(UroToday.com) The 2026 ASTRO Multidisciplinary Radiopharmaceutical Therapy Symposium featured a radiopharmaceutical program start-up session and a presentation by Dr. Dustin Boothe discussing why now is the time to build a radiopharmaceutical therapy practice. Dr. Boothe started his presentation by emphasizing the mission to margin, specifically the reasons for your mission in developing and/or expanding a radiopharmaceutical program. This may include (i) expanding access to patients, (ii) research enablement, (iii) growing your skillset, and (iv) providing comprehensive care.
With regards to radiopharmaceutical therapy economics, Dr. Boothe notes that misunderstanding the economics can result in program rejection, stagnation, and dissolution. Common comments may be:
- “This program isn’t very profitable”
- “The hospital shut down because it was losing money”
- “We aren’t starting a program because we looked at it and it won’t make money”
- “My medical director doesn’t want us to do it because it doesn’t have good RVUs or reimbursement”
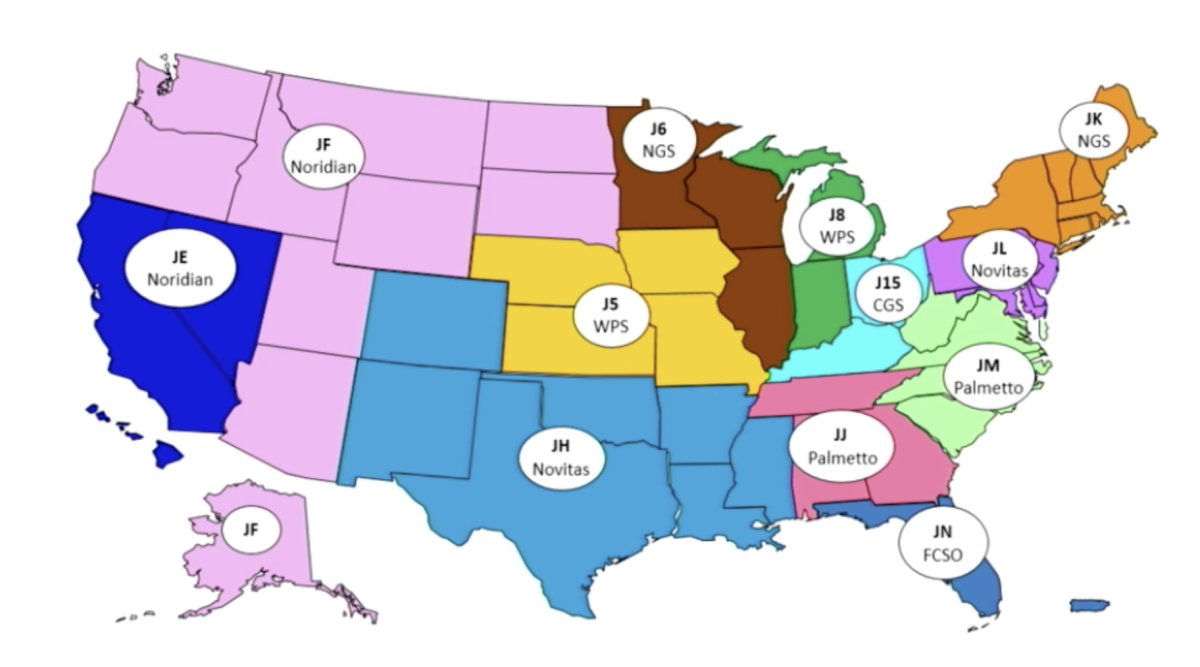
For freestanding radiopharmaceutical therapy economics, Dr. Boothe’s first take-home message is that Medicare reimburses radiopharmaceutical therapies using the average wholesale price, which is a good development given that the average wholesale price