(UroToday.com) The 2025 Interdisciplinary Genitourinary Cancer Forum featured a management of non muscle invasive bladder cancer session and a presentation by Dr. Leonard Gomella discussing novel agents in this disease space. Dr. Gomella started by noting that according to the 2014 NCCN guidelines in bladder cancer, BCG and mitomycin were the only intravesical options. Comparatively, 10 years later (2025 NCCN guidelines), we have several options:
- BCG
- Systemic pembrolizumab
- Adstilladrin
- Anktiva + BCG
- Chemotherapy: sequential gemcitabine + docetaxel, mitomycin, gemcitabine, epirubicin, valrubicin, docetaxel or sequential gemcitabine + mitomycin

Dr. Gomella notes that in 2025, there are several non muscle invasive bladder cancer outstanding needs:1
- Addressing the BCG supply shortages
- Identifying the most effective agents
- Optimal treatment sequencing
- Reducing treatment toxicity
- Biomarkers for patient selection: personalized approaches based on molecular profiling
- Developing novel delivery systems
Currently, there are general classes of novel agents in non muscle invasive bladder cancer:
- BCG:
- Plus immunotherapy (systemic and intravesical)
- Recombinant
- Novel sub-species (SWOG 1605, TOKYO, TICE)
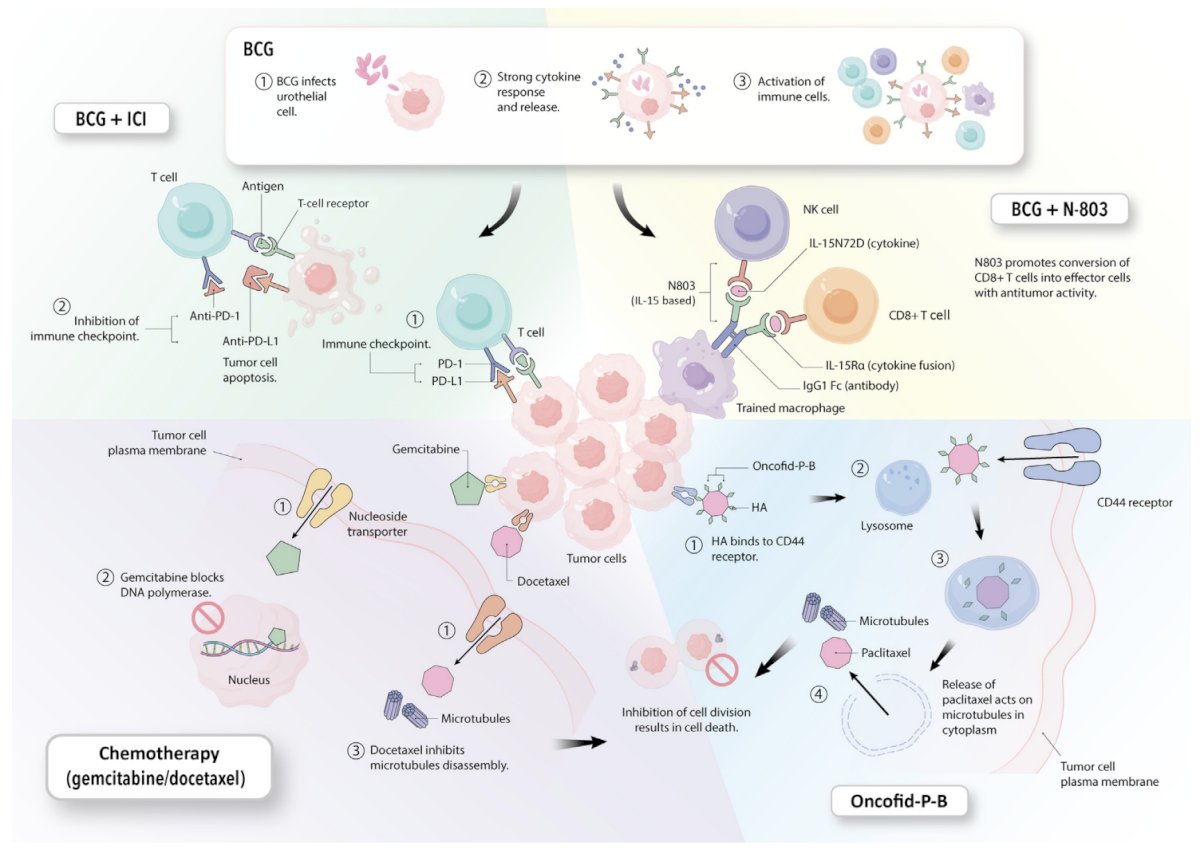
- Intravesical chemotherapy-based combinations:
- Gemcitabine + docetaxel versus BCG (BRIDGE Trial)
- Cabazitaxel, gemcitabine + cisplatin
- Chemical drug/antibody-drug conjugates:
- Oncofid-P-B
- Onco-Therad
- Large surface area microparticle docetaxel
- Enfortumab vedotin
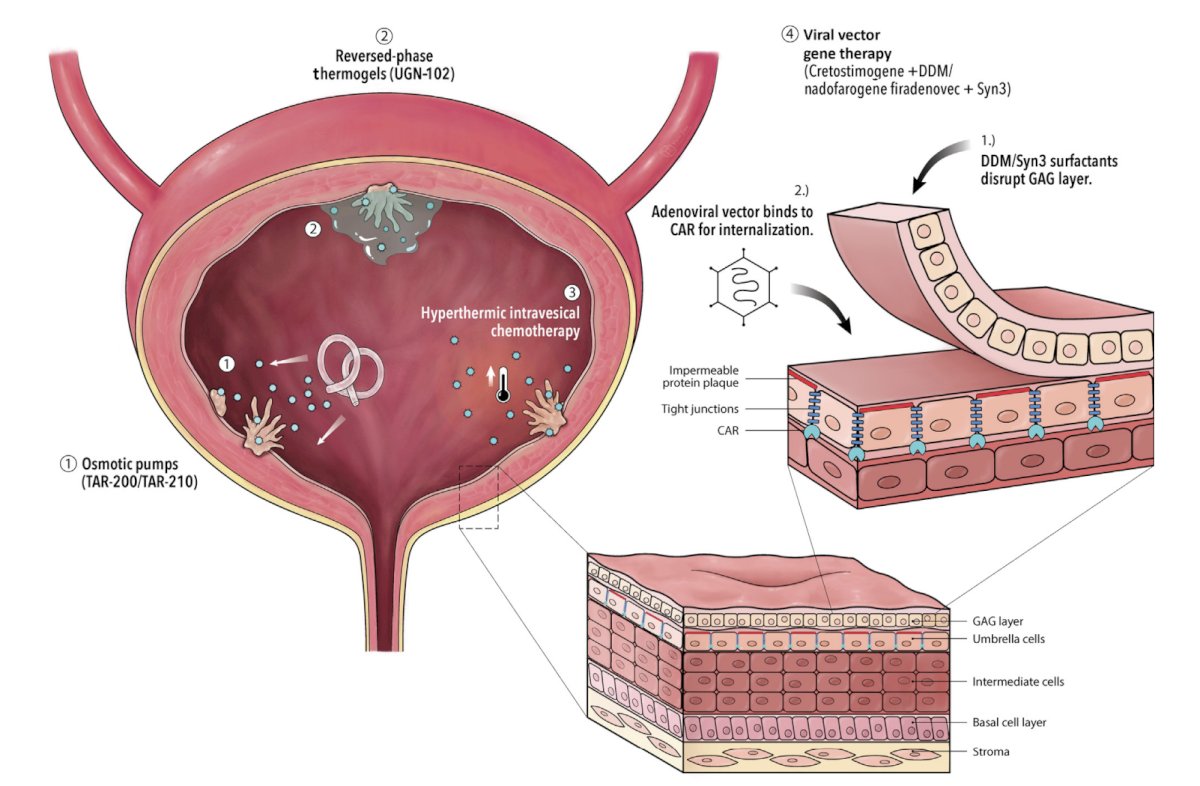
- Reverse phase thermo-gels:
- UGN-102 gel with mitomycin
- UGN-201 gel with imiquimod
