(UroToday.com) The 2026 American Society for Radiation Oncology (ASTRO) Multidisciplinary Radiopharmaceutical Therapy Symposium (MRPTS) held in Palm Desert, California between February 17th and 18th 2026, was host to the session Clinical Challenges in Radiopharmaceutical Therapy. Dr. Russell Szmulewitz discussed how to Navigate Hematologic and Renal Dysfunction in Radiopharmaceutical Therapy for Prostate Cancer.
Dr. Szmulewitz began by emphasizing that radium-223 dichloride and lutetium-177–PSMA-617 are now established treatment options for patients with metastatic prostate cancer. However, he highlighted important clinical considerations in this population, particularly limited bone marrow reserve and the risk of cumulative hematologic toxicity. He also noted that borderline renal insufficiency is common at baseline in these patients, which has implications for patient selection, safety monitoring, and dose optimization when using radiopharmaceutical therapies.
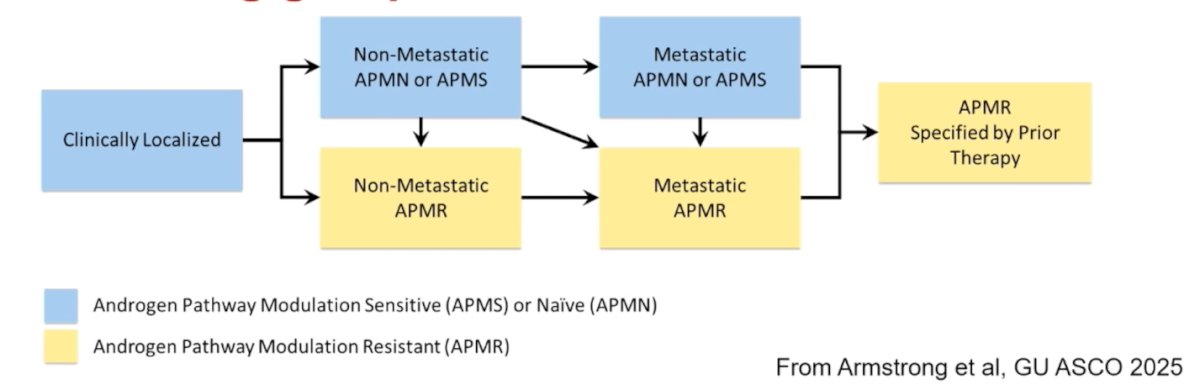
The Prostate Cancer Working Group 4 proposed an updated clinical state framework that reflects contemporary treatment paradigms. Rather than relying solely on hormone-sensitive versus castration-resistant terminology, the new nomenclature centers on androgen pathway modulation status, distinguishing androgen pathway modulation–naïve or –sensitive (APMN/APMS) from androgen pathway modulation–resistant (APMR) disease. These categories are further stratified by non-metastatic and metastatic states, with APMR additionally specified by prior therapies received. This revised structure better aligns disease classification with modern AR-targeted treatment strategies and sequencing in current practice.
