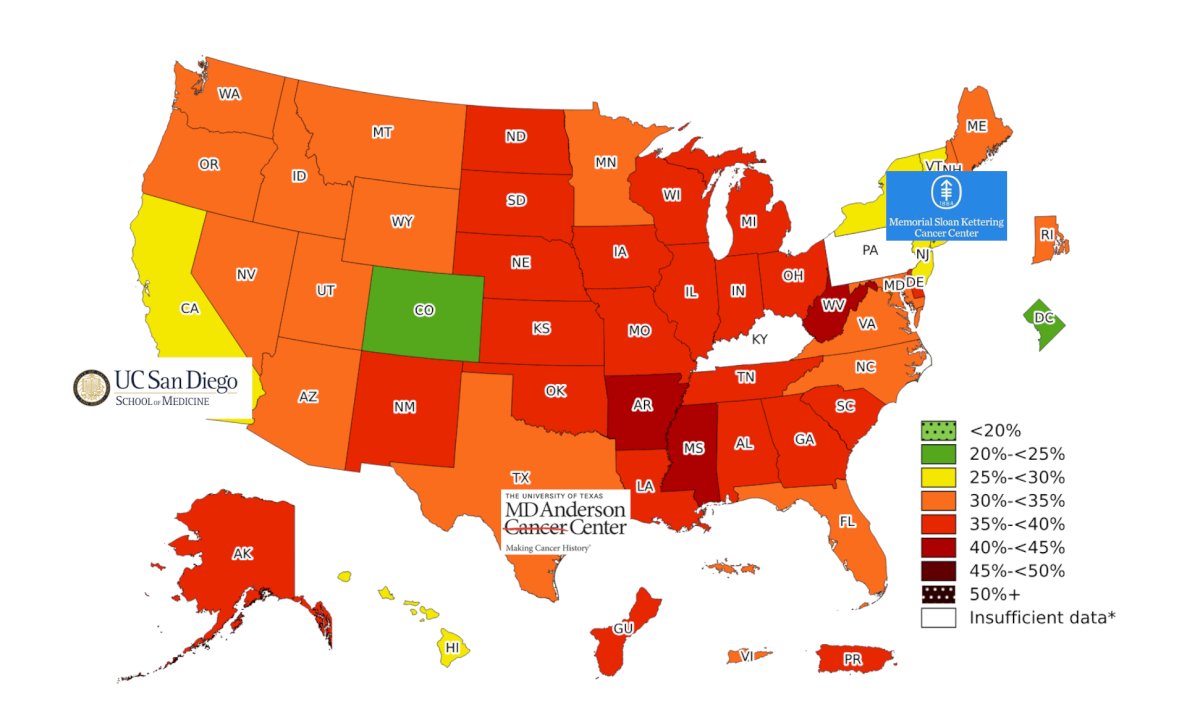
(UroToday.com) The 2025 South Central AUA annual meeting included a session on kidney cancer, featuring a presentation from Dr. Brittney Cotta discussing techniques for surgical treatment of RCC with morbidly obese patients. Dr. Cotta started her presentation by highlighting the CDC’s current map of obesity rates across the United States:
When considering a robotic nephrectomy for patients, a surgeon has to take into account the management of the subcutaneous fat, as well as the visceral fat. For subcutaneous fat in obese patients, there are some challenges, such as patient positioning, insufflation, and port placement. However, even though the subcutaneous fat may be challenging, there is typically less perinephric fat in women, leading to an easier nephrectomy. With regards to visceral fat, this can be “toxic fat”, leading to more difficult kidney mobilization and tumor defatting. Insufflation is typically not affected, as there is less thick tissue for port placement, and there is generally adequate room for robotic working space.