- UGN-301 gel with zalifrelimab
- Ablative aqueous chemotherapies: mitomycin
- Hyperthermic intravesical chemotherapy:
- Gemcitabine via BR-PRG
- Mitomycin C via COMBAT bladder recruiting system
- Intravesical osmotic pumps:
- TAR-200 (gemcitabine)
- TAR-210 (erdafitinib)
- Viruses and vectors:
- Cretostimogene + DMM
- Nadofaragene firadenovec
- EG-70 (nanoparticle + IL-12 plasmid)
The following figure highlights intravesical therapies and mechanisms of action:1
Additionally, as follows is a representation of novel mechanisms of drug delivery:1
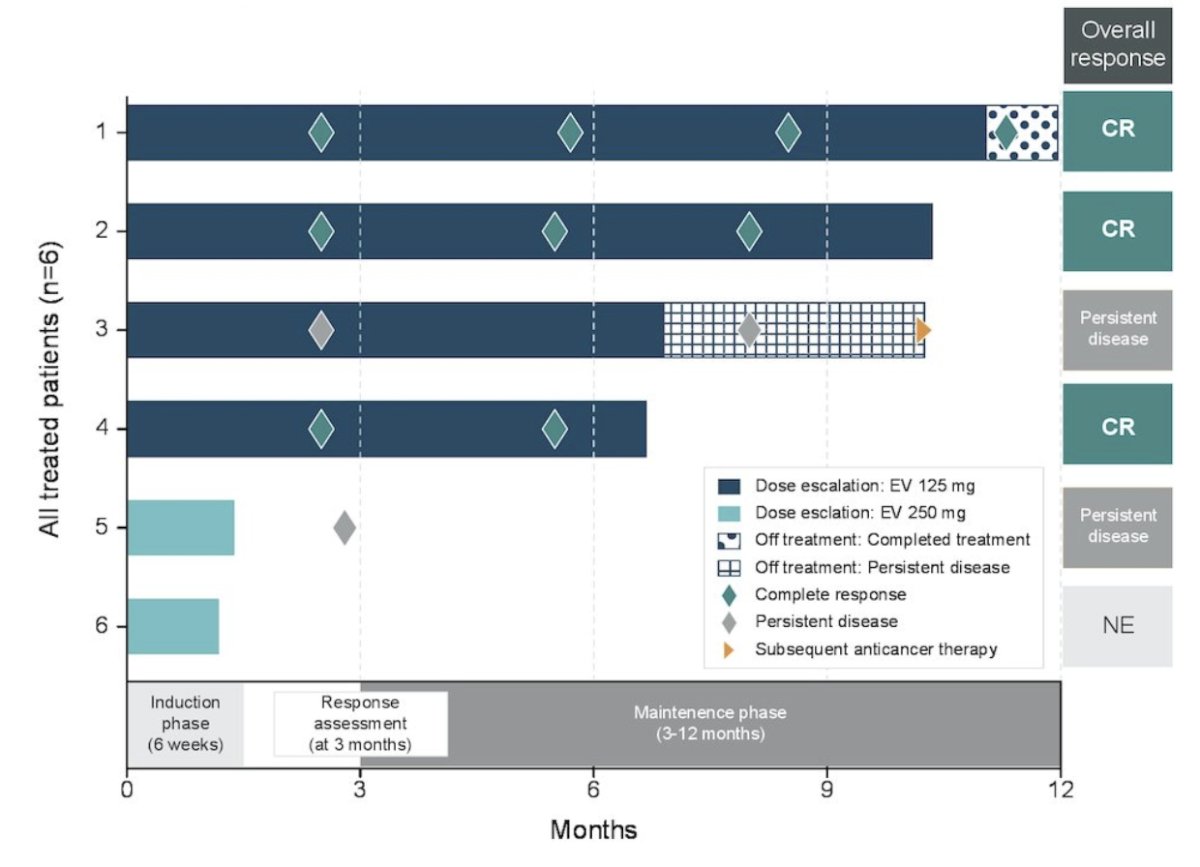
Dr. Gomella then discussed the EV-104 trial, the first in human trial of intravesical enfortumab vedotin in patients with non muscle invasive bladder cancer. Enfortumab vedotin is an antibody drug conjugate that works by targeting and binding to cells expressing the Nectin-4 protein. EV-104 is assessing the antitumor activity of intravesical enfortumab vedotin in patients with high-risk BCG-unresponsive non muscle invasive bladder cancer with CIS with or without papillary disease who are ineligible for or refuse radical cystectomy. At the time of initial data presentation, among 4 patients receiving 125 mg of intravesical enfortumab vedotin, 3 achieved complete response and continue in response. The fourth patient discontinued treatment due to persistent disease but remains on study:
As of February 19, 2025, the FDA has authorized ImmunityBio to provide recombinant BCG to urologists to address the TICE BCG shortage. This expanded use is flexible, with or without the use of N-803. Importantly, many more strains of BCG are in development: BCG-S1PT, BCG-IL-15, rBCG-INF-alpha, VPM1002BC, and BCG-disA-OE.