Radium-223 dichloride is a bone-seeking alpha-emitting radiopharmaceutical that incorporates into osteoblastic metastases. The pivotal ALSYMPCA phase 3 trial randomized 992 patients with symptomatic mCRPC in a 2:1 fashion to radium-223 versus placebo, including patients who had received prior chemotherapy or were unfit for or declined chemotherapy. Radium-223 significantly improved overall survival and delayed symptomatic skeletal events, with a PSA response observed in 47% versus 3% in the placebo arm. These data established radium-223 as a standard option in symptomatic bone-predominant mCRPC.1
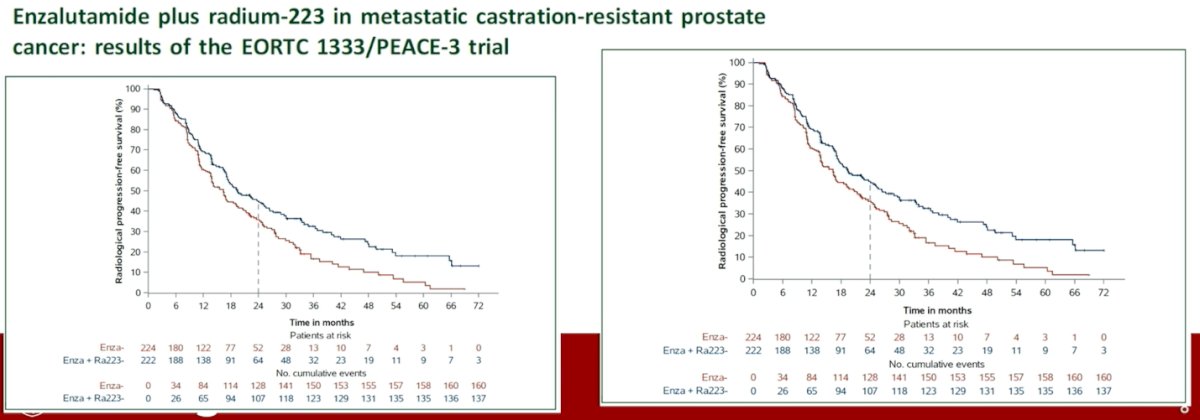
More recently, the PEACE-3 (EORTC 1333) trial evaluated enzalutamide with or without radium-223 in patients with first-line APMR mCRPC, the majority post-ADT and approximately 30% previously exposed to docetaxel. The addition of radium-223 to enzalutamide significantly improved overall survival (HR 0.69, p=0.003) and delayed time to next treatment, while time to pain progression and first symptomatic skeletal event were not significantly different. These data support a survival benefit with combination therapy in this earlier mCRPC setting and further define the role of radium-223 beyond the post-chemotherapy population.2
Dr. Smulewits highlighted that hematologic toxicity with radium-223 is higher than placebo, particularly in more heavily pretreated patients. In ALSYMPCA, rates of anemia, thrombocytopenia, and neutropenia were increased compared with placebo, with