(UroToday.com) The 2025 South Central AUA annual meeting included a session on kidney cancer, featuring a keynote lecture from Dr. Robert Uzzo discussing when to start and when to stop active surveillance for localized kidney cancer. Dr. Uzzo started his presentation by noting the following statements regarding the safety of an initial period of active surveillance for patients:
- <2 cm renal mass, localized, in a patient with comorbid conditions: almost always
- >4 cm renal mass in a healthy patient: almost never
- In between the above criteria: most of the time
With regards to offering an initial course of active surveillance for small renal masses < 3 cm (with delayed intervention options), Dr. Uzzo provided the following table based on several criteria:
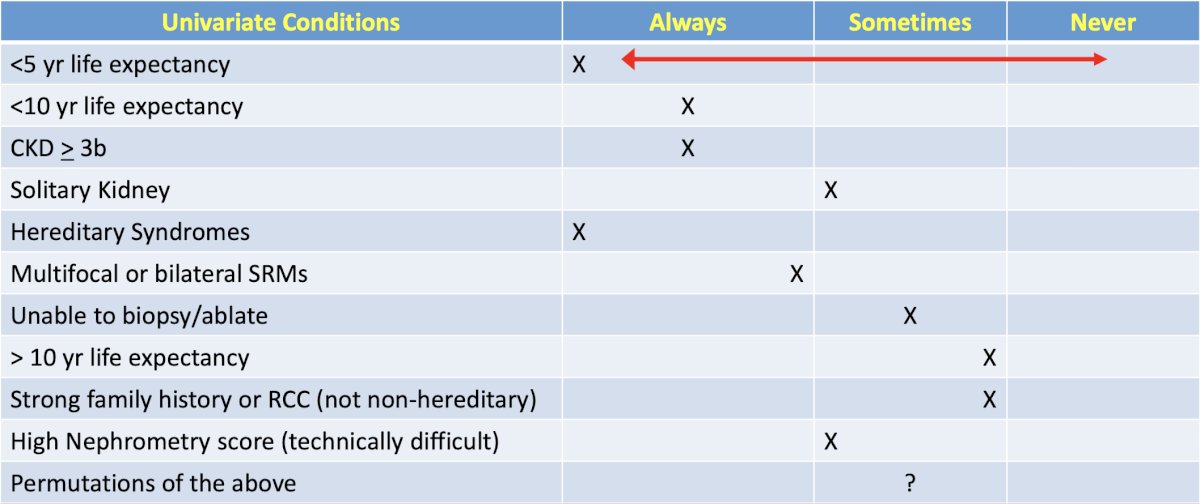
However, the decision making in the real world is difficult and made under multivariable conditions.