Next, Dr. Gomella discussed the SunRISe bladder series, which has several ongoing trials:
- SunRISe-1: phase 2 trial of TAR-200 with cetrelimab, TAR-200 alone, or cetrelimab alone for BCG-unresponsive high risk non muscle invasive bladder cancer with CIS ineligible for a radical cystectomy
- SunRISe-2: a trial assessing TAR-200 + cetrelimab versus chemoradiotherapy in muscle invasive bladder cancer
- SunRISe-3: TAR-200 + cetrelimab or TAR-200 versus intravesical BCG with BCG-naïve high risk non muscle invasive bladder cancer
- SunRISe-4: TAR-200 + cetrelimab or cetrelimab alone as neoadjuvant therapy with muscle invasive bladder cancer who are ineligible/refuse neoadjuvant platinum-based chemotherapy
- SunRISe-5: TAR-200 versus intravesical chemotherapy (mitomycin C/gemcitabine) with recurrent high-risk non muscle invasive bladder cancer after BCG (maintenance)
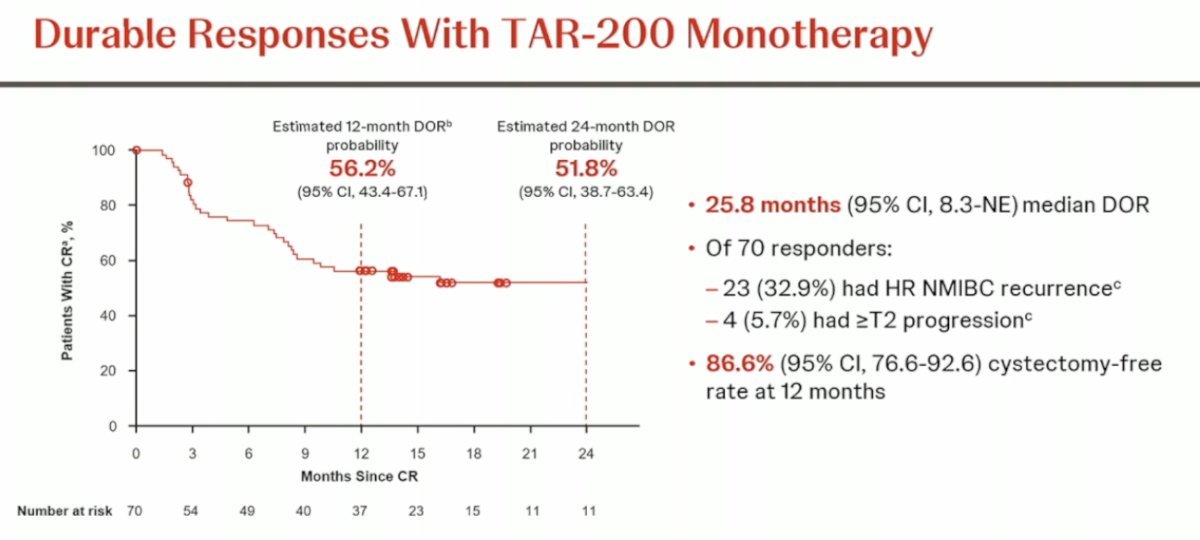
TAR-200 demonstrated promising results for TAR-200 monotherapy in patients with BCG-unresponsive, high risk CIS (+/- papillary disease), with a 48 week complete response rate of 73%, supporting further investigation of TAR-200 monotherapy in other cohorts of patients with high risk non muscle invasive bladder cancer. At the AUA 2025, 1-year durability results and patient reported outcomes were presented for SunRISe-1. The estimated 12-month duration of response rate was 56.2%, with a median duration of response of 25.8 months. Additionally, 86.6% of patients remained cystectomy-free at one year:
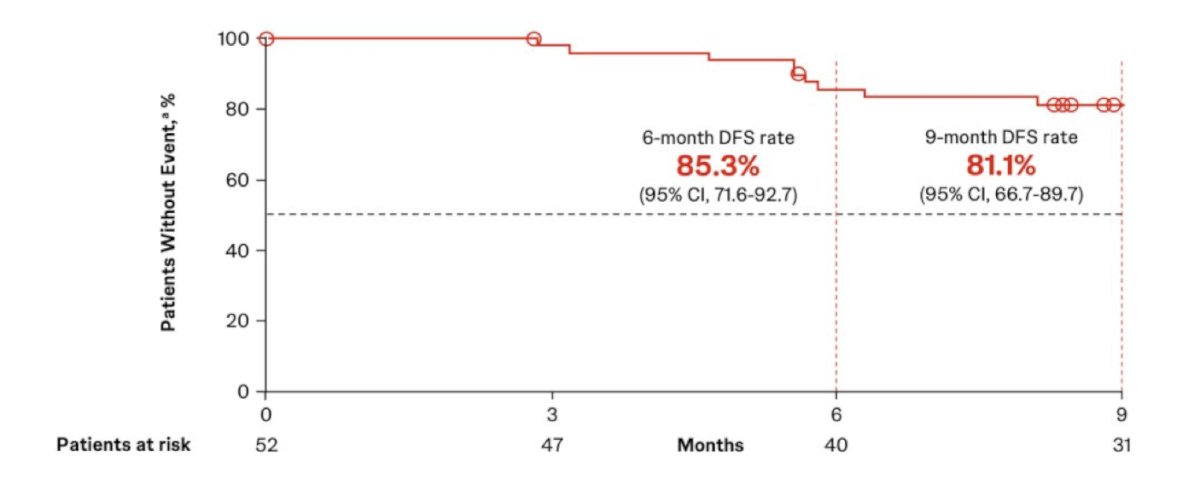
Also presented at AUA 2025 was cohort 4 of SunRISe-1 assessing TAR-200 monotherapy in patients with BCG unresponsive papillary only high risk disease:
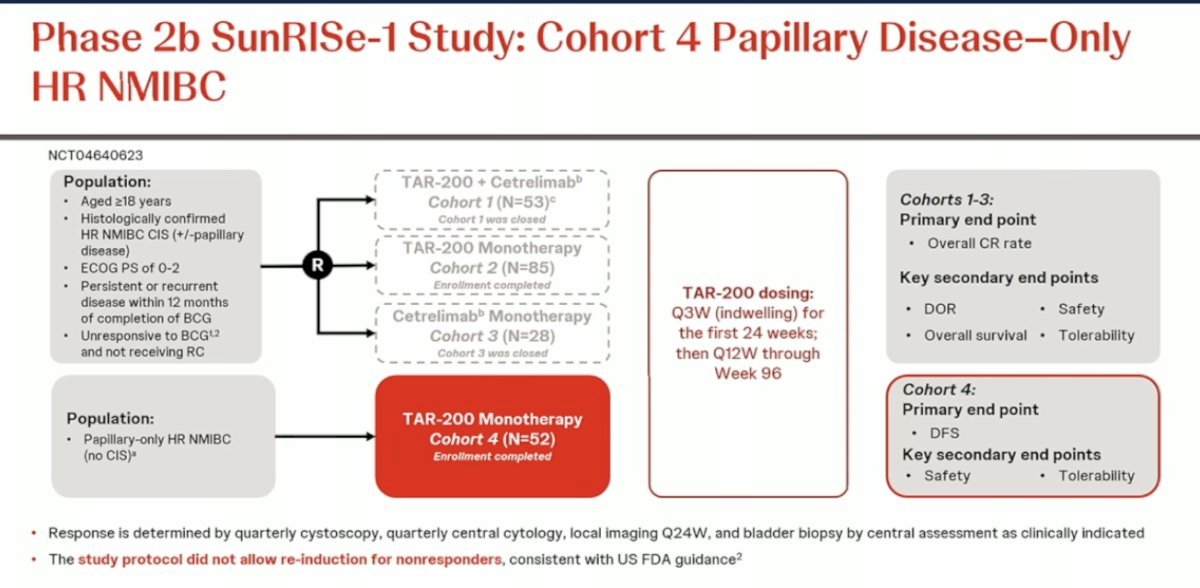
With a median follow-up of 12.8 months, the median disease free survival was not reached (95% CI 12.1–not estimable), and the disease free survival rates at 6 and 9 months were 85.3% and 81.1%, respectively. Overall, only 5.8% of patients (3 of 52) underwent radical cystectomy:
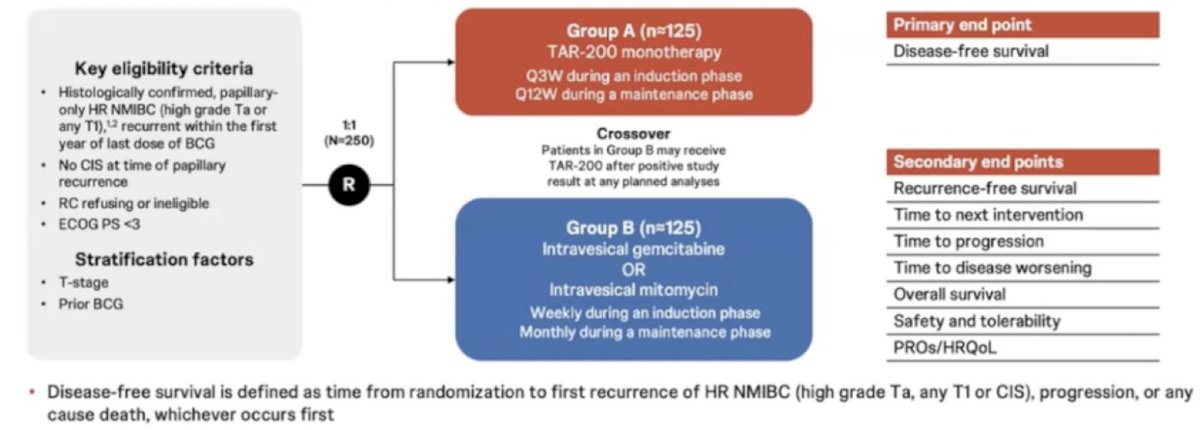
The ongoing SunRISe-5 study, comparing TAR-200 monotherapy to intravesical chemotherapy (gemcitabine or mitomycin C) in patients with BCG-unresponsive or BCG-experienced papillary-only high-risk non muscle invasive bladder cancer, will provide further evidence supporting TAR-200’s potential in this setting:
Dr. Gomella then discussed the AUA 2025 updated results of the ENVISION trial assessing UGN-102 in low grade intermediate risk non muscle invasive bladder cancer. UGN-102 is a reverse thermal gel containing mitomycin developed as a non-surgical treatment option for these patients:

ENVISION is an ongoing, multinational, single-arm, phase III trial in patients with a biopsy-proven recurrence of untreated low grade intermediate risk non muscle invasive bladder cancer [1]. Eligible patients received 6 weekly intravesical instillations of UGN-102 and were evaluated at three months. Patients achieving complete response (negative cystoscopic examination, cytology, and for-cause biopsy) underwent regular surveillance until recurrence, progression, or death. Patients who remained disease-free were planned for long-term follow-up (up to 5 years). Conversely, patients without a complete response at 3 months were offered standard of care therapy. The primary endpoint was 3-months complete response:
![ENVISION is an ongoing, multinational, single-arm, phase III trial in patients with a biopsy-proven recurrence of untreated low grade intermediate risk non muscle invasive bladder cancer [1]. Eligible patients received 6 weekly intravesical instillations of UGN-102 and were evaluated at three months. Patients achieving complete response (negative cystoscopic examination, cytology, and for-cause biopsy) underwent regular surveillance until recurrence, progression, or death. Patients who remained disease-free were planned for long-term follow-up (up to 5 years). Conversely, patients without a complete response at 3 months were offered standard of care therapy. The primary endpoint was 3-months complete response:](/images/com-doc-importer/220-interdisciplinary-gu-cancer-forum-2025/interdisciplinary-gu-cancer-forum-2025-novel-agents-in-nmibc/image-9.jpg)
Of 240 patients enrolled, 228 (95%) received all 6 planned doses. The 3-months complete response rate was 80% (95% CI 74–84.5%), with an 81% (95% CI 74–86%) probability of a maintained response at 12 months. The median duration of response was not estimable over a median 13.9-month follow-up period: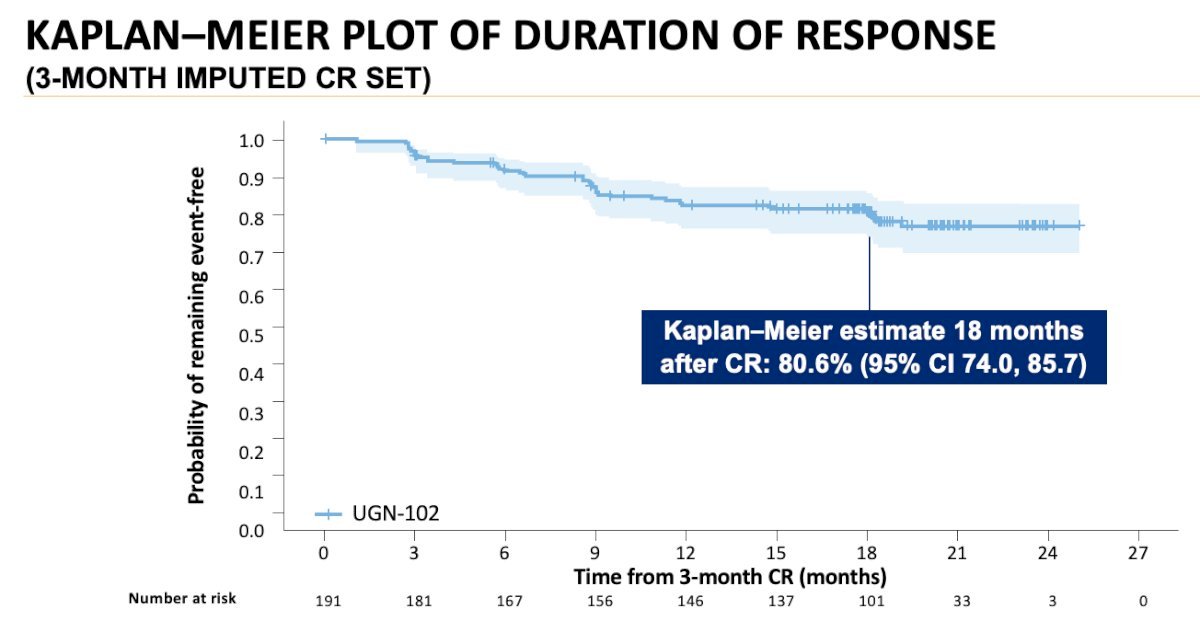