is better than the average sale price. The second take-home message is that the way you are paid by average wholesale price depends on where you practice. Medicare Administrative Contractors decide what percentage of the average wholesale price and when reimbursement increases relative to price increases:
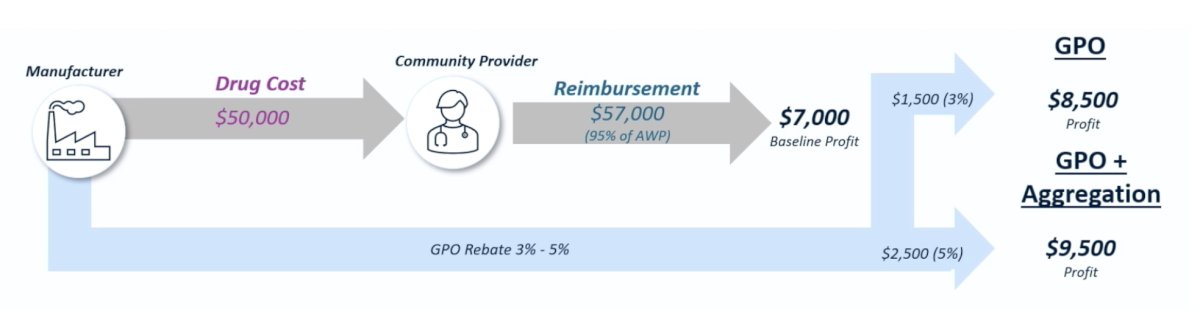
Take-home message #3 is to know the commercial contracts. Commercial payor contracts are highly variable and are often ignored in radiation centers. Dr. Boothe cautions that you may have a contract, but not a negotiated rate for drugs, thus it is important to know the contract before building a program. The fourth take-home message is that rebates help. It is important to know that rebates are processed through group purchasing organizations and that rebates are how free-standing oncology and urology practices have survived for decades:
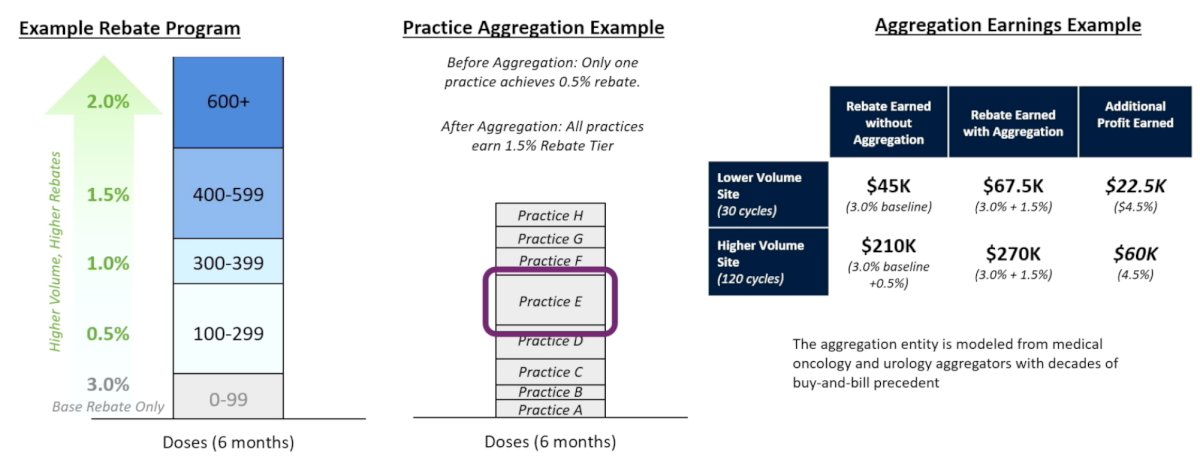
The fifth take-home message is that practice aggregation also helps. The following figure shows an example of a rebate program, an example of practice aggregation, and an example of aggregative earnings:
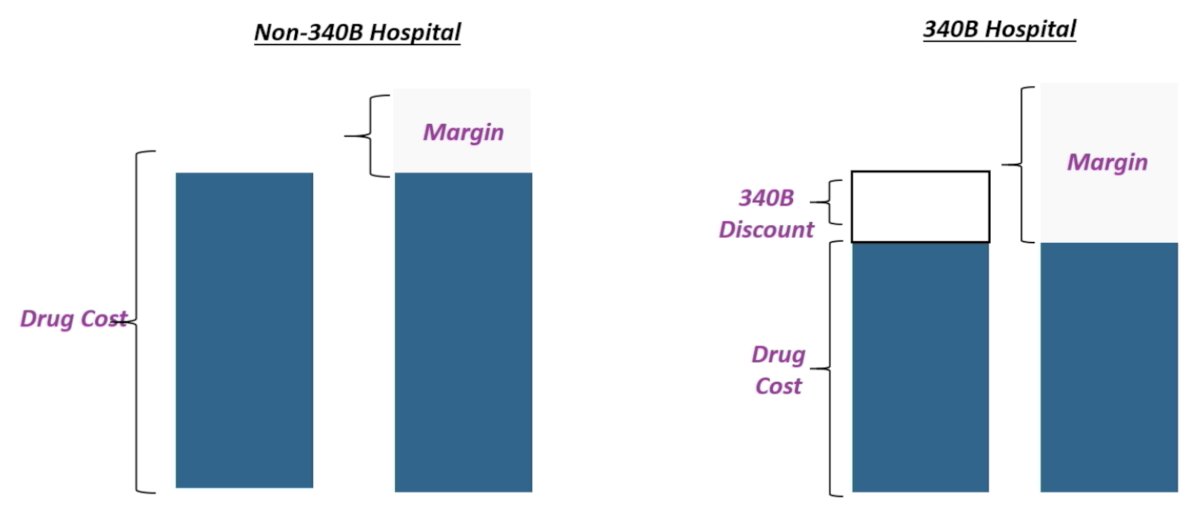
For hospital radiopharmaceutical therapy economics, the first take-home message is to know the hospital’s 340B status:
Take-home message #2 is to understand the silos, including radiation oncology, nuclear medicine/medical oncology, and the pharmacy department:
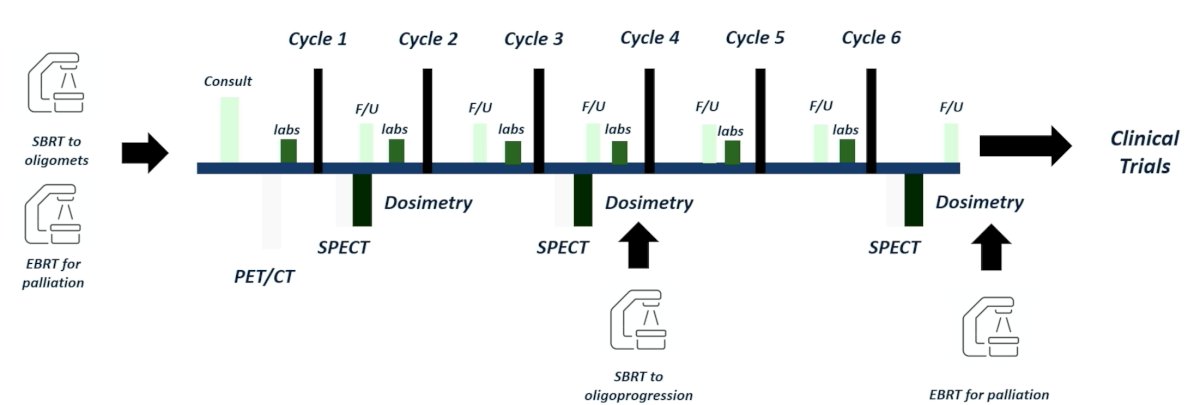
The third take-home message is to find ways to get paid without getting the drug revenue. This can include (i) medical directorships, (ii) RVU adjustments (done for medical oncology), and (iii) traditional RVUs. Finally, Dr. Boothe highlighted radiopharmaceutical therapy economics for everyone, specifically, that the program should be viewed as a “service line” and, when appropriate, we should add additional services:
Dr. Boothe concluded his presentation discussing why now is the time to build a radiopharmaceutical therapy practice with the following concluding points:
- Understanding radiopharmaceutical pricing and reimbursement is critical for evaluating the potential profitability of a radiopharmaceutical therapy program
- We need to look at a radiopharmaceutical therapy program as a “service line” and communicate value despite institutional “silos”
- We need to be both mission-focused and margin-conscious
Presented by: Dustin L. Boothe, MD, Intermountain Health Cancer Center, Murray, Utah
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society for Radiation Oncology (ASTRO) Multidisciplinary Radiopharmaceutical Therapy Symposium, Palm Desert, CA, Tues, Feb 17 – Wed, Feb 18, 2026.