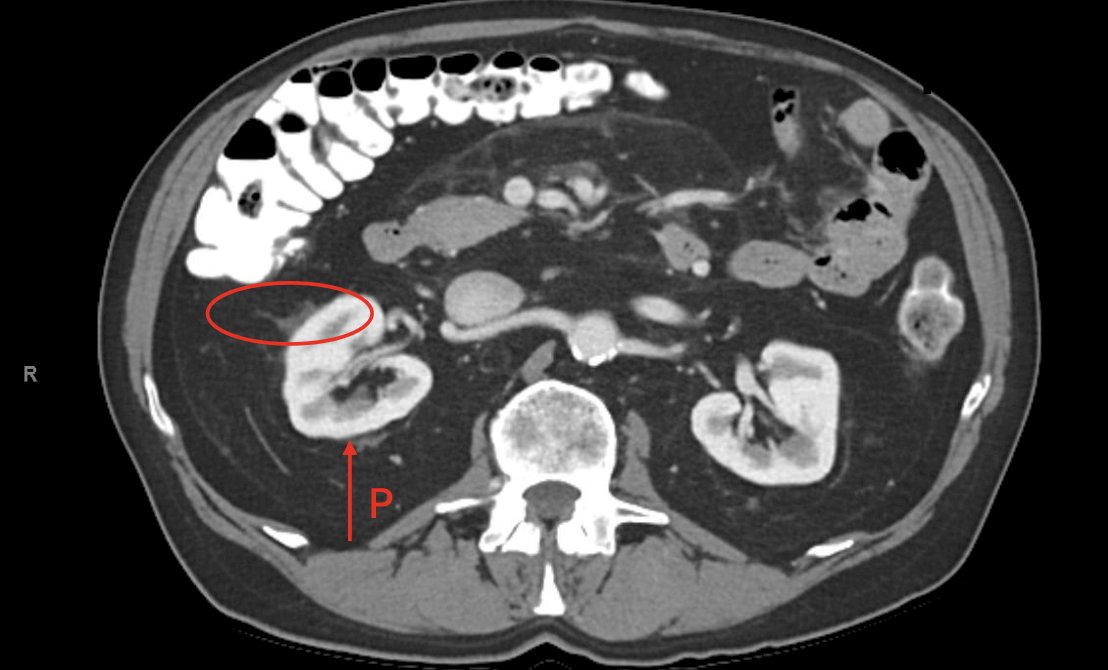
Dr. Cotta then discussed Case #1 of a 66 year old female, 5’6”, 273 pounds (BMI 44 kg/m2), with a right renal mass. The following CT scan demonstrates extensive subcutaneous fat and very little visceral or perinephric fat, which is typical in obese women:

Case #2 was a 75 year old male, 6’2”, 284 pounds (BMI 35.7 kg/m2), with a left small renal mass. This patient has very little subcutaneous fat, but extensive visceral and perinephric fat:

Finally, the third case presented by Dr. Cotta was a 58 year old female, 5’6”, 379 pounds (BMI 61 kg/m2), with a right renal mass and extensive subcutaneous and visceral fat:

BMI may not always be predictive of fat distribution. For example, this CT is of a 78 year old male, with a BMI of 26 kg/m2 and extensive visceral and perinephric fat, despite a low BMI:
Dr. Cotta then discussed the Mayo Adhesive Probability Score, which is an accurate image-based scoring system that predicts adherent perinephric fat for patients undergoing partial nephrectomy.1 Generally, posterior perinephric fat thickness and stranding are most predictive of adherent perinephric fat.
