(UroToday.com) The 2025 Interdisciplinary Genitourinary Cancer Forum featured a muscle invasive bladder cancer session and a presentation by Dr. Daniel Petrylak discussing new approaches to neoadjuvant therapy for urothelial carcinoma. Cisplatin-based neoadjuvant chemotherapy is recommended for patients with clinical stage T2 muscle invasive bladder cancer or higher.
However, there are patients who should not receive cisplatin-based chemotherapy, including those with (i) renal impairment or other comorbidities (such as cardiac disease), and (ii) poor performance status (ECOG status >= 2).
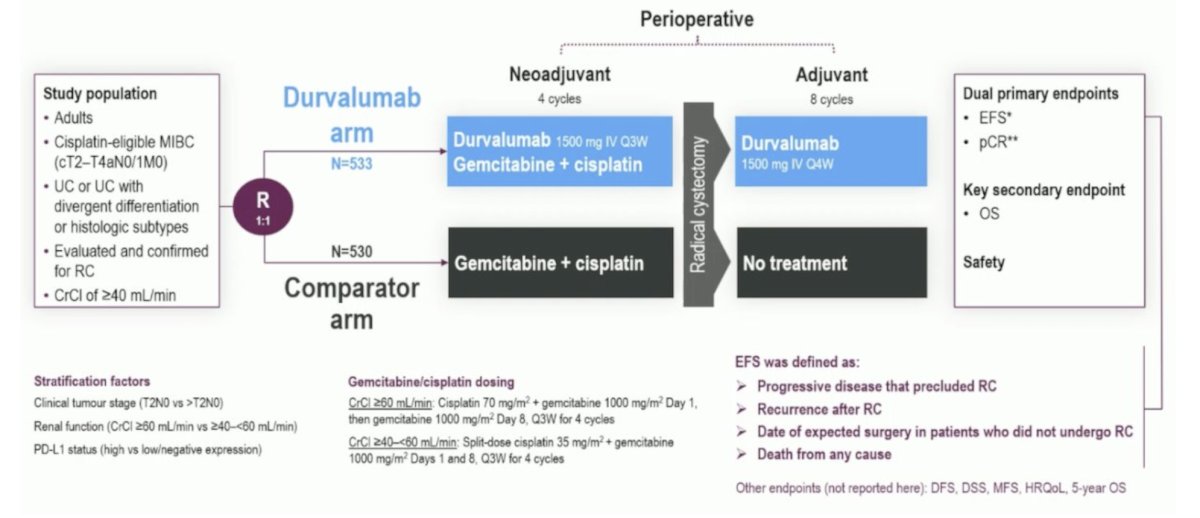
The NIAGARA trial was initially presented at ESMO 2024, the first phase 3 trial testing perioperative immune checkpoint inhibitor (durvalumab) combined with neoadjuvant chemotherapy in cisplatin-eligible patients with muscle-invasive bladder cancer. NIAGARA enrolled patients with cisplatin-eligible muscle invasive disease (cT2-TaN0/1M0), including those with divergent differentiation or histologic subtypes. In the durvalumab arm, patients were randomized to receive durvalumab 1500 mg IV every 3 weeks with gemcitabine + cisplatin for 4 cycles, followed by radical cystectomy and adjuvant durvalumab 1500 mg IV every 4 weeks for up to 8 cycles. In the comparator arm, patients were randomized to receive gemcitabine + cisplatin followed by radical cystectomy and did not receive any adjuvant treatment. The dual primary endpoints were:
- Event-free survival: defined as progressive disease that precluded radical cystectomy, recurrence after radical cystectomy, failure to undergo radical cystectomy by the expected surgery date, or death from any cause.