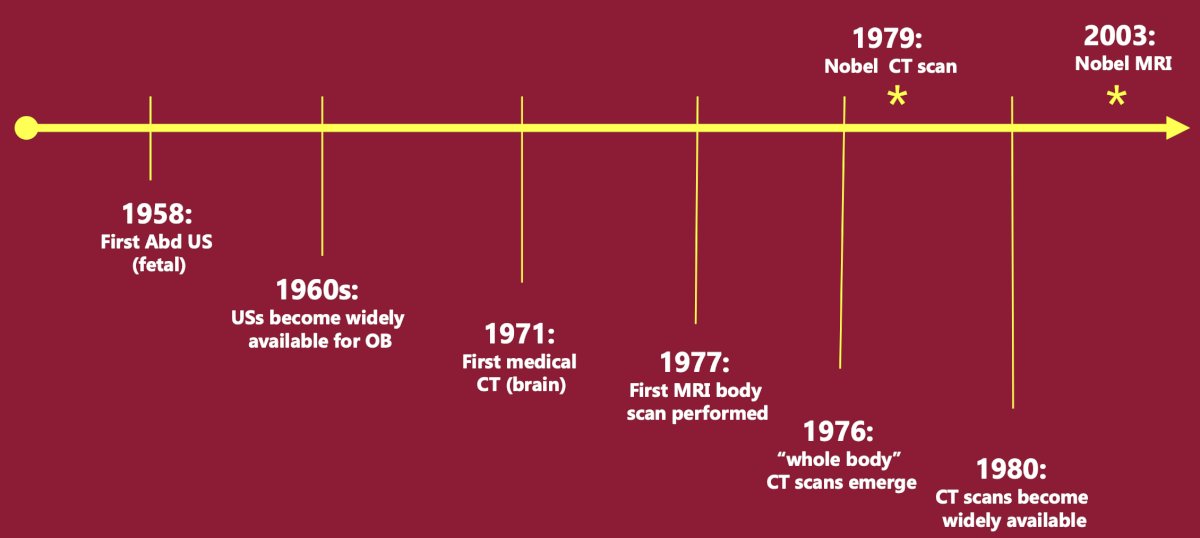
Historically, Dr. Uzzo discussed the evolution of the small renal mass, starting with the first fetal abdominal ultrasound in 1958 through the utilization of MRI in 2003:
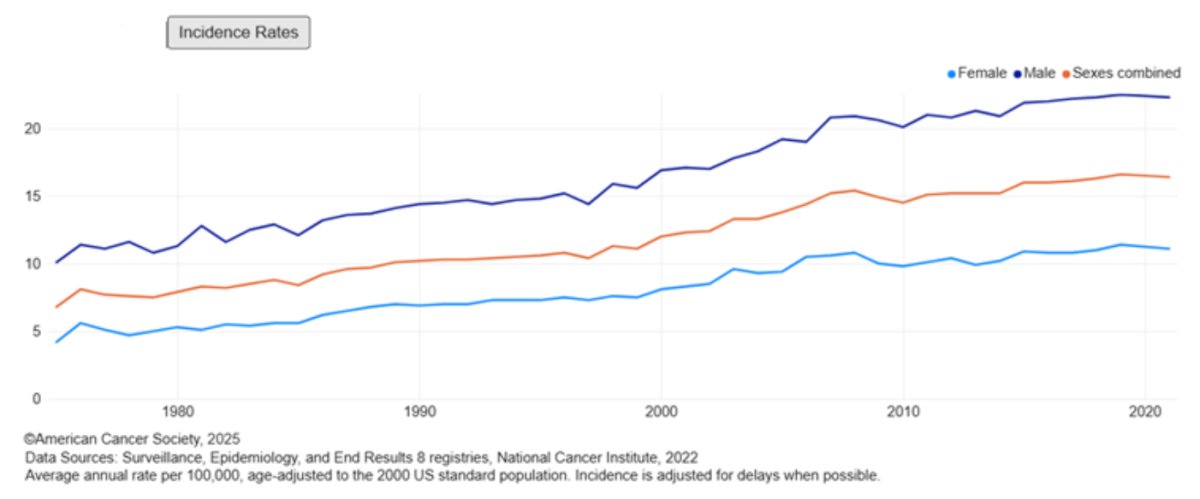
Secondary to increased utilization of cross sectional imaging, the incidence rates, according to the American Cancer Society, have steadily increased from 1980 to 2020:
During this time frame, there has also been an evolution of treatment for small renal masses, from radical nephrectomy for all patients (1950-1980), to partial nephrectomy (1990-2000), to minimally invasive approaches and active surveillance (2000s):
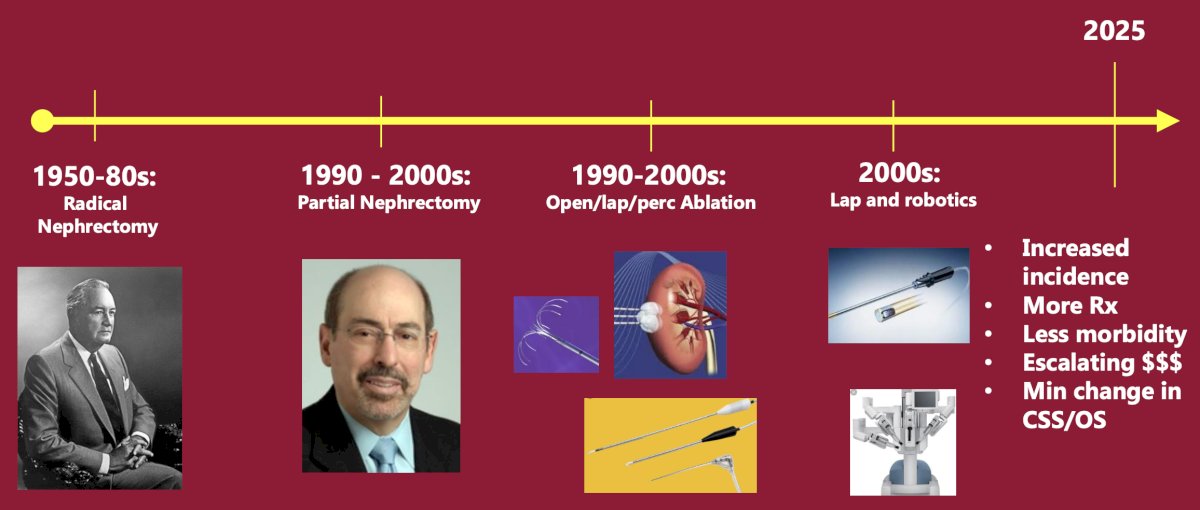
Ultimately, Dr. Uzzo emphasized that technologies evolved to “fix it” (removing the kidney and renal mass), without knowing if “fixing it” was necessary – what he calls “Drinking the Halstedian Kool-Aid.” The effects on early detection of small renal masses and improved survival, to date, are unclear.