Based on the results from ENVISION, on June 12, 2025, the FDA approved mitomycin for intravesical solution (Zusduri; formerly UGN-102) for the treatment of adult patients with recurrent low-grade intermediate-risk non–muscle invasive bladder cancer.
Also at AUA 2025, updated results of BOND-003 cohort C were presented, assessing cretostimogene grenadenorepvec for high risk BCG-unresponsive non muscle invasive bladder cancer with CIS. Cretostimogene grenadenorepvec is a conditionally replicating, highly immunogenic adenovirus regulated by the human E2F-1 promoter, enabling selective targeting of tumors with RB-E2F pathway alterations. It also encodes the GM-CSF transgene. The virus binds to the Coxsackie adenovirus receptor, which is expressed across all stages of bladder cancer. As an oncolytic immunotherapy, it exerts a dual mechanism of action: viral replication induces tumor lysis and stimulates a robust immune response:

A total of 112 patients were enrolled, all with pathologically confirmed high-risk BCG-unresponsive non muscle invasive bladder cancer with CIS, with or without high-grade Ta/T1 disease. All high-grade Ta/T1 tumors were resected prior to treatment. Patients received an induction course of cretostimogene administered weekly for six weeks, with a second induction course offered to non-responders. Maintenance therapy was given weekly for three weeks every three months during the first year, and every six months during years two and three. The primary endpoint was complete response at any time, with central pathology review and the requirement for mandatory biopsies at 12 months. The study schema of BOND-003 is shown below:
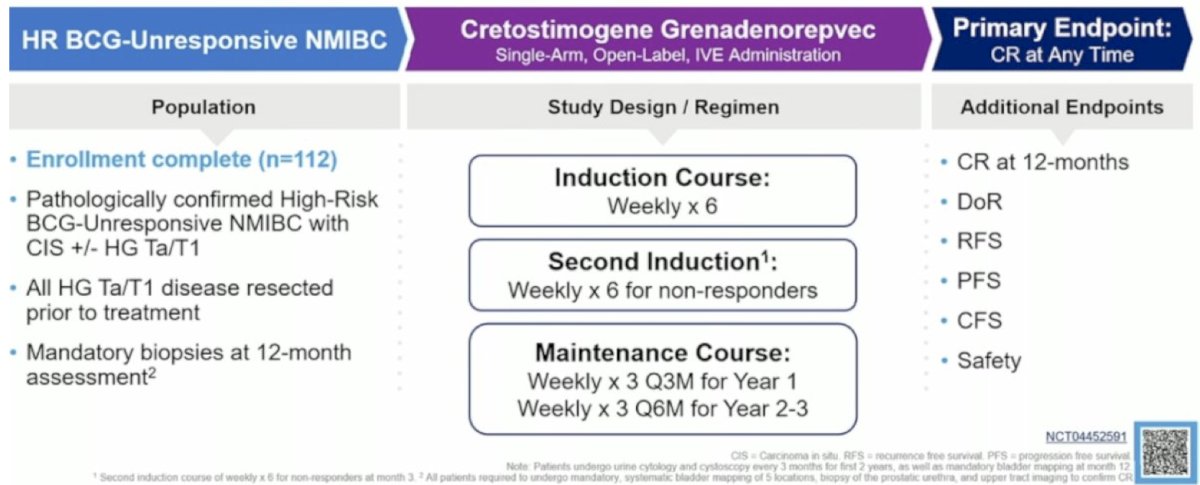
The overall complete response rate was 75.5%, with 46.4% of patients maintaining a complete response at 1 year and 33.7% at 2 years. At 24 months, 97.3% of patients were free from progression to muscle-invasive bladder cancer, and 84.5% had avoided radical cystectomy, highlighting the bladder-sparing potential of cretostimogene. Among patients who underwent radical cystectomy, 82.4% (14 out of 17) had either pT0 or non–muscle-invasive disease. Dr. Gomella notes that the SUO-CTC has two additional trials ongoing.