- Pathological complete response rate: evaluated by blinded central pathology review
The trial design for NIAGARA is as follows:
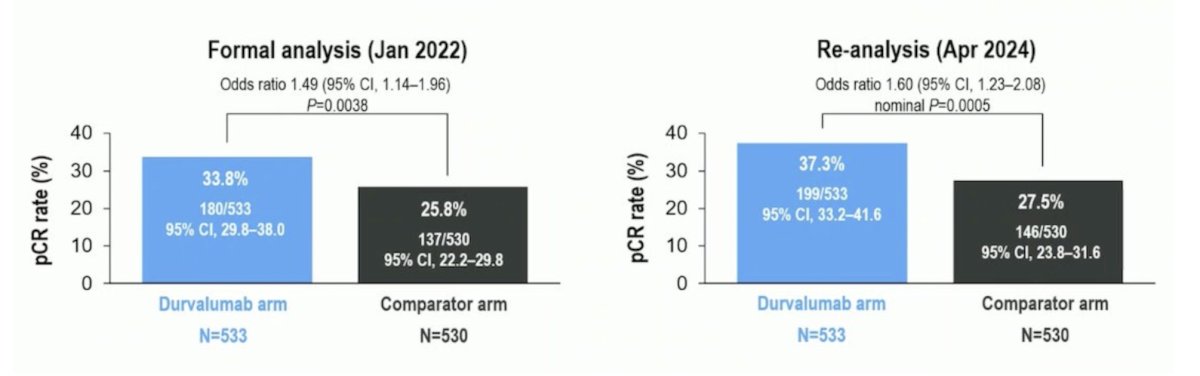
Pathological complete response was reported in two separate analyses: a formal analysis in January 2022 and a re-analysis in April 2024. The planned formal analysis for pathological complete response was not statistically significant (p = 0.0038) as the threshold for significance was a p-value of 0.001. However, this analysis incorrectly classified 59 evaluable samples as non-responders, and in a re-analysis (which included these 59 samples and identified 28 additional pathological complete responses) there was nominal statistical significance in favor of the durvalumab arm (p = 0.0005):
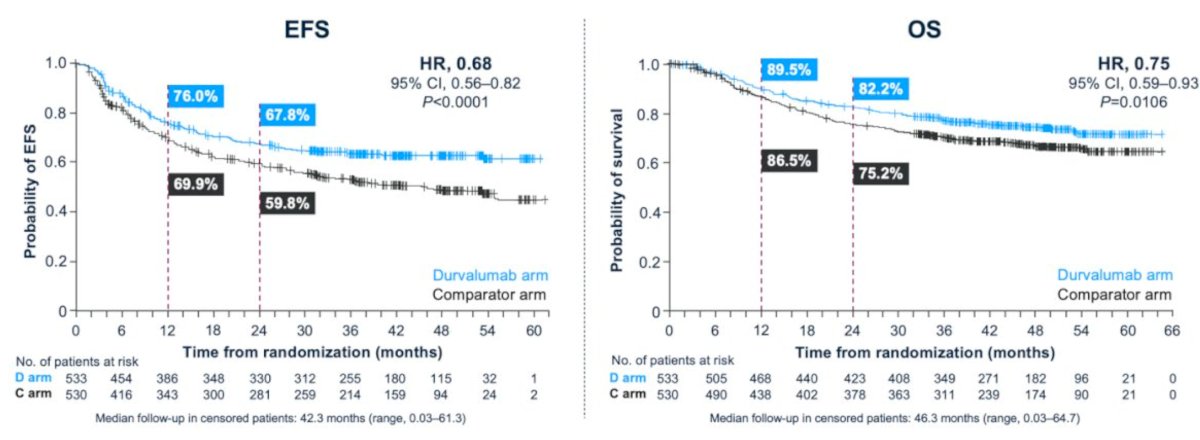