prior docetaxel exposure associated with greater hematologic adverse events. In PEACE-3, the addition of radium-223 to enzalutamide increased rates of anemia compared with enzalutamide alone, although grade ≥3 events remained relatively infrequent. Across studies, marrow failure occurred in approximately 2%, underscoring the need for careful patient selection and monitoring, particularly in those with limited bone marrow reserve.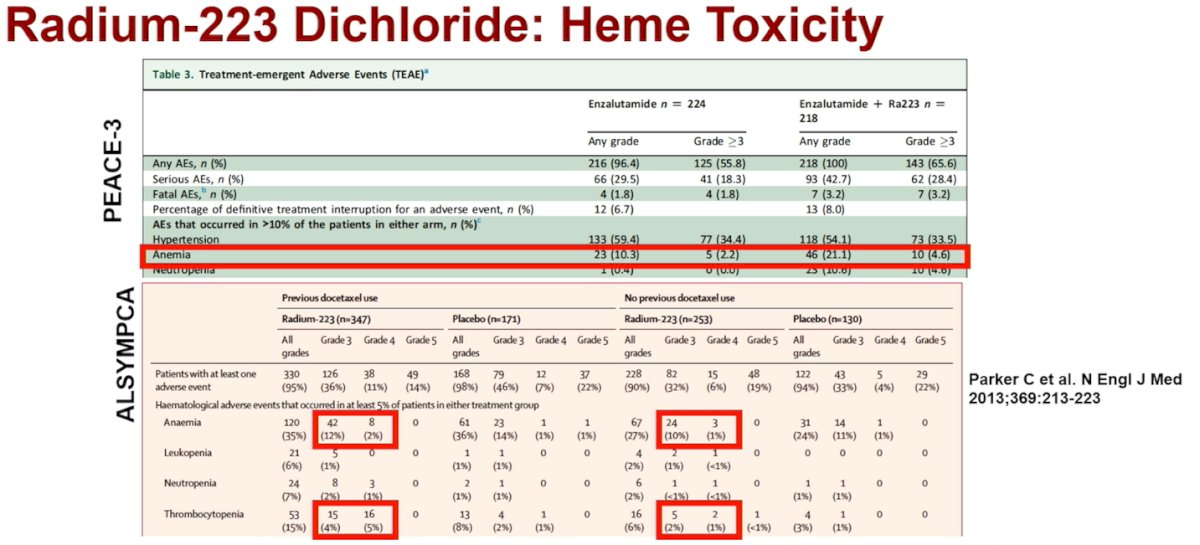
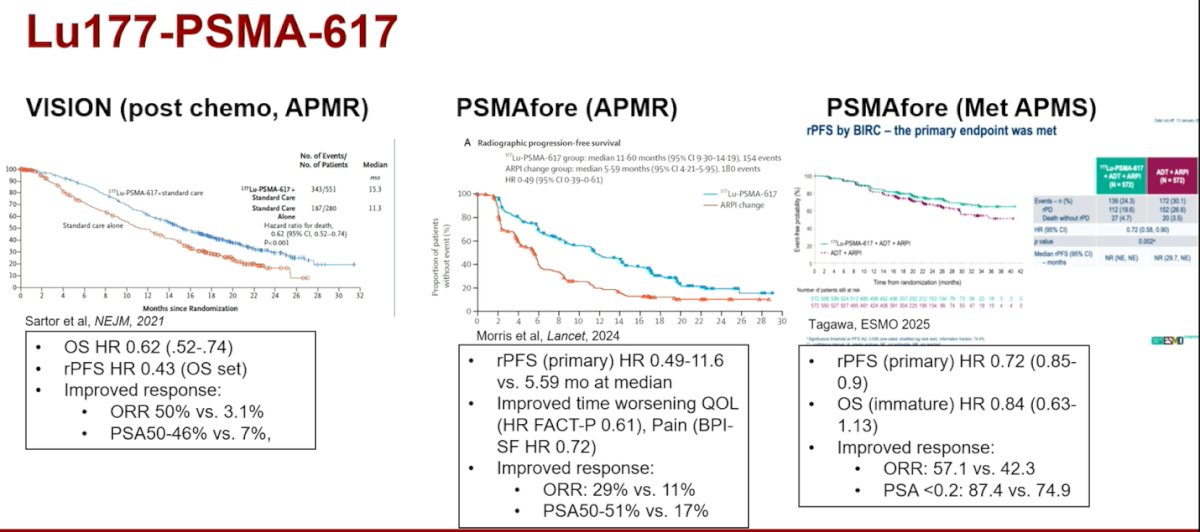
Dr. Szmulewitz then reviewed phase III data for ^177Lu-PSMA-617 across multiple clinical settings. In VISION (post-chemotherapy APMR), ^177Lu-PSMA significantly improved overall survival (HR 0.62) and radiographic PFS (HR 0.43), with marked response improvements (ORR 50% vs 3.1%; PSA50 46% vs 7%).3 In PSMAfore (pre-chemotherapy APMR), radiographic PFS improved substantially (HR ~0.49), along with time to worsening quality of life. Objective and PSA responses were again significantly higher.4 In PSMAddition (metastatic APMS), early-line use also demonstrated rPFS benefit (HR 0.72), with improved response rates, although OS data remain immature. Collectively, these data support expanding use of 177Lu-PSMA earlier in the disease course, raising important questions about long-term toxicity exposure.
He went on to discuss that adverse events across phase III trials leading to treatment interruption occurred in approximately 12–16% of patients. Dose reductions were required in 4–6%, and discontinuation rates ranged from 6–12%. Two deaths from pancytopenia were reported in VISION.3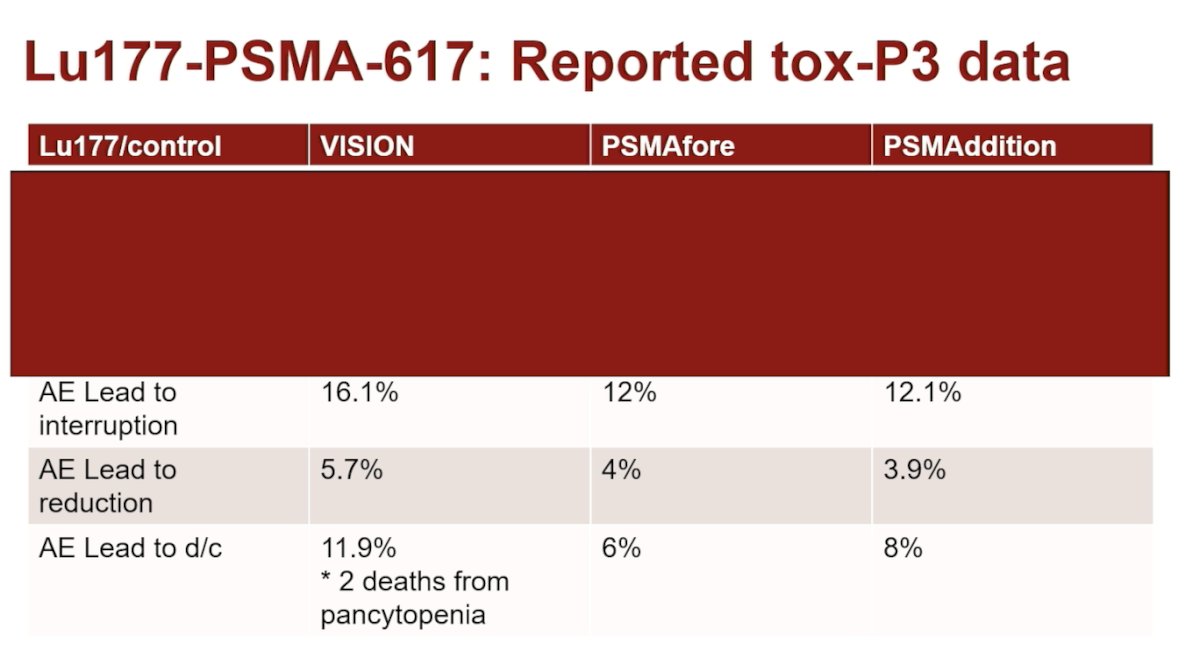