- PIVOT-006: a phase 3 trial of adjuvant cretostimogene versus TURBT alone in intermediate risk non muscle invasive bladder cancer
- CORE-008: a phase 2 multi-arm, multi-cohort trial of cretostimogene in high-risk non muscle invasive bladder cancer, with cohort A enrolling BCG-naïve patients, cohort B enrolling BCG exposed patients, and with additional cohorts under design
Dr. Gomella then discussed the initial results of the CREST trial,3 presented at AUA 2025. CREST is a three-arm study comparing different combinations of sasanlimab and BCG. Arm A received sasanlimab administered subcutaneously combined with BCG induction and maintenance, Arm B received sasanlimab with BCG induction only, and Arm C received BCG induction and maintenance alone. The primary endpoint was event-free survival, defined as recurrence of high-grade disease, progressive disease, persistence of CIS, or death from any cause: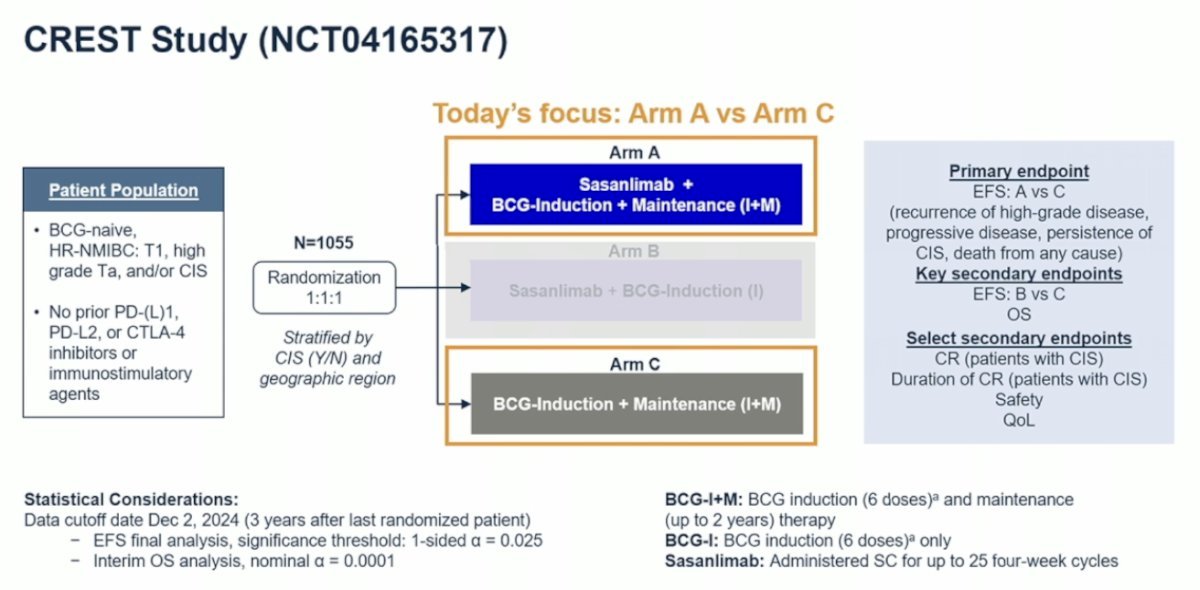
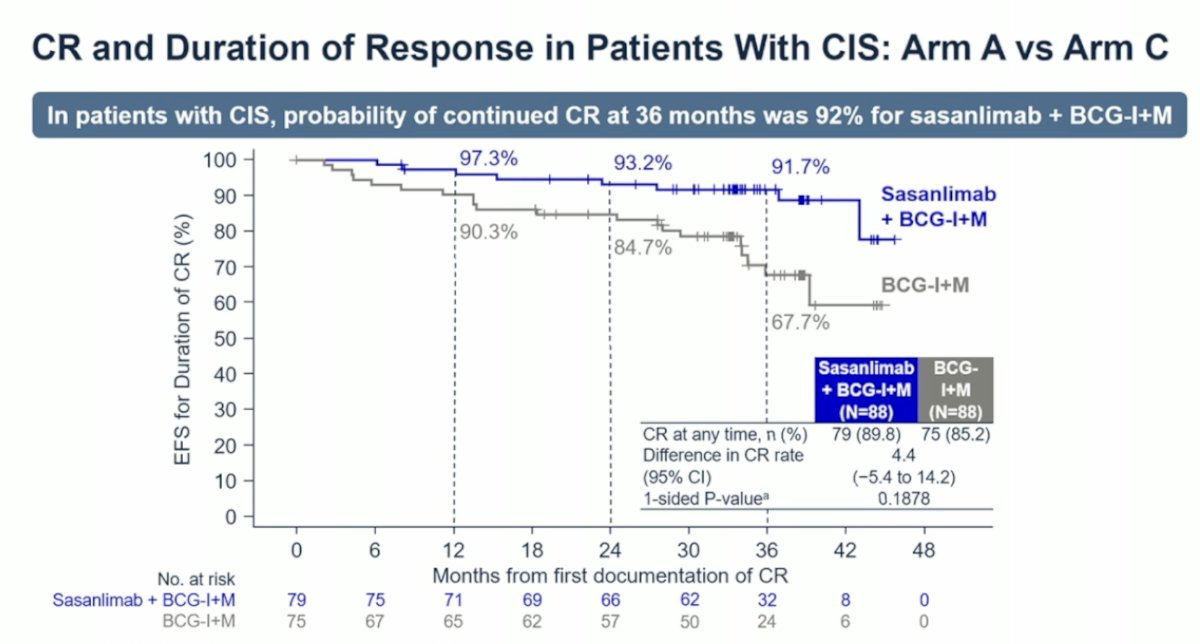
The risk of experiencing an event free survival event was 32% lower with sasanlimab + BCG compared to BCG induction and maintenance alone (stratified HR 0.68, 95% CI 0.49–0.94; 1-sided p-value: 0.0095). In patients with CIS, the probability of maintaining a complete response at 36 months was 91.7% with sasanlimab + BCG induction and maintenance, compared to 67.7% with BCG induction and maintenance alone:
Finally, Dr. Gomella discussed an artificial intelligence platform developed and trained to quantify morphologic features which, combined with key clinical features, create multimodal assays:
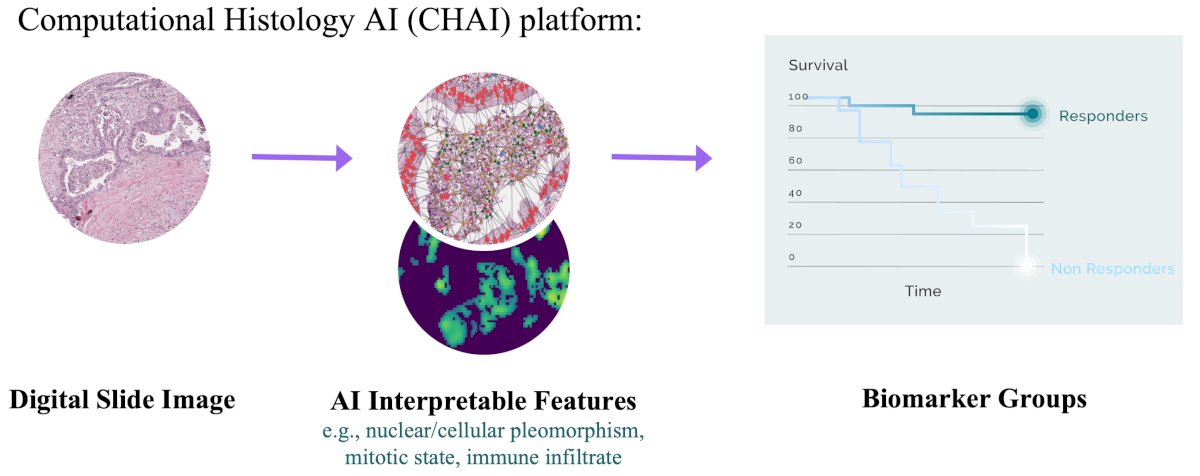
The computational histology artificial intelligence biomarker identifies cases of high risk BCG unresponsive disease:
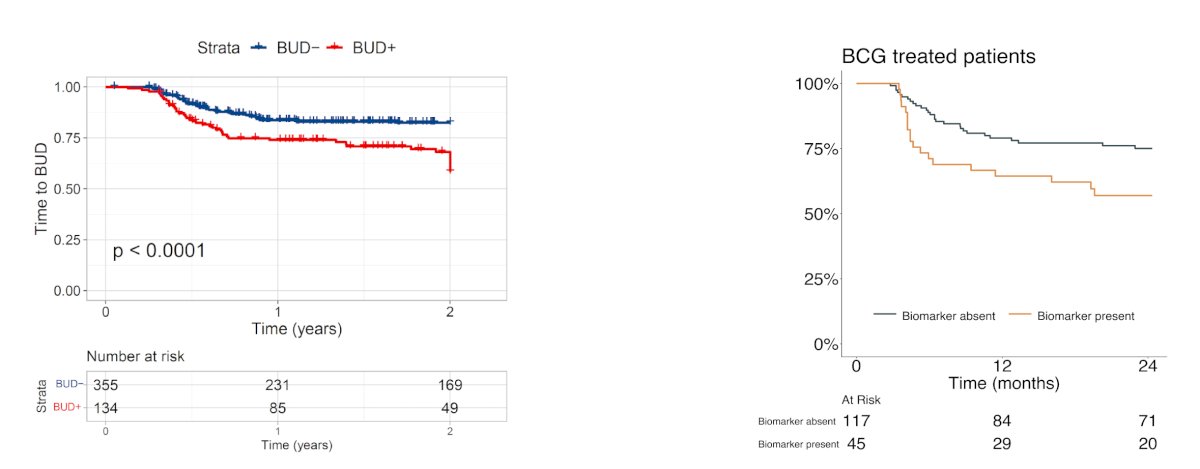
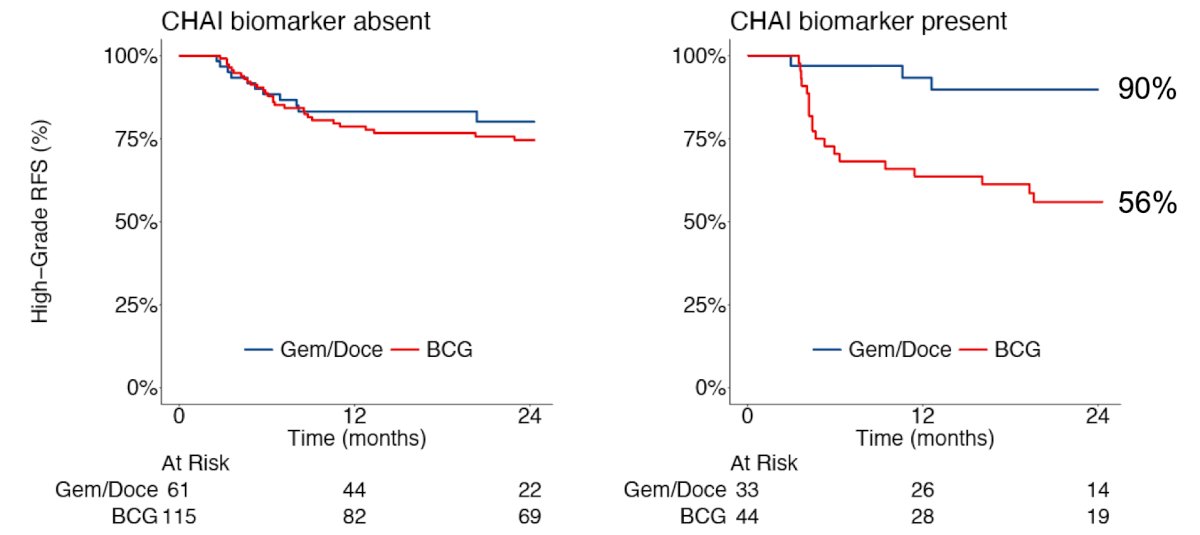
Additionally, the computational histology artificial intelligence biomarker predicts differential treatment benefit: biomarker positive patients have improved high grade recurrence free survival on gemcitabine + docetaxel versus BCG:
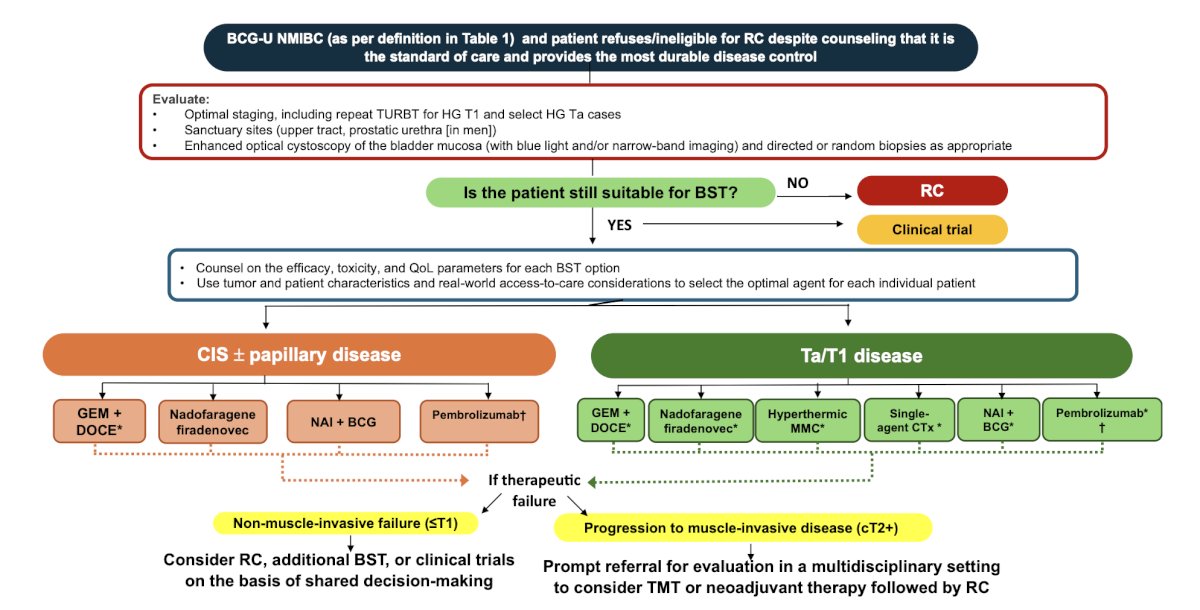
The International Bladder Cancer Group has recently provided recommendations for optimal sequencing and patient selection among patients with BCG unresponsive non muscle invasive bladder cancer.4 For patients with BCG-unresponsive CIS, gemcitabine + docetaxel, nadofaragene firadenovec, and NAI + BCG are recommended; because of its systemic toxicity, pembrolizumab should only be offered after other options are exhausted. For patients with BCG-unresponsive papillary-only tumors, gemcitabine + docetaxel, nadofaragene firadenovec, NAI + BCG, single-agent chemotherapy, hyperthermic mitomycin C, and pembrolizumab are recommended:
Dr. Gomella concluded his presentation discussing novel agents in non muscle invasive bladder cancer with the following take home points:
- BCG remains the gold standard
- There has been a major increase in non muscle invasive bladder cancer options over the last 10 years:
- Low grade disease: 15 year progression free survival is up to 95% and <1% cancer specific mortality