Looking at 40 year trends in management of small renal masses, we are finding more masses more often because of increased use of CT, ultrasound, and MRI imaging, and we are removing small renal masses better and safer with:
- Organ preservation and improved reconstruction techniques
- Increased use of minimally invasive surgical approaches and decreased length of stay
- Decreased adverse events
Since 2008, the renal mass guideline landscape has continued to evolve, with many review articles and guideline contributions from the AUA, EAU, NCCN, and ASCO:
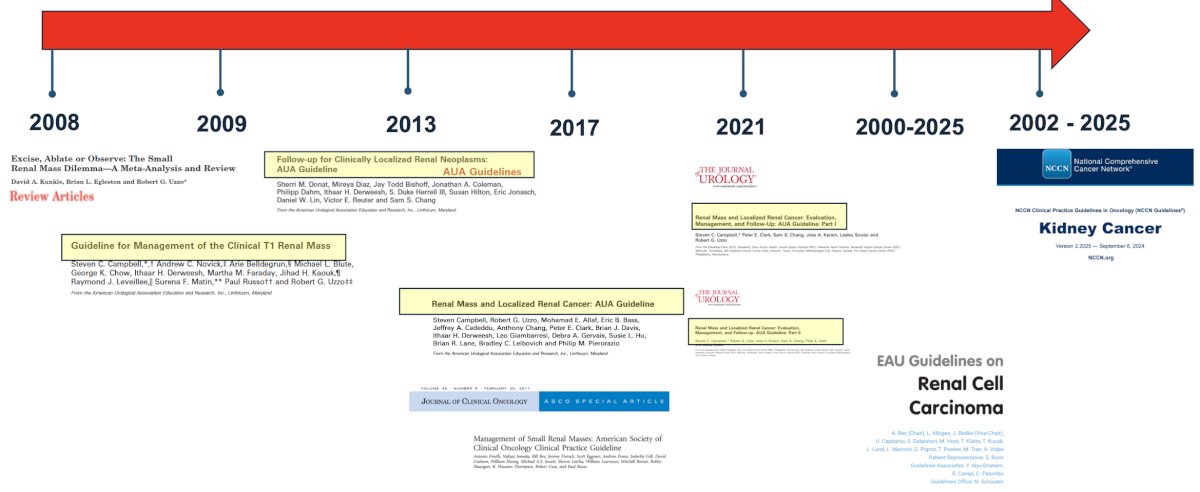
Generally, Dr. Uzzo notes that the guidelines are all pretty consistent for recommending active surveillance, which he states is a major shift since his own surgical training.