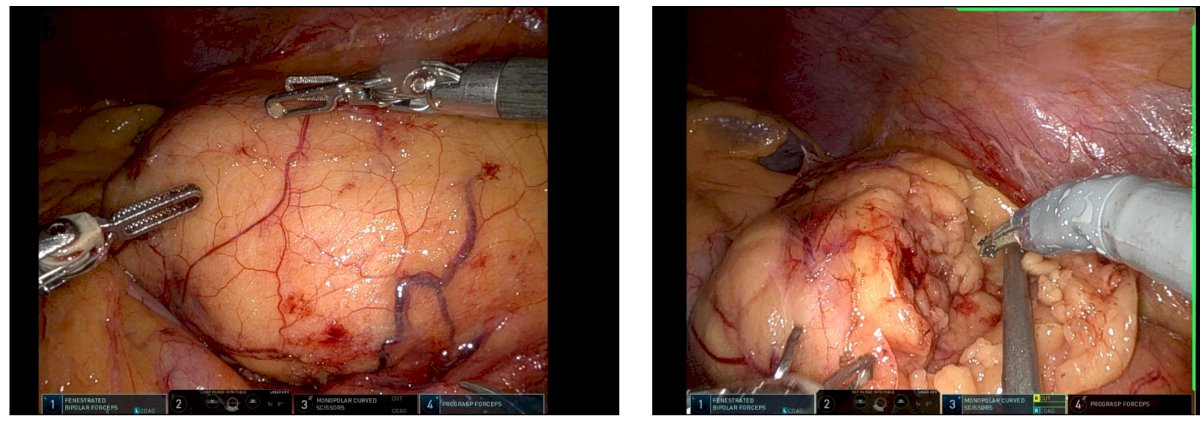
For obese patients, proper positioning of the patient is extremely important. This includes sufficient padding, multiple tape rolls, padding under the belly, and pre-marking the abdominal midline while the patient is still supine. Also important is robotic port placement. This includes a more lateral port placement on obese patients, with the assistant port off the midline to reach the intra-abdominal working area around the kidney. For a right sided nephrectomy, it is often helpful to have an additional port for a liver retractor, as well as a bariatric trocar for a 4th arm in patients with a large amount of subcutaneous fat (usually not necessary with visceral fat only). The following images show representative techniques for de-fatting the kidney in an obese patient for a robotic partial nephrectomy
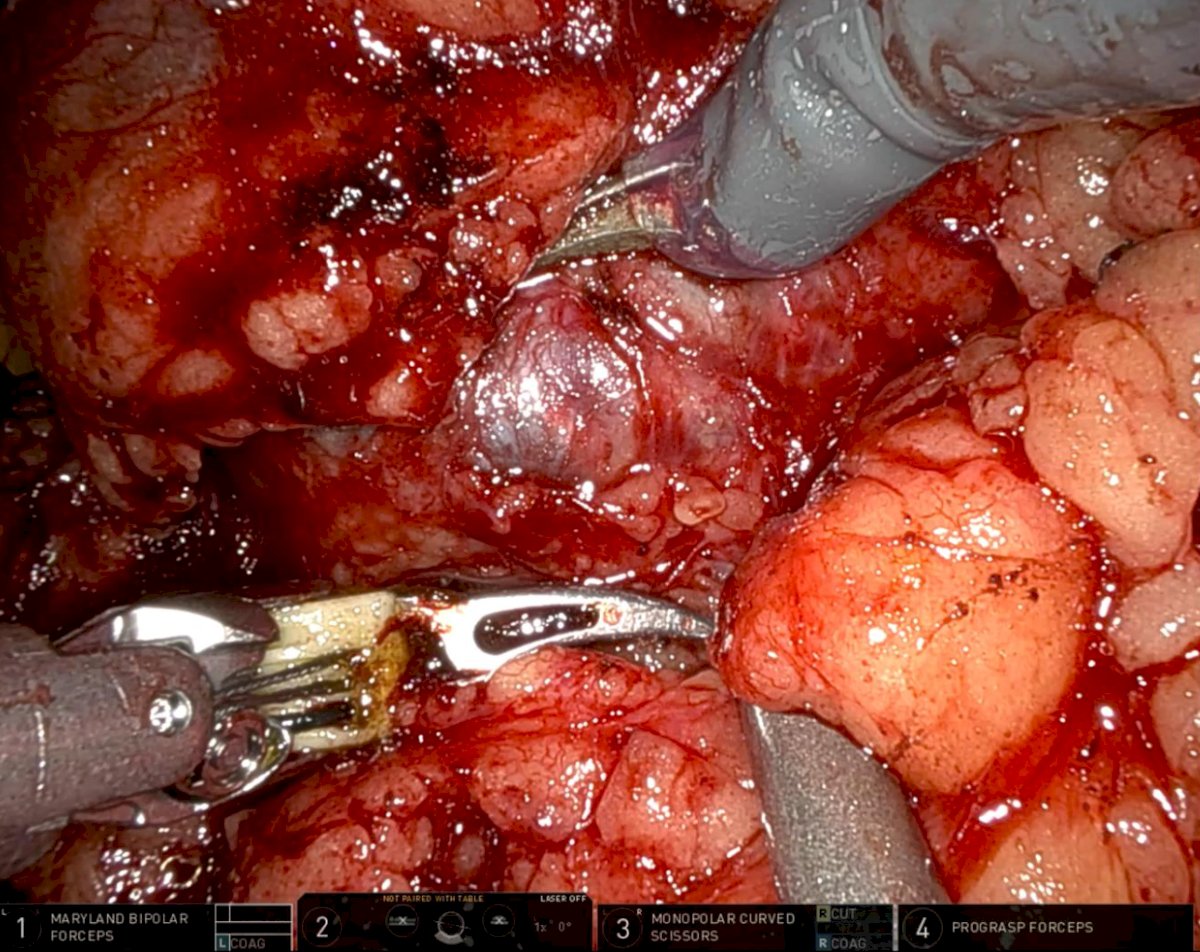
