The 2026 ASTRO Multidisciplinary Radiopharmaceutical Therapy Symposium featured a plenary session and a presentation by Dr. David Adam discussing quantitative radium-223 SPECT/CT for tumor dosimetry in combined stereotactic body radiotherapy and radiopharmaceutical therapy. Approximately 20% of prostate cancer diagnoses are classified as metastatic disease. Stereotactic ablative radiotherapy alone to treat oligometastatic disease has historically, based on the ORIOLE trial,1 resulted in microscopic failure. As such, combination approaches (ie standard of care stereotactic ablative radiotherapy and radium-223) could improve outcomes.
Outside of standard-of-care body-scaled administered activities, radium-223 has typically relied on model-based or 2D planar imaging approaches for dosimetry. Advances in quantitative SPECT/CT reconstruction now allow improved estimation of radium-223 activity distributions for organ and lesion dosimetry, and combining quantifiable SPECT/CT-alpha-based radiopharmaceutical therapy with stereotactic body radiotherapy may enable synergistic tumor dose escalation while mitigating the toxicities of stereotactic body radiotherapy alone. At the 2026 ASTRO Multidisciplinary Radiopharmaceutical Therapy Symposium, Dr. Adam presented data of retrospectively analyzed combined stereotactic body radiotherapy and radium-223 radiopharmaceutical therapy dosimetry in oligometastatic prostate cancer patients from a phase II clinical trial using SPECT/CT-derived dose estimates for multiple cycles.