Dr. Uzzo then presented Case #1 of a 62 year old male with a medical history complicated by Crohn’s disease and an incidence finding of a right 1.5 cm enhancing renal mass:
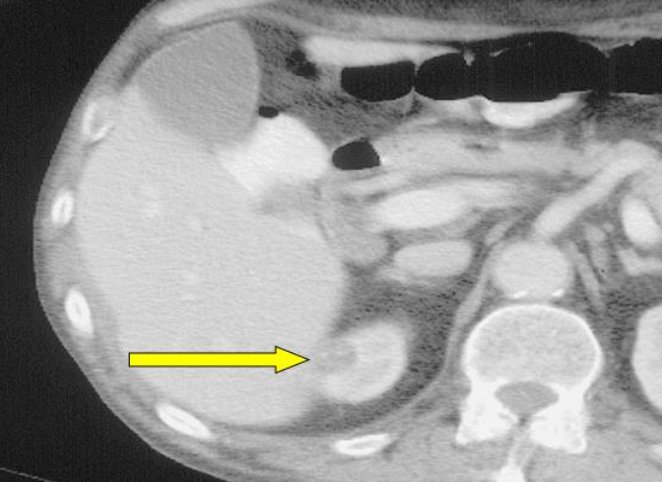
Additional medical history included stable angina, COPD, CVA, and hypertension, as well as a 1 pack per day smoking history. His pertinent medications included daily prednisone, and his performance status was ECOG 1-2. His eGFR was 54 cc/min, and he had a normal contralateral kidney. After discussing treatment options, this patient elected for active surveillance.
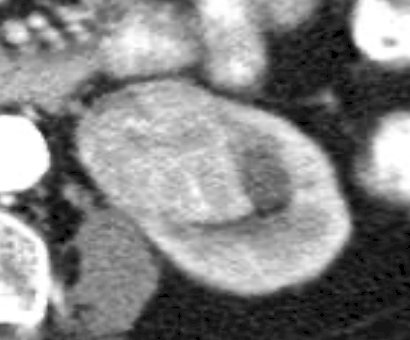
Case #2 was a 77 year old male with an incidental right 2.0 cm enhancing renal mass:
This patient had a history of hypertension secondary to renal artery stenosis, coronary artery disease, and non-insulin dependent diabetes mellitus. His surgical history was notable for coronary artery bypass grafting with stents, his performance status was ECOG 0, and his eGFR was 45 cc/min. A renal function study noted 58% function for the right kidney and 42% function for the left kidney. After discussion of treatment options, this patient also elected for a period of active surveillance.
Based on the AUA 2021 guidelines for renal masses and localized renal cancer, statement #5 states that “clinicians should provide counselling for cT1a tumors, and the low oncologic risk of many small renal masses should be reviewed (Clinical Principle) [1]. As part of counselling, Dr. Uzzo noted that preoperative imaging cannot predict tumor biology, specifically benign versus malignant or indolent versus aggressive disease. However, size, tumor complexity and enhancement patterns are the most helpful for predicting RCC: (i) at 1 cm in size, a small renal mass is likely to be benign in 40% of cases, but only in 6% of cases for tumors > 7 cm, and (ii) males are more likely than females to have RCC, although RCC still predominates small renal masses in both genders. Importantly, many cT1a tumors have a low oncologic risk. In retrospective, extirpative surgical series, almost no patients with a tumor < 2 cm presented with metastatic RCC, and <2% of patients with tumors <= 4 cm presented with or developed metastatic disease when observed for a median of 36 months.
Statement #29 of the AUA guidelines states, “for patients with solid renal masses < 2 cm, or those that are predominantly cystic, clinicians may elect for active surveillance with potential for delayed intervention for the initial management (Conditional Recommendation; Evidence Level: Grade C).” Dr. Uzzo notes that active surveillance is a safe and effective option for selected patients who have been properly informed. In the published active surveillance literature, in patients > 70 years of age (average mass size 2 cm, follow-up 12-36 months), cancer specific survival and metastasis specific survival rates are 98-100%. Oncologic risks are also particularly low for masses < 2 cm, and active surveillance is an acceptable option for the initial management of all patients, not just for those with limited life expectancy or poor performance status.
