(UroToday.com) The 2025 South Central AUA annual meeting included a session on kidney cancer, featuring a presentation from Merrick Huang discussing patient decision making and treatment preferences for localized renal masses. The incidence of renal masses is rising, with over 80,000 new kidney and renal pelvis cancer cases estimated in 2024, and up to 70% detected incidentally.
Management options include active surveillance, renal mass biopsy, and surgical/ablative treatments, each with distinct risks and benefits. A new renal mass diagnosis can cause significant anxiety about prognosis, treatment options, complications, and financial burden. Despite increasing cases, patient-centered research on treatment decision factors remains limited, and no standardized questionnaires exist to assess these considerations. This study examined factors influencing treatment decisions in patients with newly diagnosed localized renal tumors to improve patient-centered care and guide future research.
A prospective survey was independently conducted among newly diagnosed renal mass patients following their urological consultation. Of the 67 patients approached, 41 completed an internally developed questionnaire consisting of 20 items assessing decision-making factors (ie. cost, hospitalization, tumor removal desire, complications, and kidney failure risk) and willingness to undergo renal mass biopsy or consider hypothetical tumor downsizing with neoadjuvant systemic therapy. Descriptive statistics and comparative analyses (ie. Friedman and chi-squared tests) were used to evaluate associations between patient preferences and decision-making factors.
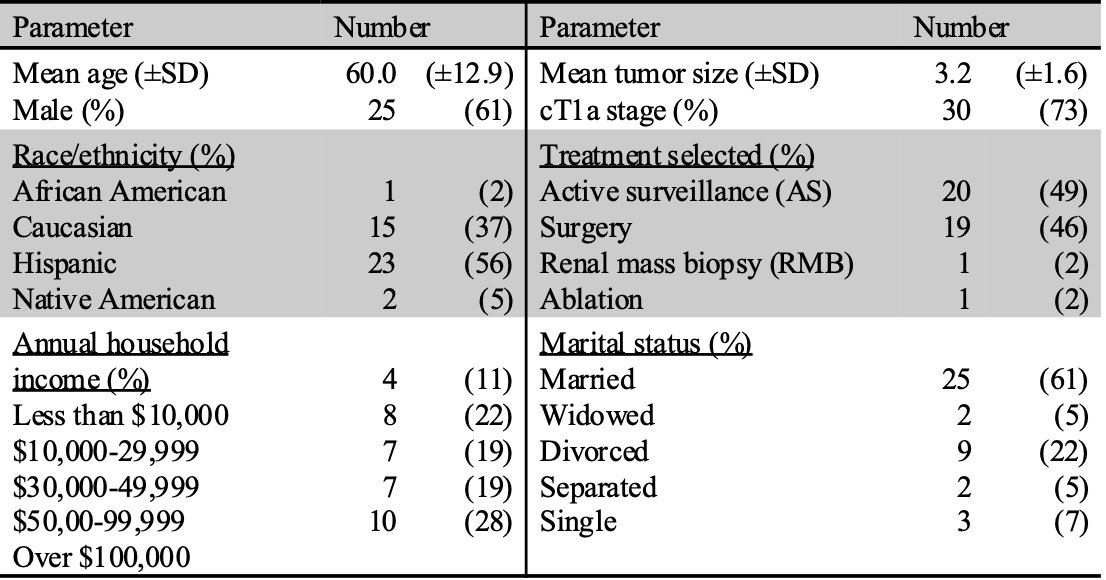
The patient demographic information is noted in the following table:
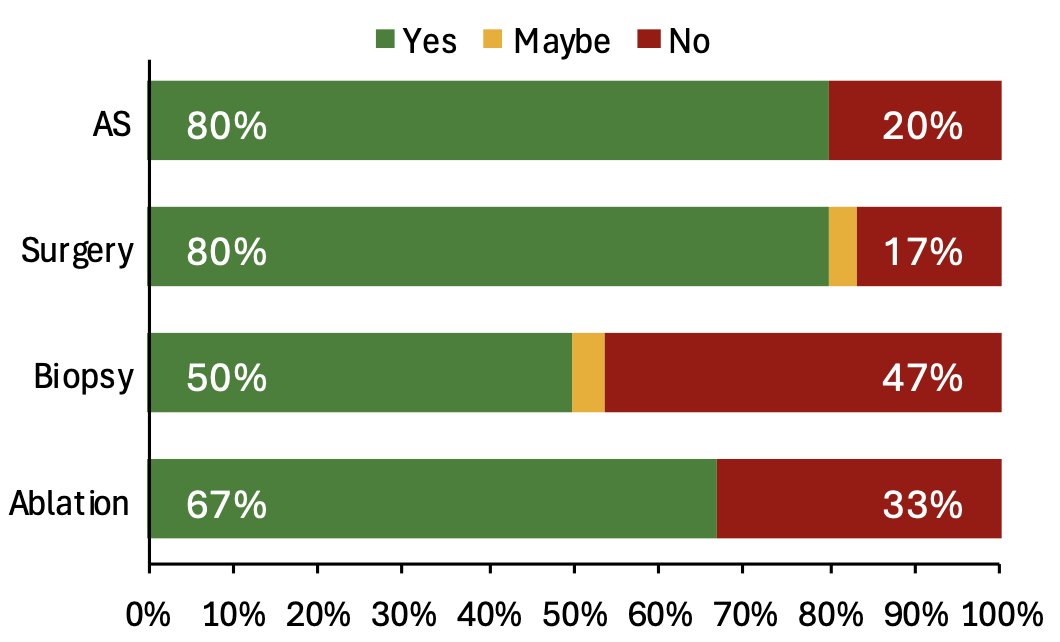
Among cT1a patients, 80% were counseled on active surveillance and surgery, 67% were counseled on ablation, but only 50% were informed about renal mass biopsy:
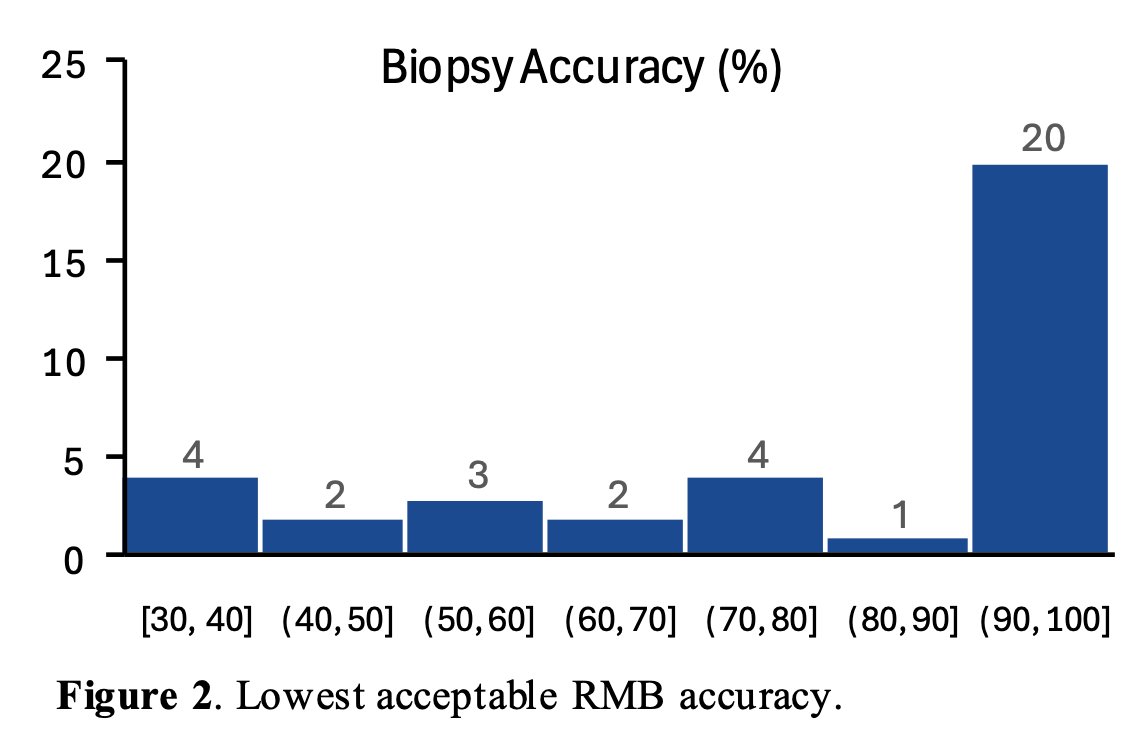