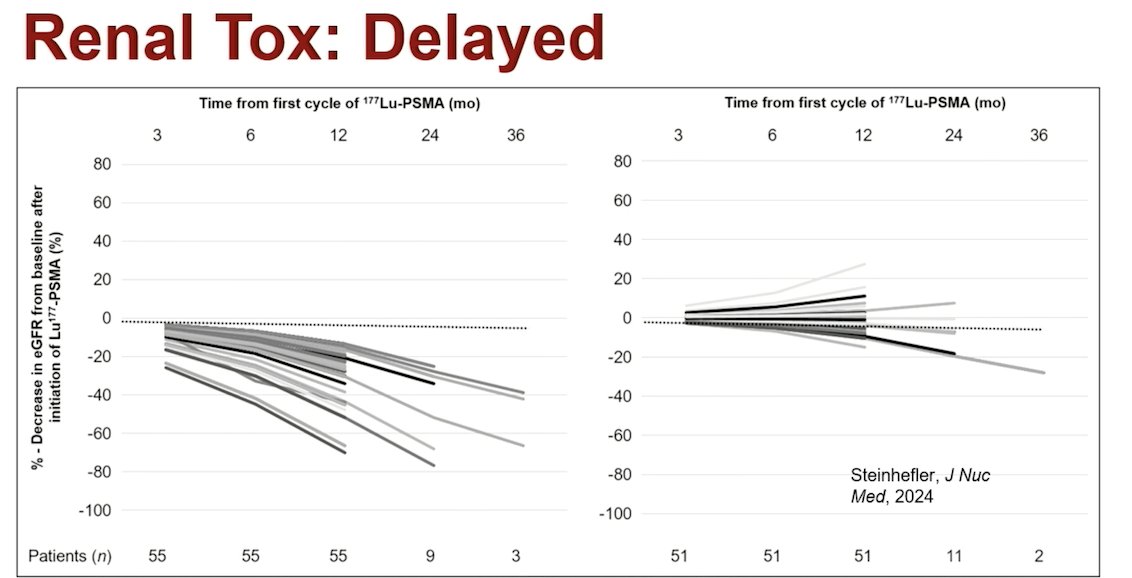
Renal toxicity appears to be more delayed. Retrospective data suggest that nearly half of patients experience ≥15% decline in GFR, with about 25% experiencing ≥40% decline. Only ~1% decline to GFR <30, but longer-term outcomes beyond one year remain insufficiently characterized. Given that PSMA is expressed in proximal tubules and that drug half-life increases in renal impairment, caution is warranted in patients with baseline chronic kidney disease.
Moreover, long-term marrow concerns are emerging. Retrospective data in 381 patients showed 1.3% treatment-related myeloid neoplasia, with a median time to diagnosis of 33 months. Additionally, post-hoc TheraP analyses suggest increased rates of clonal hematopoiesis after 177Lu-PSMA, particularly with greater exposure (OR 3.2 for new CH events). While causality remains unclear, these findings underscore the need for longer-term surveillance.
Dr. Szmulewitz highlighted retrospective sequencing data (radium to 177Lu-PSMA), suggesting higher rates of grade 3–4 anemia and thrombocytopenia, particularly within 90 days post-treatment, supporting the concept of cumulative marrow injury as shown below.
Regarding the management of renal toxicity, Dr. Szmulewitz highlighted that no dose reduction is required if GFR >30 mL/min. If creatinine rises ≥40% or CLcr decreases ≥40%, dose reduction should be considered. In his practice for CLcr 30–40 mL/min, he reduces to 160 mCi. For CLcr <30, data are limited; if no alternatives exist, he considers a 40–60% dose reduction with aggressive hydration.