The study consisted of 5 patients receiving standard of care stereotactic ablative radiotherapy and radium-223 (55 kBq/kg) between January 2021 and April 2023 under an IRB-approved phase II protocol. Quantitative SPECT/CT scans were acquired ~2–4, 24, and 48 hours after injection during the first and final treatment cycles using a novel reconstruction method incorporating forward projection modeling and multiple energy range corrections (6 lesions were analyzed):

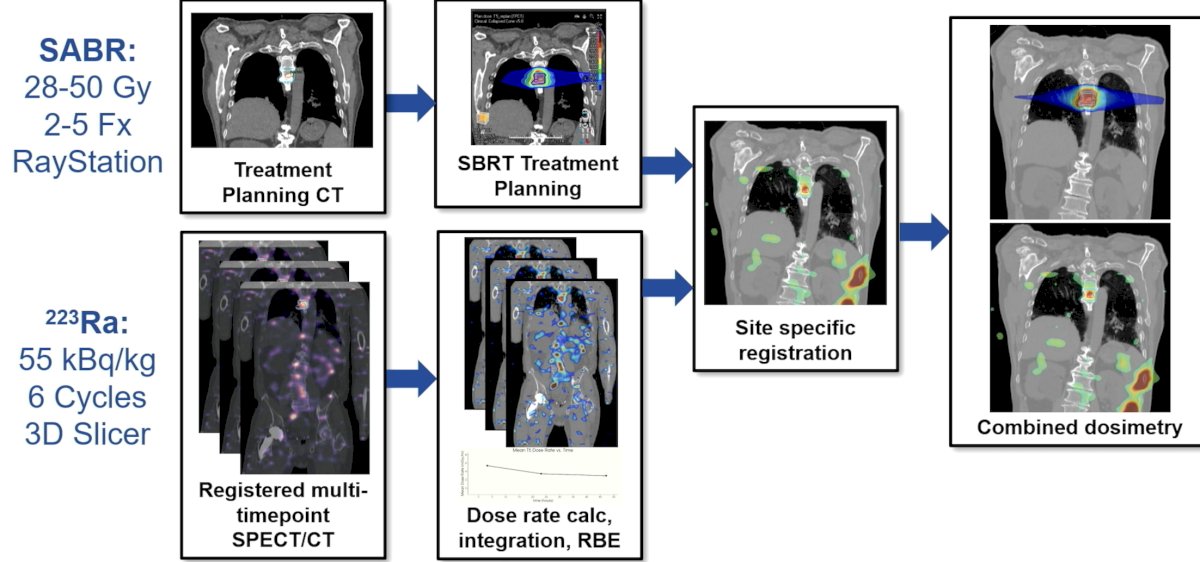
Standard of care photon stereotactic body radiotherapy plans were created in RayStation, and voxelwise radium-223 dose-rate maps were registered in 3D Slicer to the stereotactic body radiotherapy CT and integrated. The resultant absorbed dose was then imported and registered to the stereotactic body radiotherapy CT into the treatment planning system for voxelized summation. An alpha-particle relative biological effectiveness factor of 5 was applied to the radium-223 dose contribution. The dosimetry workflow for this study is as follows:
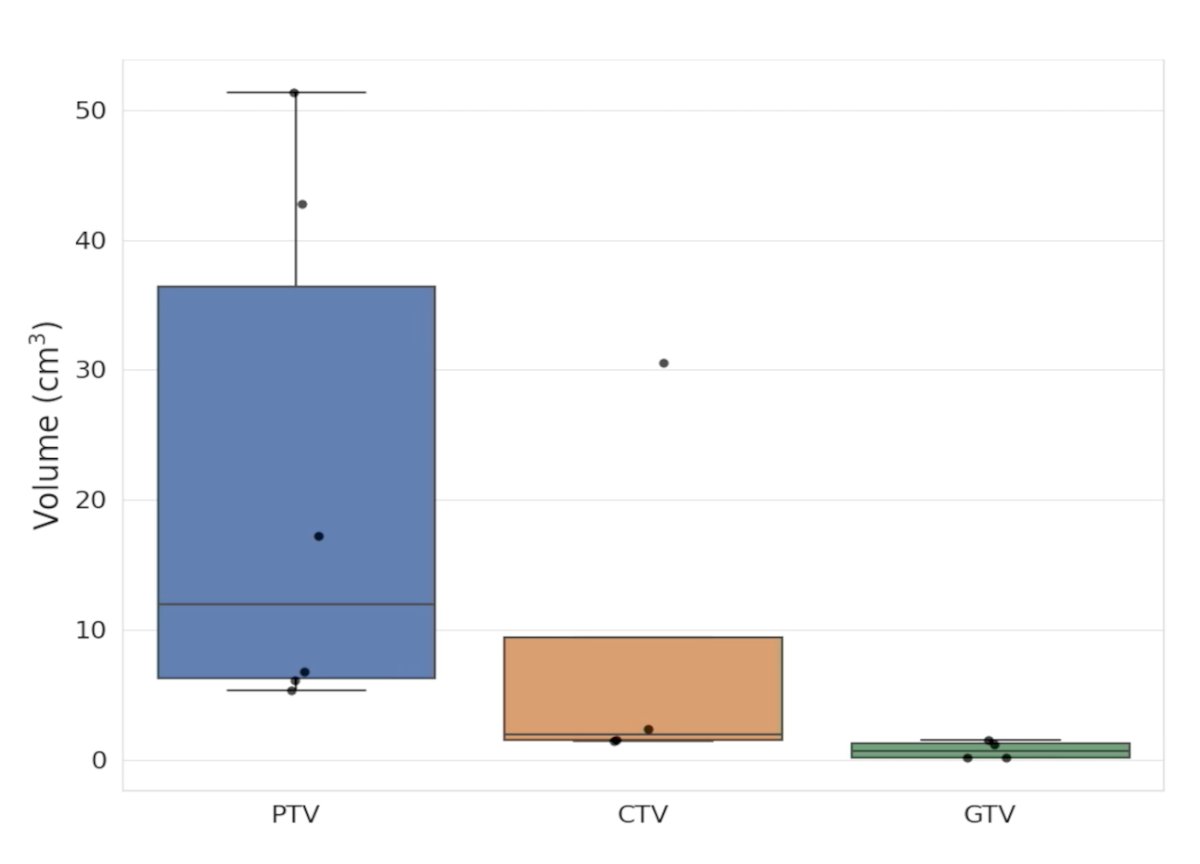
Among the 6 lesions analyzed, the 6 PTVs ranged from 5.4 – 51.3 mL (mean 21.6 mL), 4 CTVs ranged from 1.4-30.5 mL (mean 9.0 mL), and 4 GTVs ranged from 0.2-1.6 mL (mean 0.8 mL):
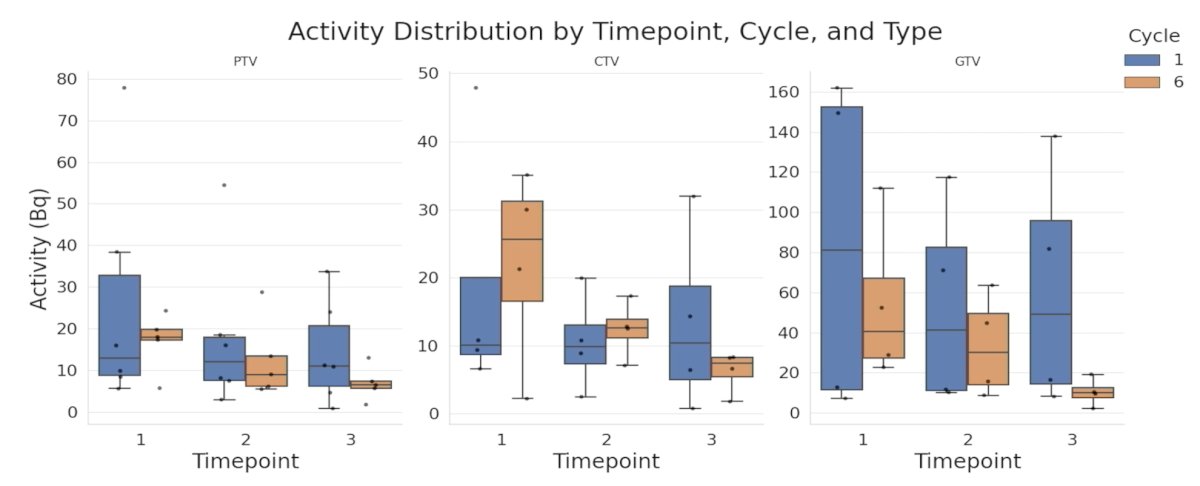
PTV and CTV had similar activity levels, while GTV was higher (up to ~160 Bq). Cycle 1 generally had greater activity than cycle 6:
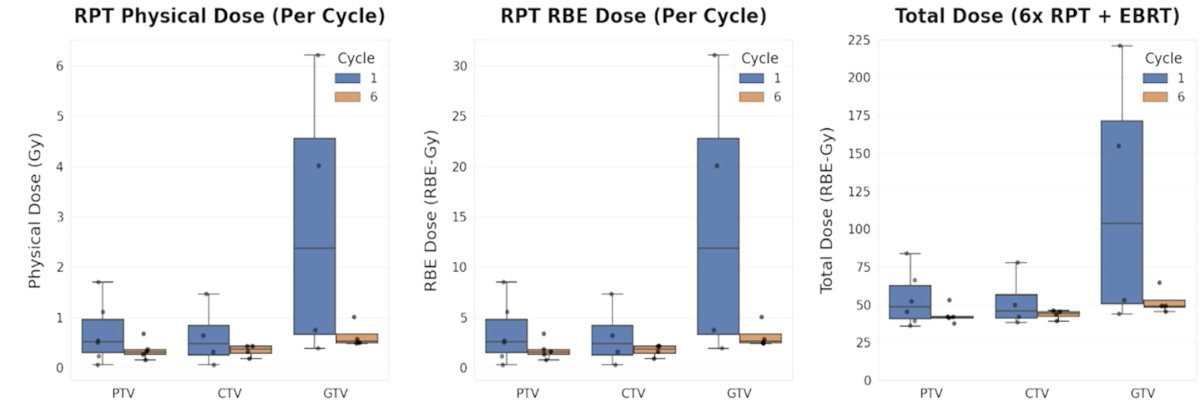
The PTV physical dose was 0.1-1.7 Gy, and the relative biological effectiveness dose was 0.3-8.5 Gy. Assuming 6 cycles, the combined dose for PTV was 36.0-83.8 relative biological effectiveness-Gy:
Dr. Adam provided the following discussion points:
- Caution with contour definition:
- GTV and CTVs considered were from external beam radiotherapy planning and quite small, especially in comparison to size of SPECT voxels
- The uncertainty of quantification for small targets is large
- Important if considering adaptive planning
- Caution with absorbed dose calculation:
- Local energy deposition, especially near heterogeneities
- Caution with voxel-level results
- Integration with dose-response:
- Assumed a relative biological effectiveness of 5, and subsequent radiobiologically informed dosimetry is important
- Accounting for micro-/small scale dosimetric phenomena
Dr. Adam concluded his presentation discussing quantitative radium-223 SPECT/CT for tumor dosimetry in combined stereotactic body radiotherapy and radiopharmaceutical therapy with the following take-home points:
- SPECT imaging of alpha-emitting compounds to inform combined stereotactic body radiotherapy and radiopharmaceutical therapy paradigms is possible
- Incorporating radiopharmaceutical therapy dose during the optimization of stereotactic body radiotherapy plans could potentially further improve treatment regimens for oligometastatic disease
Presented by: David Adam, PhD, MS, Johns Hopkins University School of Medicine, Baltimore, MD
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society for Radiation Oncology (ASTRO) Multidisciplinary Radiopharmaceutical Therapy Symposium, Palm Desert, CA, Tues, Feb 17 – Wed, Feb 18, 2026.
Reference:
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol 2020 Mar 26;6(5):650-659.