Over half (58%) would decline renal mass biopsy if accuracy were below 95%, and 39% would refuse renal mass biopsy irrespective of accuracy:
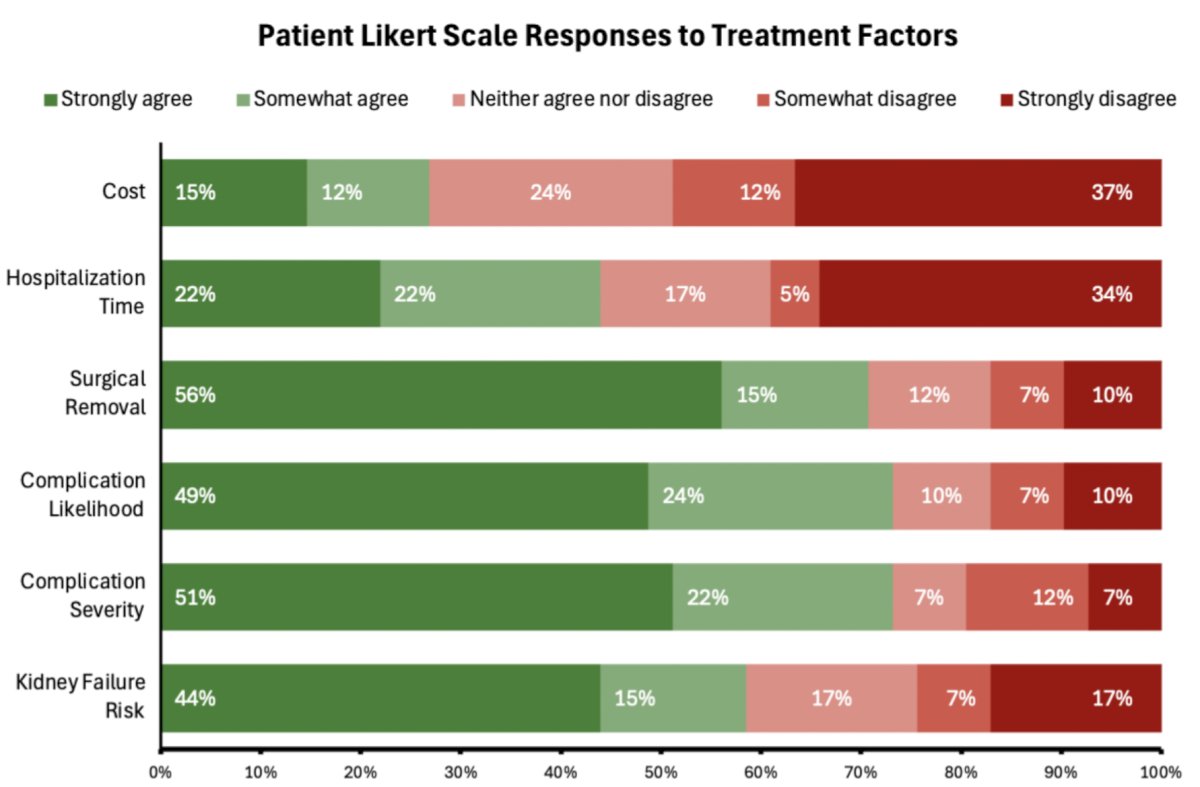
Patients prioritized treatment complications and kidney failure risk over cost and hospitalization considerations (p < 0.05). A majority (71%) strongly valued surgical excision, with 62% expressing low concern for recurrence:
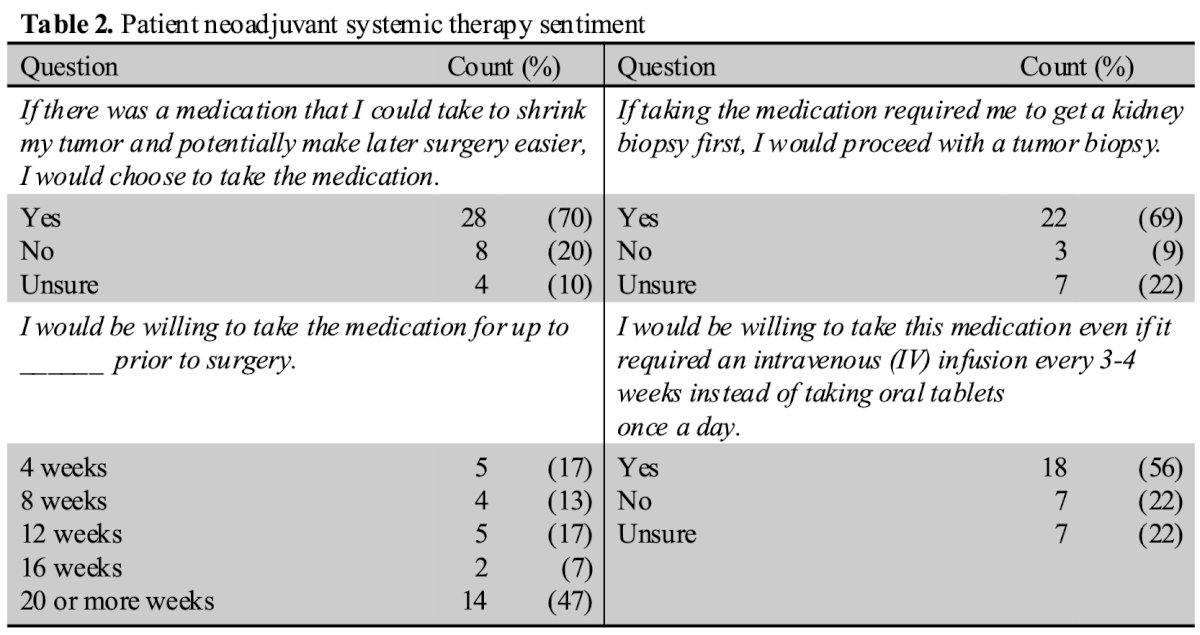
Neoadjuvant systemic therapy was acceptable to 70% of patients, with 69% of those willing to undergo renal mass biopsy first. While 52% would consider neoadjuvant systemic therapy for ≥16 weeks and 56% with intravenous administration, acceptance declined with potential lifelong side effects (48%):
Merrick Huang concluded this presentation discussing patient decision making and treatment preferences for localized renal masses with the following take-home points:
- Patients with renal masses prioritize tumor removal, but have significant concerns about complications and kidney failure
- Hesitation toward renal mass biopsy highlights the need for better patient education on its safety, value, and potential role
- The strong interest in neoadjuvant therapies supports further research on their role in renal mass treatment, aligning with patient preferences and improving shared decision-making
- Decision aids may assist patients when deciding between treatment options for cT1a masses
- This study emphasizes the importance of patient-centered counseling in renal mass management, and future research should address misconceptions about renal mass biopsy, explore strategies to improve patient education, and further evaluate neoadjuvant therapy’s role in localized renal cancer
- Clinical trials should assess neoadjuvant therapy’s oncologic benefits and patient tolerance to refine treatment protocols
Presented by: Merrick Huang, PhD, The University of Texas Health Science Center at San Antonio, San Antonio, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.