Statement #6 of the AUA guidelines states, “during counseling of patients with a solid or Bosniak 3 or 4 complex cystic renal mass, clinicians must review the most common and serious urologic and non-urologic morbidities of each treatment pathway and the importance of patient age, comorbidities/frailty, and life expectancy (Clinical Principle). Dr. Uzzo emphasized that each treatment option is associated with a unique profile of renal functional and perioperative outcomes, as well as potential harms, and quality of life concerns. Each treatment strategy (radical nephrectomy, partial nephrectomy or thermal ablation) has similar rates of minor and major complications, but a unique profile of complications to discuss. Importantly, each strategy should account for patient preferences and prioritize potential harms on an individual basis. Active surveillance foregoes the operative risks but introduces anxieties and oncologic risks not suitable for all patients.
Looking back at Case #1, Dr. Uzzo highlighted the following imaging dates, size of the renal mass, and key events:
- CT June 2001: 1.5 cm enhancing solid lesion
- November 2001: CVA with aspiration, recovered
- CT January 2002: 1.5 cm enhancing solid lesion, unchanged
- CT June 2002: 1.5 cm enhancing solid lesion, unchanged
- CT December 2002: 1.5 cm enhancing solid lesion, unchanged
- CT July 2003: 1.5 cm enhancing solid lesion, unchanged
- CT February 2004: 1.5 cm enhancing solid lesion, unchanged
- CT May 2005: 1.5 cm enhancing solid lesion, unchanged
- The patient ultimately passed way in 2007 secondary to other causes
For Case #2, Dr. Uzzo highlighted the following imaging dates and size of the renal mass:
- CT July 2001: 2.0 cm enhancing lesion with simple cysts
- CT September 2001: 2.0 cm enhancing lesion, unchanged
- Ultrasound December 2001: 2.2 cm solid renal mass
- Ultrasound April 2002: 1.8 cm solid renal mass
- CT July 2002: 2.5 cm renal mass
- CT December 2002: 2.6 cm renal mass
Given this patient’s increasing anxiety, he underwent cardiac clearance for surgery and underwent an uncomplicated 2 hour laparoscopic partial nephrectomy with minimal blood loss for a grade 2 clear cell RCC. However, during the closure, the patient suffered a cardiac arrest, was immediately transferred to the cardiac cath lab, but ultimately passed away.
Next, Dr. Uzzo discussed Case #3 (higher risk/“complex” active surveillance), an 82 year old female with flank pain and history of kidney stones who was diagnosed with a 4.5 cm renal mass. Her medical history was significant for hypertension secondary to renal artery stenosis (on prednisone 20 mg/day), COPD (on home oxygen), emphysema, and diverticulitis (s/p colectomy). Her ECOG performance status was 2-3 and her eGFR was 64 cc/min:
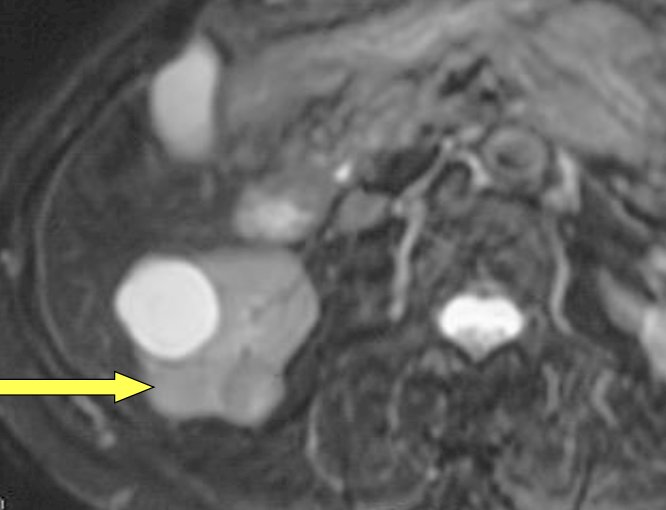
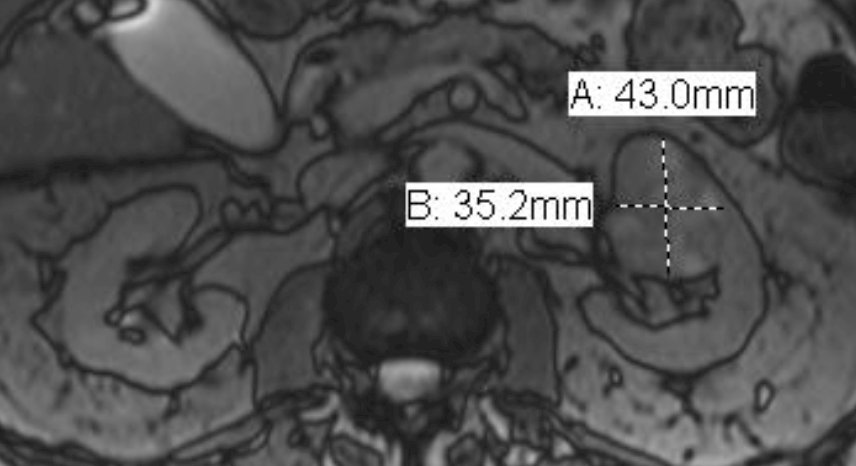
