherapy for prostate cancer (EMPIRE-1): A single centre, open-label, phase 2/3 randomized controlled trial. Lancet. 2021 May 22;397(10288):1895-1904.
- Parker CC, Clarke NW, Cook AD, et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): A randomized, controlled phase 3 trial. Lancet 2020;396(10260):1413-1421.
- Sargos P, Chabaud S, Latorzeff I, et al. Adjuvant radiotherapy versus early salvage radiotherapy plus short-term androgen deprivation therapy in men with localized prostate cancer after radical prostatectomy (GETUG-AFU 17): A randomized, phase 3 trial. Lancet Oncol 2020;21(10):1341-1352.
- Kneebone A, Fraser-Browne C, Duchesne GM, et al. Adjuvant radiotherapy versus early salvage radiotherapy following radical prostatectomy (TROG 08.03/ANZUP RAVES): A randomized, controlled, phase 3, non-inferiority trial. Lancet Oncol. 2020;21(10):1331-1340.
- Vale CL, Fisher D, Kneebone A, et al. Adjuvant or early salvage radiotherapy for the treatment of localized and locally advanced prostate cancer: A prospectively planned systematic review and meta-analysis of aggregate data. Lancet 2020 Oct 31;396(10260):1422-1431.
- Touijer KA, Karnes RJ, Passoni N, et al. Survival Outcomes of Men with Lymph Node-positive prostate cancer after radical prostatectomy: A comparative analysis of different postoperative management strategies. Eur Urol. 2018 Jun; 73(6):890-896.
- Moschovas MC, Saikali S, Sandri M, et al. Outcomes of salvage robotic-assisted radical prostatectomy: High-volume multicentric data from the European Association of Urology Robotic Urology Section Scientific Working Group. Eur Urol. 2025 Jul;88(1):103-113.
- Exterkate L, Peters M, Somford DM, et al. Functional and oncological outcomes of salvage cryosurgery for radiorecurrent prostate cancer. BJU Int. 2021 Jul;128(1):46-56.