(UroToday.com) The 2025 South Central AUA annual meeting included a session on bladder cancer, featuring a trials in progress presentation from Dr. Yair Lotan discussing a streamlined, patient-centric design of the cretostimogene grenadenorepvec expanded access program in patients with non-muscle invasive bladder cancer unresponsive to BCG.
The current AUA guideline recommendation for patients diagnosed with high-risk BCG-unresponsive non-muscle invasive bladder cancer is radical cystectomy. However, many patients are unwilling to undergo this morbid intervention or are unfit due to competing medical risks. Therefore, a considerable unmet medical need exists for clinically effective, well-tolerated, and readily available bladder-sparing treatment options for patients with high-risk BCG-unresponsive non-muscle invasive bladder cancer.
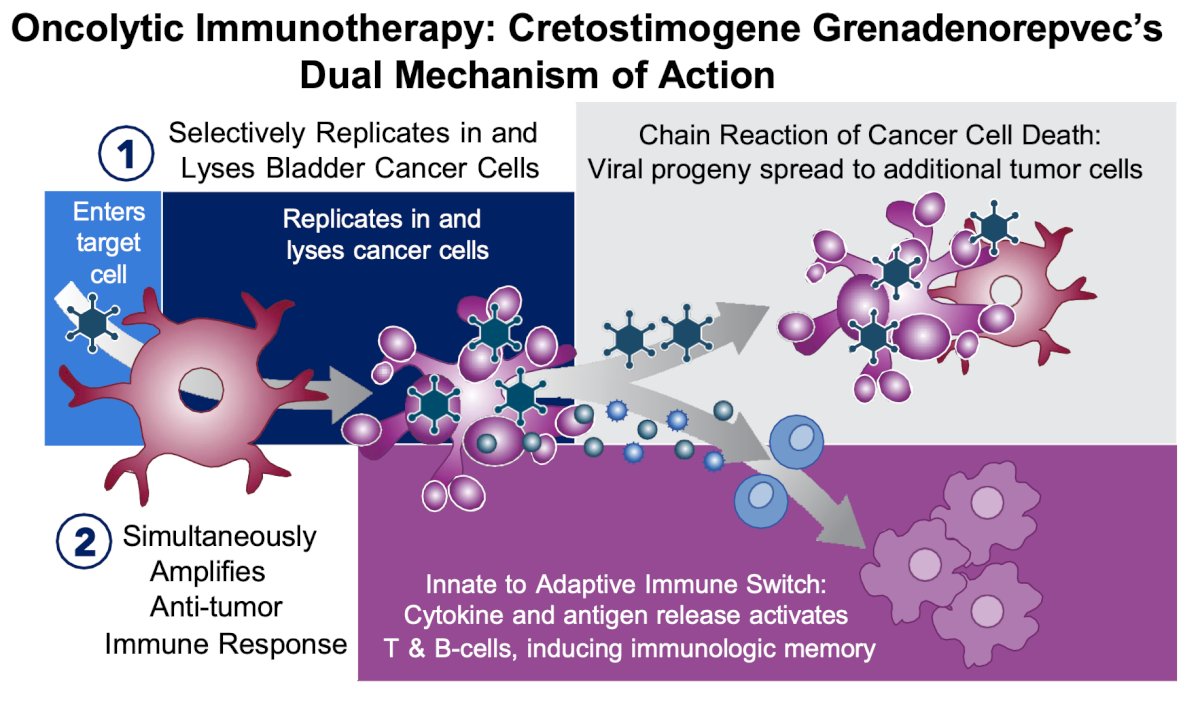
Cretostimogene grenadenorepvec is an oncolytic immunotherapy with a dual mechanism of action. It selectively replicates in and lyses bladder cancer cells with Rb-E2F pathway alterations. The subsequent release of virus- and tumor-specific antigens initiates an antitumor immune activation amplified by the transgene for GM-CSF, a potent cytokine:
Based upon preliminary efficacy and safety results from the ongoing Phase 3 BOND-003 study, cretostimogene received Fast Track and Breakthrough Therapy Designations by the US FDA for the BCG-unresponsive non-muscle invasive bladder cancer with CIS indication. The cretostimogene Expanded Access Program (CRETO-EAP) (NCT06443944) is an open-label, expanded access clinical trial designed to provide cretostimogene to a diverse population of real-world patients with BCG-unresponsive non-muscle invasive bladder cancer with CIS who may not otherwise be eligible for currently enrolling clinical trials.
Pragmatic real-world eligibility criteria are as follows:
- ECOG performance status 0-3
- Pathologically confirmed BCG-unresponsive CIS +/- HG Ta/T1 disease after completion of adequate BCG treatment
The protocol has been amended to improve flexibility and allow patients who received prior therapies for high-risk BCG-unresponsive non-muscle invasive bladder cancer, including investigational agents:
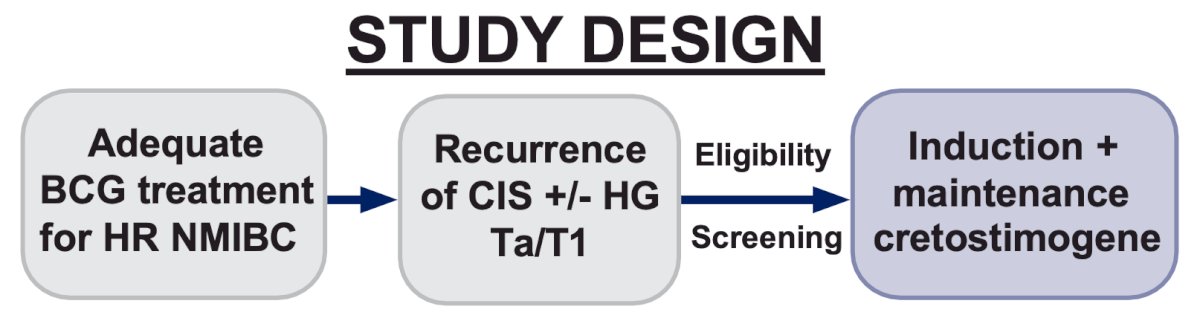
Intravesical cretostimogene will be administered in combination with n-dodecyl-β-D-maltoside (DDM), an excipient that enhances adenoviral delivery for six weekly doses during the induction phase, followed by three weekly maintenance cycles quarterly through month 12, then every six months through month 24. Re-induction is permitted. Additionally, patients with partial response, defined as persistent but improved disease at week 25 or subsequent time points, may receive continued doses of cretostimogene at the discretion of the investigator:

Primary disease assessments include serial cystoscopy, urine cytology, axial imaging, and directed bladder biopsies as clinically indicated, with local review of pathologic samples. Co-primary endpoints include safety and complete response at any time. The incidence of adverse events will be reported using Medical Dictionary for Regulatory Activities (MedDRA) and CTCAE v5.0. Secondary outcomes include duration of response, progression-free survival, cystectomy-free survival, patient-reported outcomes, and health-related quality of life measures. A broad cross-section of geographically diverse clinical sites in the US and Canada that serve socioeconomically diverse patients has been identified. The study is actively recruiting patients, with the first patients having received treatment.
Presented by: Yair Lotan, MD, Urologic Oncologist, UT Southwestern Medical Center, Dallas, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.