Case #4 (higher risk/“complex” active surveillance) was an 85 year old male with a history of hypertension, coronary artery disease, Gleason 6 prostate cancer (treated with IMRT), and chronic kidney disease stage 3 (eGFR 32 cc/min) who was noted to have a 4.3 x 3.5 cm incidental renal mass found on an evaluation of weight loss. His ECOG performance status was 0, with the following MRI images:
Statement #30 of the AUA guidelines states, “For patients with a solid or Bosniak 3 or 4 complex cystic renal mass, clinicians should prioritize active surveillance/expected management when the anticipated risk of intervention or competing risks of death outweigh the potential oncological benefits of active treatment. In asymptomatic patients, the panel recommends periodic clinical surveillance and/or imaging based shared decision making (Clinical Principle).” Dr. Uzzo notes that when competing risks outweigh oncologic risk, active surveillance should be mandatory. Clinicians should orient and reorient patients regarding active surveillance and consider print and online resources to educate patients. Clinicians should also include patients, family, and caregivers in these discussions, and encourage good record keeping, noting improvements or diminishments in symptoms or health conditions once observation begins. When competing risks are equivalent to oncologic risk, this can be managed with “relative” active surveillance. Patients should be informed that the risk of metastases is low (<3%) in the short term (median of 24-36 months), but not zero. Triggers of progression may include absolute tumor size, complexity, infiltrative appearance, and interval growth. Moreover, since histology may improve stratification for success or failure of active surveillance, clinicians may consider renal mass biopsy in patients with an equivocal clinical risk/benefit analysis, which may decrease anxiety and recalibrate risk calculation. The following table from the AUA guidelines [2] provides guidance on factors favoring active surveillance versus expectant management:

Looking back at Case #3, the patient eventually underwent a renal mass biopsy of her 4.5 cm renal mass, which demonstrated clear cell RCC grade 2, and 6 month of subsequent imaging showed growth to 4.7 cm. Moving forward, this mass was stable for 18 months, but eventually demonstrated growth to 5.0 cm (with a renal venous thrombus). Ultimately, the patient passed away at home of pulmonary complications at the age of 85 years, 3+ years after presenting with her renal mass.
For Case #4, this patient also had a renal mass biopsy that showed clear cell RCC grade 2-3. He also chose active surveillance, and ultimately passed at 96 years of age (after celebrating his 70th wedding anniversary) from heart disease, with an 8.8 cm renal mass, eGFR of 24, and cT3aN0M0 RCC during almost four years before passing away.
