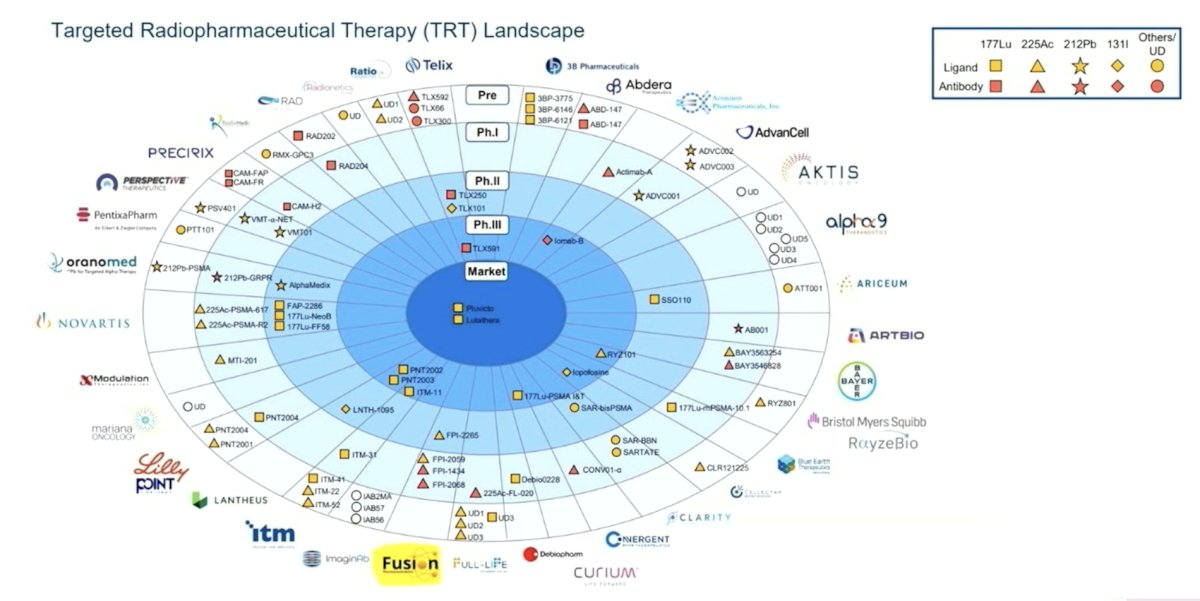
(UroToday.com) The 2026 ASTRO Multidisciplinary Radiopharmaceutical Therapy Symposium featured an access to therapy and addressing unmet needs session and a presentation by Dr. Ravi Patel discussing ways to address the unmet needs in radiopharmaceutical therapy. To start his presentation, Dr. Patel highlighted the vast targeted radiopharmaceutical therapy landscape:
Importantly, the challenge is patient access to radiopharmaceuticals, given that there is a need to expand access to radiopharmaceuticals outside of academic medical centers. Dr. Patel notes that there are different infrastructure needs for external beam radiotherapy versus radiopharmaceutical therapy, which is important to consider:

Ultimately, there is a need for increased collaboration between nuclear medicine and radiation oncology (including sharing revenue and resources), with the following advantages and disadvantages for radiation oncology and nuclear medicine:
- Radiation oncology advantages:
- Have a presence in community/rural settings to improve access
- Are able to administer therapeutic radiopharmaceuticals
- Have relationships with local medical oncologists and understand the oncology landscape
- May be better suited to understand the role of dosimetry
- Can combine external beam radiotherapy with radiopharmaceutical therapy
- Radiation oncology disadvantages:
- Most radiation oncology centers do not have nuclear imaging capabilities (PET/SPECT)
- They are not certified for diagnostic isotopes
- They have less experience in reading diagnostic imaging
- Radiation oncology centers may not have built-in infrastructure for theranostics (ie. nuclear medicine technician, hot lab, radioactive bathroom)
- Not all radiation oncologists have authorized user certification – 66% according to the 2024 ASTRO member survey
- The American Board of Radiology has made it harder for radiation oncologists to get broad scope authorized user certification
- Nuclear medicine advantages:
- Have imaging equipment and infrastructure for radiopharmaceuticals
- Are able to administer therapeutic and imaging radiopharmaceuticals
- Are better suited to read and understand the nuances of diagnostic imaging
- Many nuclear medicine physicians have more experience with radiopharmaceuticals
- Nuclear medicine disadvantages:
- Poor presence in community/rural settings (remote or academic positions)
- Many nuclear medicine teams do not manage toxicity or complete insurance authorizations
- Rely on referrals from oncology (radiation oncology and medical oncology)
- Less experience with dosimetry
Dr. Patel notes that there are several needs for expanding radiopharmaceutical therapy. The first need is full service staffing, which includes (i) financial counselors for authorizations, (ii) advanced practice providers to ensure proper follow–up, (iii) nursing for tracking labs, and giving patient instructions, (iv) patient coordinators for communicating with medical oncology, and coordinating care and transfusions, (v) medical physicists for program quality assessment, and incorporating imaging and dosimetry, (vi) nuclear medicine technologists for performing treatment administrations and imaging, and (vii) authorized users for either nuclear medicine or the radiation oncology physician. The second need is resources and billing, which includes (i) adequate staffing and equipment necessary for program building, (ii) reimbursement is skewed to the department administering the radiopharmaceutical therapy agent, however often patient management, authorization, and toxicity management is delegated to others, and (iii) community physicians want an easy solution for a referral, in that the more work that is placed on them, the less likely they will be to make a referral.