- High grade disease: outcomes can vary greatly – 5 year recurrence free survival of 17-89%, while overall survival ranges from 28-90%
- While cystectomy is still recommended for BCG refractory high grade disease, these newer options may allow bladder preservation
- Many novel intravesical approaches are under study, focusing on high grade disease
Presented by: Leonard Gomella, MD, FACS, Thomas Jefferson University, Philadelphia, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Interdisciplinary Genitourinary Cancer Forum, St. Petersburg, FL, Thurs, Jun 19 – Sat, Jun 21, 2025.
References:
- Ghodoussipour S, Bivalacqua T, Bryan RT, et al. A systematic review of novel intravesical approaches for the treatment of patients with non-muscle-invasive bladder cancer. Eur Urol. 2025 Jul;88(1):33-55.
- Prasad SM, Shishkov D, Vladimirov Mihaylov N, et al. Primary Chemoablation of Recurrent Low-Grade Intermediate-Risk Nonmuscle-Invasive Bladder Cancer with UGN-102: A Single-Arm, Open-Label, Phase 3 Trial (ENVISION). J Urol. 2025 Feb;213(2):205-216.
- Shore ND, Powles TB, Bedke J, et al. Sasanlimab plus BCG in BCG-naïve, high-risk non-muscle invasive bladder cancer: The randomized phase 3 CREST trial. Nat Med. 2025 May 31 [Epub ahead of print].
- Li R, Hensley PJ, Gupta S, et al. Bladder-sparing therapy for Bacillus Calmette-Guerin-unresponsive non-muscle-invasive Bladder Cancer: International Bladder Cancer Group Recommendations for Optimal Sequencing and Patient Selection. Eur Urol. 2024 Aug 24;S0302-2838(24)02516-8.