And finding the renal capsule:
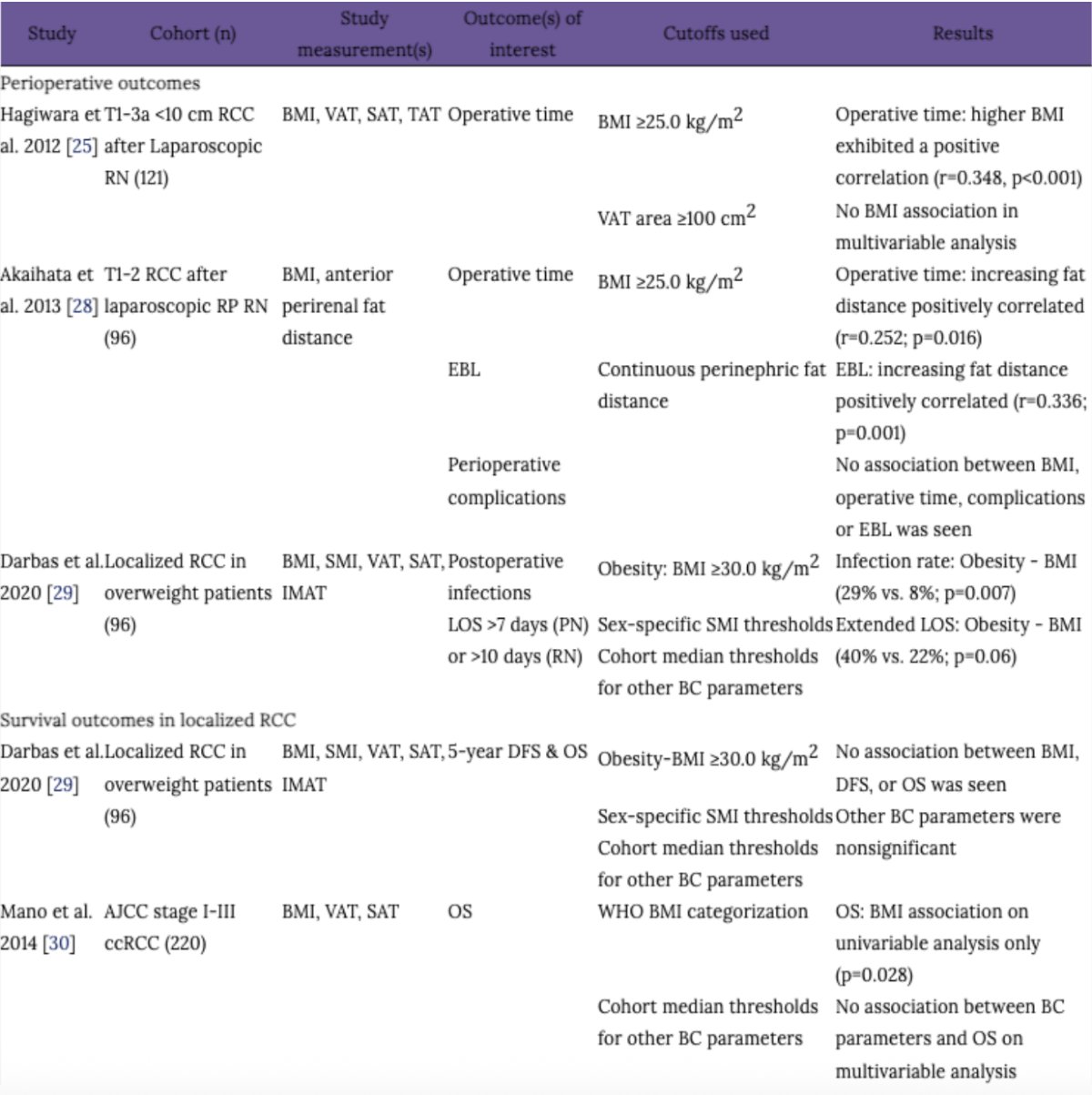
Dr. Cotta concluded her presentation discussing techniques for surgical treatment of RCC with morbidly obese patients by highlighting a review article assessing outcomes for obese patients undergoing a nephrectomy.2 Generally, these procedures are associated with longer operative room times, increased blood loss with more perinephric fat, higher rates of infection, but no association with survival when compared to non obese patients:
Presented by: Brittney Cotta, MD, MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.
References:
- Davidiuk AJ, Parker AS, Thomas CS, et al. Mayo adhesive probability score: an accurate image-based scoring system to predict adherent perinephric fat in partial nephrectomy. Eur Urol. 2014 Dec;66(6):1165-1171.
- Nicaise EH, Schmeusser BN, Shah YB, et al. Influence of body composition on the perioperative and survival outcomes of renal cell carcinoma. J Urol Oncol. 2023;21(3):193-199.