Event free survival in the intention-to-treat population showed a 2 year rate of 67.8% in the durvalumab arm compared to 59.8% in the comparator arm (HR 0.68, 95% CI 0.56-0.82, p < 0.0001). With regards to overall survival, the 2 year rate was 82.2% for patients in the durvalumab arm compared to 75.2% in the comparator arm (HR 0.75, 95% CI 0.59–0.93, p = 0.016):
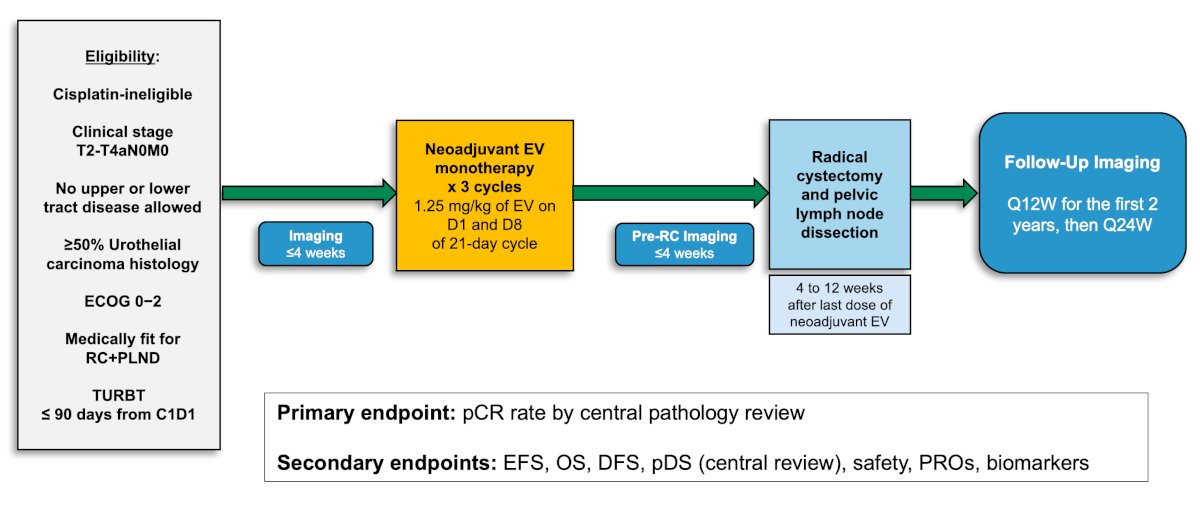
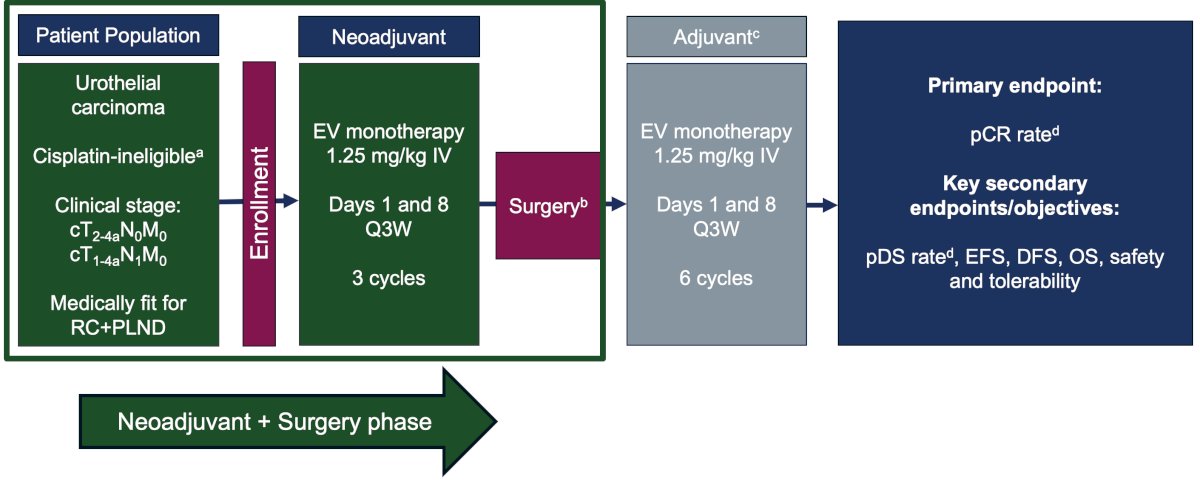
Next, Dr. Petrylak discussed the EV-103 cohort H trial, which enrolled patients with cisplatin ineligible cT2-T4aN0M0 muscle invasive bladder cancer who were eligible for radical cystectomy and pelvic lymph node dissection and had an ECOG of 0-2. Patients received 3 cycles of neoadjuvant enfortumab vedotin (1.25 mg/kg) on Days 1 and 8 of every 3-week cycle prior to radical cystectomy and pelvic lymph node dissection. The primary endpoint of