(UroToday.com) The 2025 Interdisciplinary Genitourinary Cancer Forum featured a radical approaches to bladder cancer session and a presentation by Dr. Gennady Bratslavsky discussing the role of ctDNA in selecting adjuvant therapy post-cystectomy. Dr. Bratslavsky started his presentation by highlighting the historical report by Stein and colleagues1 who evaluated the USC long-term experience with patients treated uniformly with radical cystectomy and pelvic lymph node dissection for invasive bladder cancer. Among 1,054 patients over a median follow-up of 10.2 years (range: 0 to 28 years), the overall recurrence-free survival at 5 and 10 years was 68% and 66%, respectively. The 5- and 10-year recurrence-free survival for patients with organ-confined, lymph node-negative tumors was 92% and 86% for T0 disease, 91% and 89% for Tcis, 79% and 74% for Ta, and 83% and 78% for T1 tumors, respectively. Patients with muscle invasive (T2 and T3a), lymph node-negative tumors had 89% and 87% and 78% and 76% 5- and 10-year recurrence-free survival, respectively. Patients with nonorgan-confined (T3b, T4), lymph node-negative tumors demonstrated a significantly higher probability of recurrence compared with those with organ-confined bladder cancers (p <0.001). The 5- and 10-year recurrence-free survival for T3b tumors was 62% and 61%, and for T4 tumors was 50% and 45%, respectively. A total of 246 patients (24%) had lymph node tumor involvement. The 5- and 10-year recurrence-free survival for these patients was 35% and 34%, respectively, which was significantly lower than for patients without lymph node involvement (p <0.001):

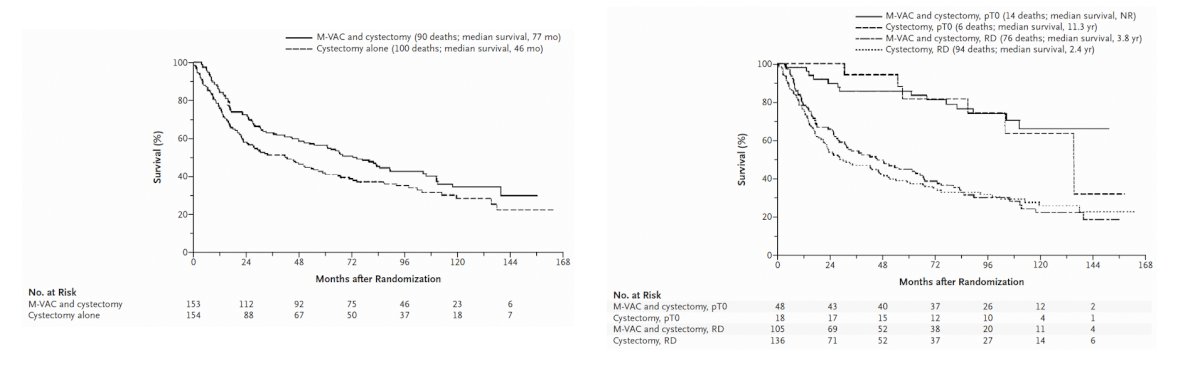
This analysis set the stage for the Grossman et al.2 SWOG 8710 landmark neoadjuvant chemotherapy trial, which showed a median survival among patients assigned to surgery alone of 46 months versus 77 months among patients assigned to neoadjuvant chemotherapy + radical cystectomy (p = 0.06). Moreover, the natural history of ypT > 0 residual disease had a 3.4 year overall survival benefit versus an 11 year survival benefit for ypT0:
Since these trials, we have seen the emergence of adjuvant nivolumab3 and pembrolizumab4 in muscle invasive bladder cancer, as well as perioperative durvalumab in combination with neoadjuvant chemotherapy5 in the perioperative setting:

However, with regards to adjuvant therapy following cystectomy, Dr. Bratslavsky emphasizes that we do not know what we are doing, and we do not know who to give adjuvant therapy to:

Perhaps biomarkers (ie. ctDNA, urine DNA, etc) are able to guide who is and who is not likely to benefit from adjuvant therapy for muscle invasive bladder cancer after radical cystectomy. In 2023, Christensen and colleagues6 investigated the use of plasma and urine DNA mutation analysis for predicting neoadjuvant chemotherapy response and oncological outcomes in 92 patients with muscle invasive bladder cancer. They found that tumor DNA levels were higher in urine supernatants and urine pellets compared with plasma samples (p < 0.001). In plasma, detection of ctDNA before neoadjuvant chemotherapy was associated with a lower neoadjuvant chemotherapy response rate (p < 0.001). Detection of tumor DNA after neoadjuvant chemotherapy was also associated with lower response rates in plasma, urine supernatant, and urine pellets (p < 0.001, p = 0.03, p = 0.002). Finally, tumor DNA dynamics during neoadjuvant chemotherapy was predictive of neoadjuvant chemotherapy response and outcome in urine supernatant and plasma (p = 0.006 and p = 0.002).
Recent work from Ben-David et al.7 assessed whether ctDNA status before radical cystectomy is predictive of pathological and oncological outcomes, in addition to evaluating the dynamic changes in ctDNA status after radical cystectomy in relation to recurrence-free survival. Among 112 patients undergoing radical cystectomy from 2021-2023, ctDNA was detected before radical cystectomy in 53% of patients and was associated with poor recurrence free survival (log-rank p < 0.0001):

Additionally, multivariable analyses demonstrated that detectable ctDNA before radical cystectomy was associated with a higher risk of nodal disease (OR 5.4, 95% CI 1.9-18.2; p = 0.003) and locally advanced disease (OR 3.6, 95% CI 1.5-9; p = 0.005).
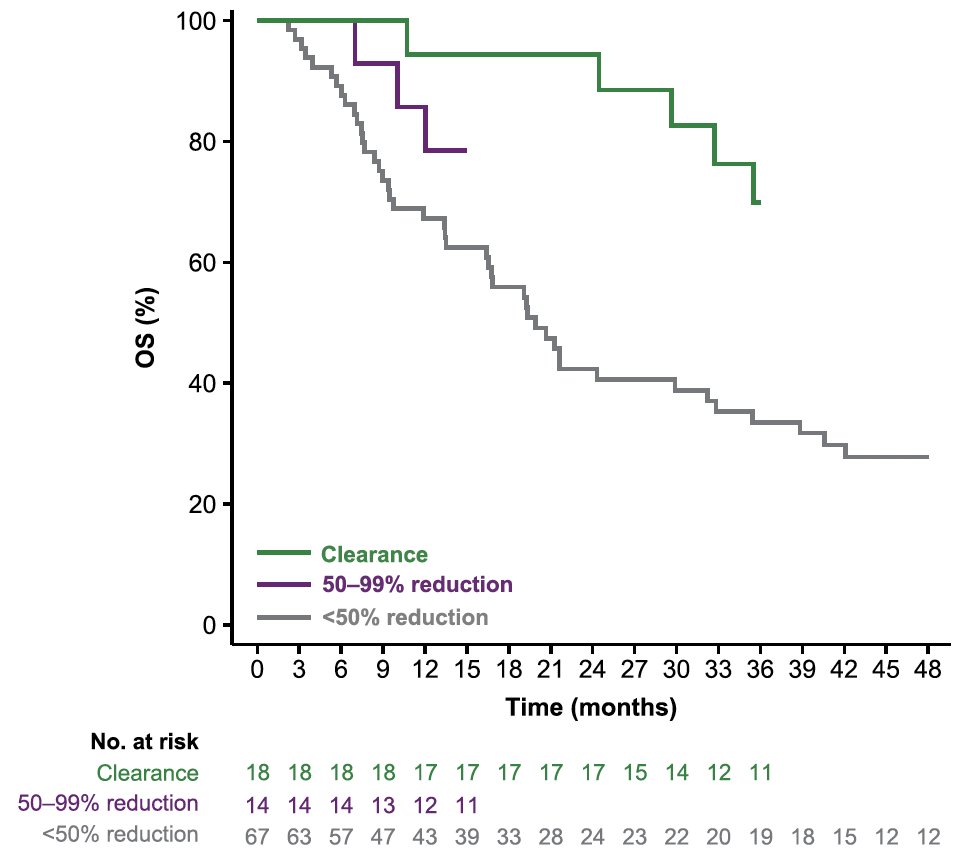
Dr. Bratslavsky then discussed ctDNA in the IMvigor010 trial, which at an interim analysis showed an overall survival benefit for adjuvant atezolizumab versus observation in patients with ctDNA positive muscle invasive urothelial carcinoma [8]. In an updated report published in 2024 [9], in the observation arm, ctDNA positivity versus negativity was associated with shorter overall survival (HR 6.3, 95% CI 4.3-9.3), and ctDNA positivity identified patients with an overall survival benefit favoring atezolizumab versus observation (HR 0.59, 95% CI 0.42-0.83). Moreover, a greater reduction in ctDNA levels with atezolizumab was associated with longer overall survival: 100% clearance, 60.0 months (95% CI 35.5-not estimable) versus 50-99% reduction, 34.3 months (95% CI 15.2-not estimable) versus <50% reduction, 19.9 months (95% CI 16.4-32.2):
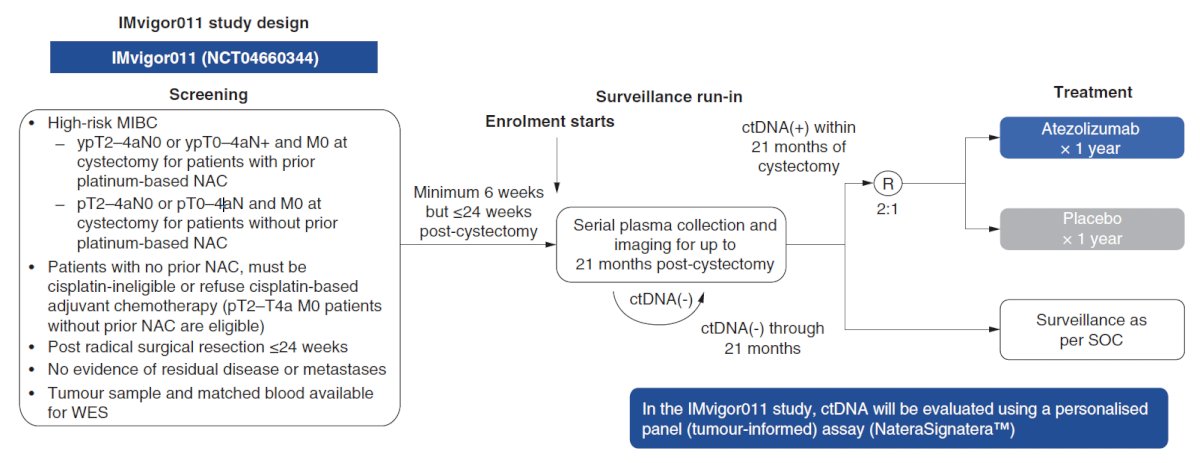
Finally, Dr. Bratslavsky highlighted two key ongoing trials in this disease space, the IMvigor011 trial and the MODERN trial:

Dr. Bratslavsky concluded his presentation discussing the role of ctDNA in selecting adjuvant therapy post-cystectomy with the following take home points:
- ctDNA is an evolving biomarker in management of bladder cancer
- Growing literature suggests that monitoring for ctDNA predicts outcomes and therapeutic response
- Data suggest that ctDNA may predict response to adjuvant therapy
- We are awaiting confirmation from prospective trials
Presented by: Gennady Bratslavsky, MD, SUNY Upstate, Syracuse, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Interdisciplinary Genitourinary Cancer Forum 2025, between June 19 – 22, 2025 in St. Petersburg, Florida, United States
References:
- Stein JP, Lieskovsky G, Cote R, et al. Radical cystectomy in treatment of invasive bladder cancer: long-term results in 1,054 patients. J Clin Oncol. 2001 Feb 1;19(3):666-675.
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med 2003;349(9):859-866.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021 Jun 3;384(22):2102-2114.
- Apolo AB, Ballman KV, Sonpavde G, et al. Adjuvant pembrolizumab versus observation in muscle-invasive urothelial carcinoma. N Engl J Med. 2025 Jan 2;392(1):45-55.
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(1):1773-1786.
- Christensen E, Nordentoft I, Birkenkamp-Demtroder K, et al. Cell-free urine and plasma DNA mutational analysis predicts neoadjuvant chemotherapy response and outcome in patients with muscle-invasive bladder cancer. Clin Cancer Res. 2023 Apr 14;29(8):1582-1591.
- Ben-David R, Tillu N, Cumarasamy S, et al. Longitudinal tumor-informed circulating tumor DNA status predicts disease upstaging and poor prognosis for patients undergoing radical cystectomy. Eur Urol Oncol. 2024 Oct;7(5):1105-1112.
- Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021 Jl;595(7867):432-437.
- Powles T, Assaf ZJ, Degaonkar V, et al. Updated overall survival by circulating tumor DNA status from the phase 3 IMvigor010 trial: adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma. Eur Urol. 2024;85(2):114-122.