(UroToday.com) The 2026 ASTRO Multidisciplinary Radiopharmaceutical Therapy Symposium featured a plenary session and a presentation by Dr. Brandon R. Mancini discussing factors influencing lesion-level response after 177Lu-PSMA-radioligand therapy on post therapy SPECT/CT with artificial intelligence annotation. Post therapy SPECT/CT after treatment with Lu-177 PSMA-617 for metastatic prostate cancer enables a quantitative whole body assessment of tumor burden and uptake:
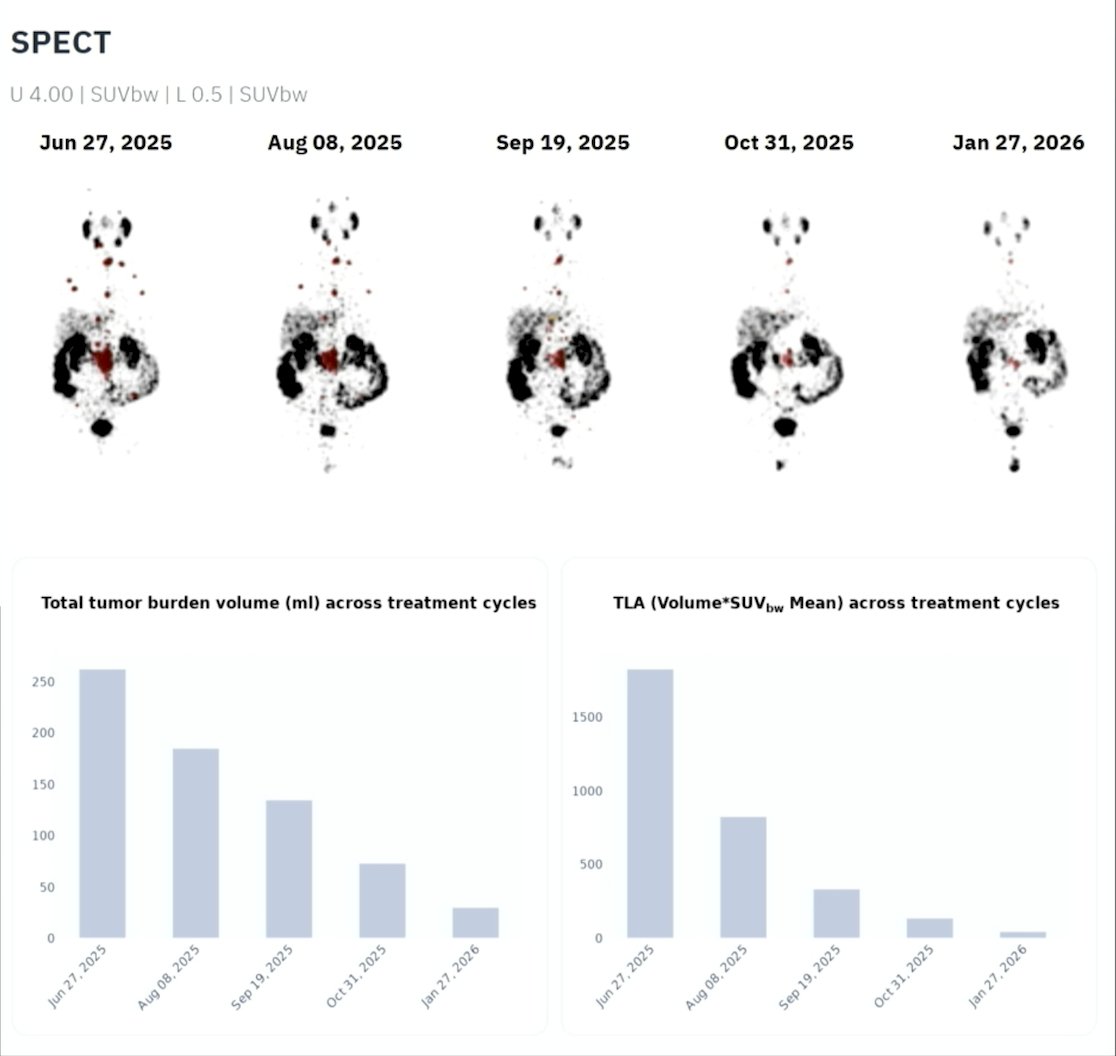
However, the relative prognostic value of lesion-level metrics for subsequent lesion response remains uncertain. The objective of this study is to determine which quantitative PSMA SPECT/CT metrics (ie. SUVmean/max/peak, lesion volume, total lesion activity, organ normalized ratios, and spatial dispersion) at a particular treatment cycle, ie. at time t, best predict the lesion-level outcome on a subsequent post therapy SPECT/CT study at a later cycle, ie, at time t+1 (~6 weeks later) using multinomial modeling.