With regard to whether we should excise, ablate, or observe small renal masses, the AHRQ database is unable to identify strong, consistent predictors of comparative oncologic benefit among management strategies. This data is limited by heterogeneity and a paucity of data, particularly for assessing treatment other than radical or partial nephrectomy. Importantly, increasing age or limited life expectancy is associated with a lower incidence of cancer specific mortality independent of management strategy, especially in patients > 75 years of age. However, it is impossible to determine if one management strategy is preferred based on patient age, comorbidities, frailty, and/or life expectancy, and all treatment modalities should be considered during individualized counseling. The “Score Card” for localized RCC provided by Dr. Uzzo highlights active surveillance as follows:

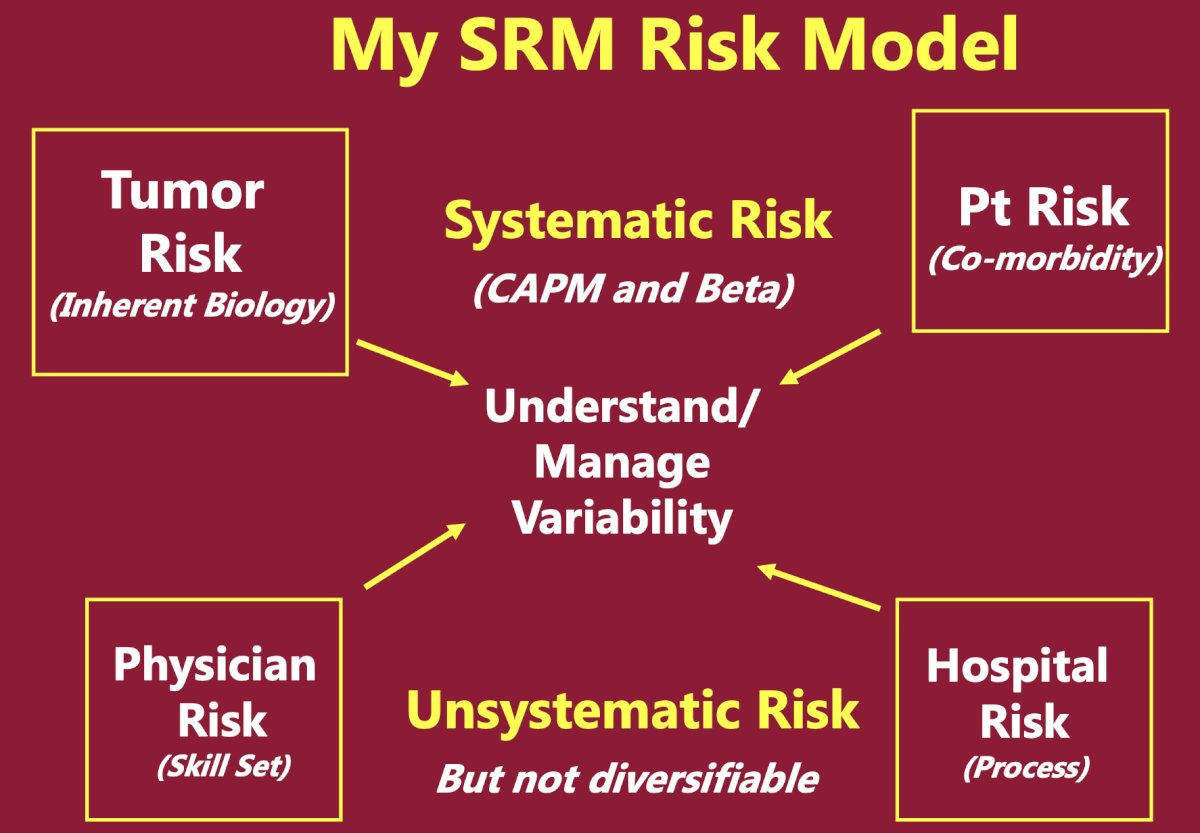
Dr. Uzzo’s small renal mass risk model is emphasized in the following algorithm:
Finally, Dr. Uzzo concluded his presentation discussing when to start and when to stop active surveillance for localized kidney cancer by highlighting a quote from Sir William Osler “Medicine is a science of uncertainty – and an art of probability.”
Presented by: Robert Uzzo, MD, MBA, FACS, Fox Chase Cancer Center, Philadelphia, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.
References:
- Campbell SC, Clark PE, Chang SS, et al. Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-Up: AUA Guideline: Part I. J Urol. 2021 Aug;206(2):199-208.
- Campbell SC, Uzzo RG, Karam JA, et al. Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-Up: AUA Guideline: Part II. J Urol. 2021 Aug;206(2):209-218.