Lastly, he moved on to discuss the management of hematological toxicity. For radium-223, label guidance requires ANC >1.5k and platelets >100,000 prior to treatment. Therapy should be held if platelets fall below 50,000. Dr. Szmulewitz checks CBC one week prior to each dose and discontinues therapy if counts fail to recover within 12 weeks. For 177Lu-PSMA, the label provides limited upfront dose modification guidance. Dr. Szmulewitz checks CBC and CMP mid-cycle and prior to dosing. Grade 3 anemia prompts transfusion and dose reduction. Growth factor support is used when clinically indicated. Dr. Szmulewitz noted that platelet-based decisions are stratified in his practice as follows:
- 75–100,000 platelets: treat with dose reduction (typically 160 mCi)
- 50–75,000: hold and reassess
- <50,000: do not treat
Dr. Szmulewitz concluded with the following key takeaways:
- Multidisciplinary coordination is essential in delivering RPT safely. Communication between oncology, nuclear medicine, and supportive care teams is critical.
- Hematologic toxicity is common, but incidence and severity appear lower when RPT is used earlier in the disease course. The long-term renal and marrow consequences of earlier and cumulative exposure remain uncertain.
- As new radiopharmaceuticals enter the prostate cancer landscape, key unanswered questions remain: how should we optimally sequence therapies? How do we mitigate long-term toxicity? And most importantly, can we dose more precisely and intelligently?
Presented by: Russell Szmulewitz, MD, Associate Director, Genitourinary Oncology Program; Assistant Professor of Medicine, University of Chicago Medical Center. Chicago, IL.
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society for Radiation Oncology (ASTRO) Multidisciplinary Radiopharmaceutical Therapy Symposium (MRPTS) held in Palm Desert, California, between February 17th and 18th, 2026.
References:
- Parker C, Nilsson S, Heinrich D, Helle SI, O'Sullivan JM, Fosså SD, Chodacki A, Wiechno P, Logue J, Seke M, Widmark A, Johannessen DC, Hoskin P, Bottomley D, James ND, Solberg A, Syndikus I, Kliment J, Wedel S, Boehmer S, Dall'Oglio M, Franzén L, Coleman R, Vogelzang NJ, O'Bryan-Tear CG, Staudacher K, Garcia-Vargas J, Shan M, Bruland ØS, Sartor O; ALSYMPCA Investigators. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med. 2013 Jul 18;369(3):213-23. doi: 10.1056/NEJMoa1213755. PMID: 23863050.
- Tombal B, Choudhury A, Saad F, Gallardo E, Soares A, Loriot Y, McDermott R, Rodriguez-Vida A, Isaacsson Velho P, Nolè F, Cruz F, Roumeguere T, Daugaard G, Yamamura R, Bompas E, Maroto P, Gomez Veiga F, Skoneczna I, Martins da Trindade K, Mavignier Carcano F, Lecouvet F, Coens C, Poncet C, Fournier B, Gillessen S. Enzalutamide plus radium-223 in metastatic castration-resistant prostate cancer: results of the EORTC 1333/PEACE-3 trial. Ann Oncol. 2025 Sep;36(9):1058-1067. doi: 10.1016/j.annonc.2025.05.011. Epub 2025 May 30. PMID: 40450503.
- Sartor O, de Bono J, Chi KN, Fizazi K, Herrmann K, Rahbar K, Tagawa ST, Nordquist LT, Vaishampayan N, El-Haddad G, Park CH, Beer TM, Armour A, Pérez-Contreras WJ, DeSilvio M, Kpamegan E, Gericke G, Messmann RA, Morris MJ, Krause BJ; VISION Investigators. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103. doi: 10.1056/NEJMoa2107322. Epub 2021 Jun 23. PMID: 34161051; PMCID: PMC8446332.
- Morris MJ, Castellano D, Herrmann K, de Bono JS, Shore ND, Chi KN, Crosby M, Piulats JM, Fléchon A, Wei XX, Mahammedi H, Roubaud G, Študentová H, Nagarajah J, Mellado B, Montesa-Pino Á, Kpamegan E, Ghebremariam S, Kreisl TN, Wilke C, Lehnhoff K, Sartor O, Fizazi K; PSMAfore Investigators. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naive patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): a phase 3, randomised, controlled trial. Lancet. 2024 Sep 28;404(10459):1227-1239. doi: 10.1016/S0140-6736(24)01653-2. Epub 2024 Sep 15. Erratum in: Lancet. 2025 Dec 21;404(10471):2542. doi: 10.1016/S0140-6736(24)02716-8. PMID: 39293462; PMCID: PMC12121614.