Additionally, there is a need for dosimetry for radiopharmaceutical therapy. With regards to dosing for external beam radiotherapy versus radiopharmaceutical therapy, external beam radiotherapy is generally prescribed as a dose to a point or volume, whereas radiopharmaceutical therapy is generally prescribed similarly to chemotherapy as an injected activity per injection, body weight, or surface area. There are several advantages for patient specific dosimetry for radiopharmaceutical therapy, which include:
- Uptake into areas of disease may be heterogeneous and vary by metastatic site or patient
- Normal tissue uptake and corresponding dose likely vary by patient
- Injected activity can be modified to increase the therapeutic index
- Combination external beam radiotherapy + radiopharmaceutical therapy treatment plans can be optimized for tumor control
Dr. Patel notes that there are several unknowns for dosimetry, such as it being unclear if dosimetry will provide a survival/treatment outcome benefit, and there are unknown dose constraints for normal tissues, whereas external beam radiotherapy dose constraints likely do not apply. The following emphasizes the general workflow for patient specific dosimetry for radiopharmaceutical therapy, which allows an optimized combination for radiopharmaceutical therapy + external beam radiotherapy treatment planning:

Patients undergoing radiopharmaceutical therapy can benefit from external beam radiotherapy, such as the use of palliation of painful sites, consolidation of heterogeneous responses, and providing local pain control. Examples include (i) 8 Gy x 1 for a bone metastasis, (ii) stereotactic body radiotherapy to a liver lesion, and (iii) treatment to the prostate as re-irradiation causing local symptoms. Currently, in their practice at UPMC, Dr. Patel notes that ~40% of patients receiving radiopharmaceutical therapy also get external beam radiotherapy, highlighting that the number of patients getting external beam radiotherapy with radiopharmaceutical therapy will likely increase with optimization of workflows.
Dr. Patel concluded his presentation discussing ways to address the unmet needs in radiopharmaceutical therapy with the following take-home points:
- Radiopharmaceutical therapy research, both clinical and preclinical, is a priority for academia as well as big pharma, and new agents are coming
- There is a need for increased collaboration between radiation oncology and nuclear medicine: each has strengths for leading a radiopharmaceutical therapy program, and models for program building and revenue sharing are needed
- Full service options with appropriate staffing and resources are needed for radiopharmaceutical therapy expansion to improve patient access
- Dosimetry and imaging may be incorporated into radiopharmaceutical therapy programs to personalize patient treatment, and trials testing dosimetry are needed
Presented by: Ravi Patel, MD, PhD, University of Pittsburgh Medical Center, Pittsburgh, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society for Radiation Oncology (ASTRO) Multidisciplinary Radiopharmaceutical Therapy Symposium, Palm Desert, CA, Tues, Feb 17 – Wed, Feb 18, 2026.