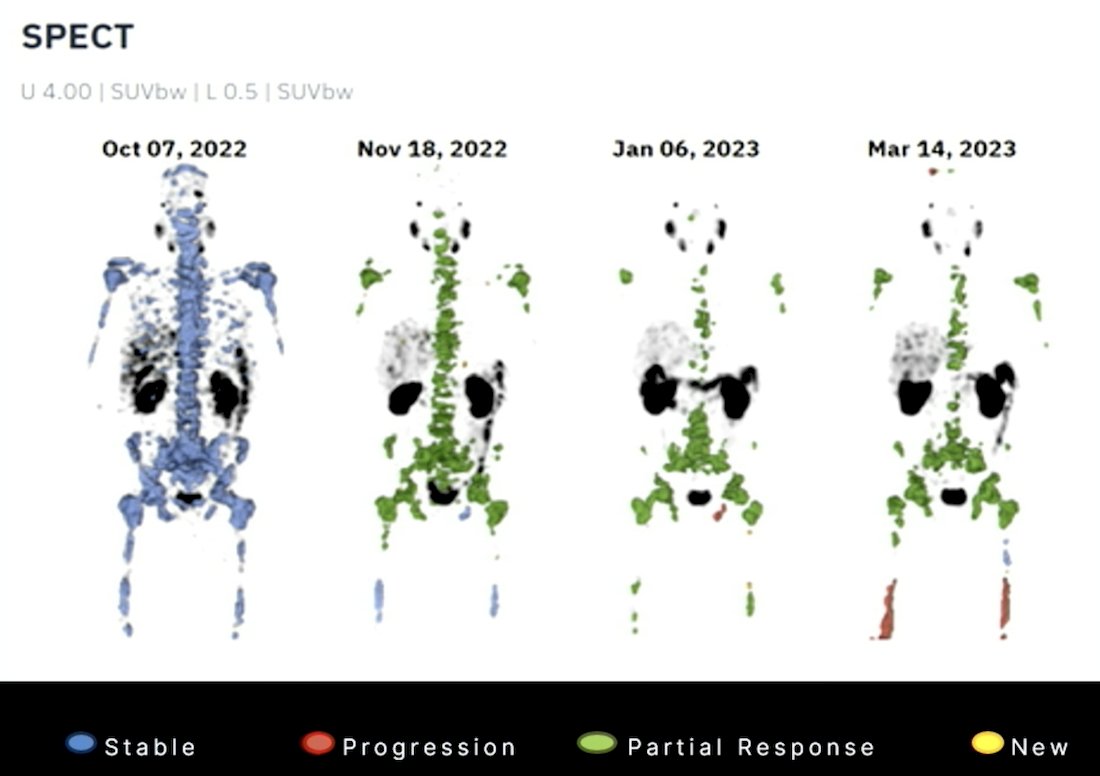
Dr. Mancini and colleagues retrospectively identified 43 patients with prostate cancer treated with at least 2 cycles of 177Lu-PSMA-617 who underwent quantitative post-therapy SPECT/CT at ~24 hours. A state-of-the-art deep learning model segmented the lesion, liver, salivary glands, and prostate. Lesions were defined as 3D connected components within the tumor mask (≥10 voxels). For each time t, lesion level metrics included volume, SUVmean, SUVmax, SUVpeak (~1 mL spherical volume of interest), ratios to liver/salivary (mean/max), ratios to total tumor (mean/max), and distance to the prostate centroid. Subject-level metrics included PSMA total tumor volume and total lesion activity (Σ SUVmean × volume). Lesion outcomes at t + 1 by volume were assigned by majority overlap with the subsequent study (1 = progression with volume increasing by >30%, 2 = stable, 3 = partial response with volume decreasing by >30%):
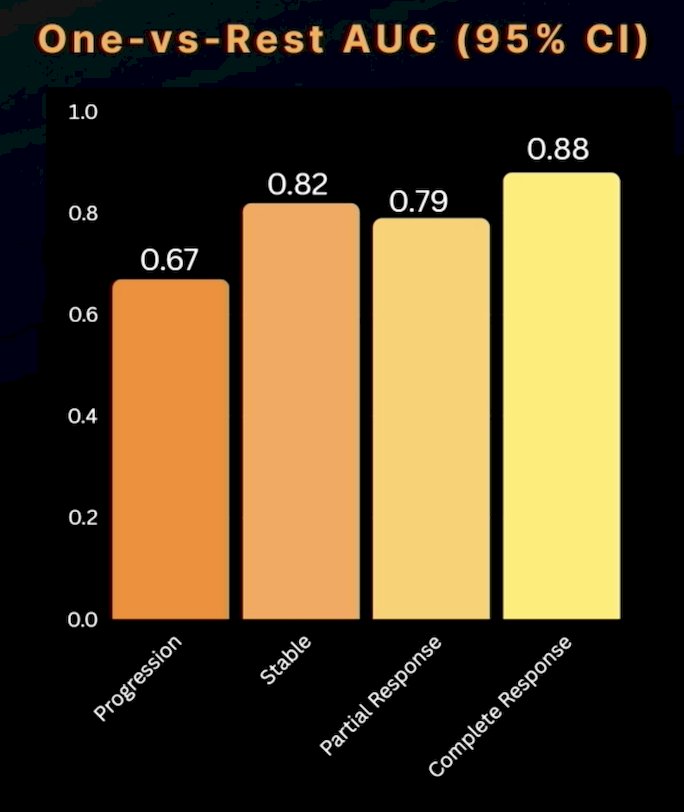
Primary modeling used penalized multinomial logistic regression (cross-validated L1/L2) for the 3-class outcome, with one versus rest receiver operating characteristic AUC (bootstrap 95% CIs) for class-wise discrimination.
Using all lesion and subject level predictors jointly, the penalized multinomial model achieved AUCs of 0.67 (95% CI 0.63–0.71) for progression (n = 174), 0.82 (95% CI 0.80–0.84) for stable (n = 420), 0.88 (95% CI 0.87–0.90) for complete response, and 0.79 (95% CI 0.78–0.81) for partial response (n = 1,101):
Bootstrap, FDR-controlled class-wise coefficients revealed outcome-specific signals: higher SUVpeak was associated with complete response, higher SUVmax was associated with stable and partially responding lesions, and higher SUVmean significantly increased the odds of a subsequent lesion progression. Conversely, higher baseline lesion volume strongly reduced the odds of a complete response.
Dr. Mancini noted that larger studies and validation will result in:
- Early identification of resistant lesions
- Enable lesion adaptive therapy
- Dose escalation
- Focal radiotherapy
- Treatment switching
- Moves beyond patient averages to precision theranostics
Dr. Mancini concluded his presentation discussing factors influencing lesion-level response after 177Lu-PSMA-radioligand therapy on post-therapy SPECT/CT with artificial intelligence annotation, with the following take-home points:
- Quantitative post-177Lu-PSMA-617 therapy SPECT/CT for a particular cycle (time t) provides an independent, clinically meaningful signal for predicting lesion level outcomes at a subsequent treatment cycle (t+1), with class-wise discrimination ranging from 0.67–0.88
- Core drivers are lesion uptake (SUVmax, SUVmean, SUVpeak), and volume metrics, supporting prospective validation and integration with clinical covariates for individualized therapy response assessment
- This framework is automated, scalable, and clinically actionable
Presented by: Brandon R. Mancini, MD, BAMF Health, Grand Rapids, MI
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society for Radiation Oncology (ASTRO) Multidisciplinary Radiopharmaceutical Therapy Symposium, Palm Desert, CA, Tues, Feb 17 – Wed, Feb 18, 2026.