the study was pathological complete response rate (ypT0N0) by central review. Key secondary endpoints included pathological downstaging rate (yp T0,Tis,Ta,T1,N0) and safety. The trial design for EV-103 cohort H is as follows:
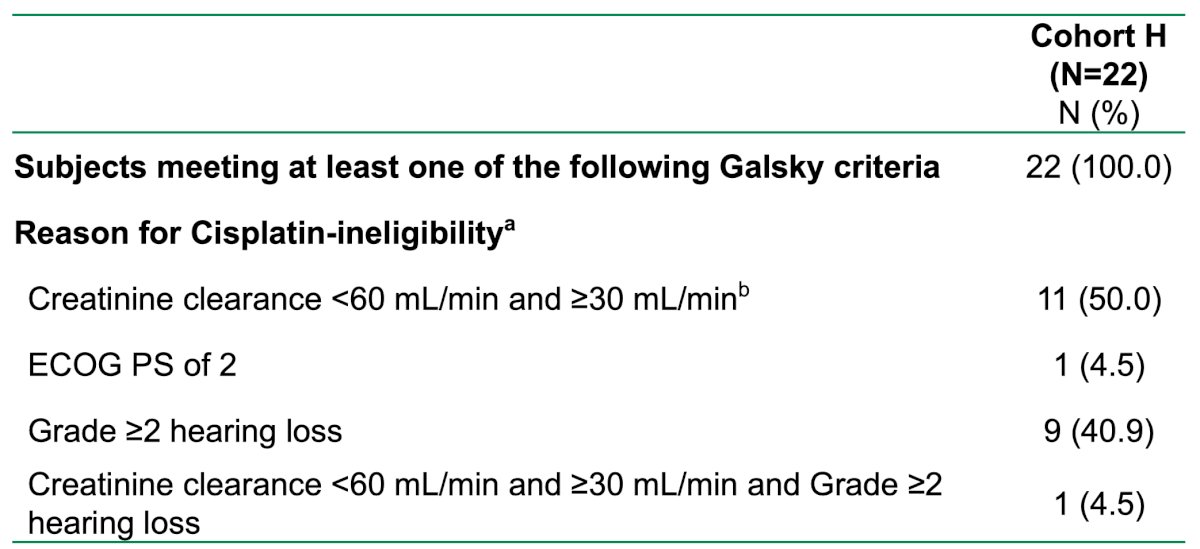
There were 22 patients treated, with the following clinical stage: cT2 (68.2%), cT3 (27.3%), and cT4 (4.5%) tumors. Among these patients, 68.2% patients had predominant urothelial cancer and 31.8% had a mixed histology:

The most common reasons for cisplatin ineligibility included creatinine clearance <60 mL/min (50%) and Grade >=2 hearing loss (40.9%):
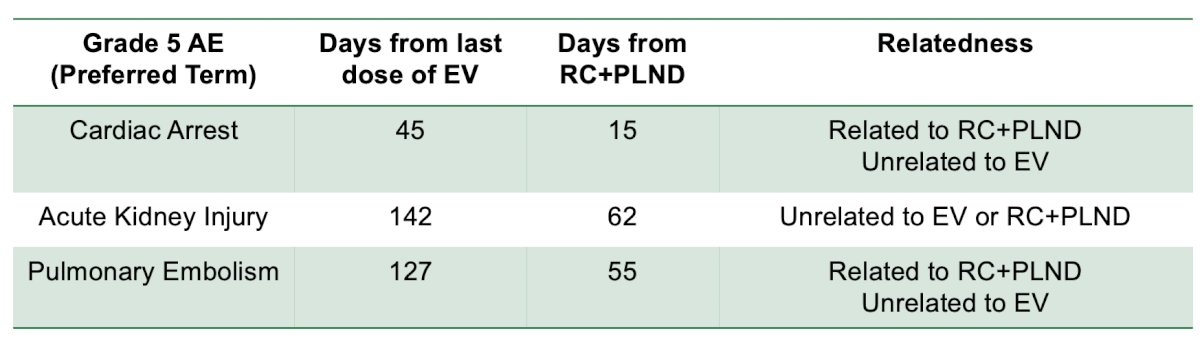
Overall, 36.4% (95% CI 17.2-59.3) of patients had a pathological complete response, and pathological downstaging was seen in 50.0% (95% CI 28.2-71.8) of patients. The most common enfortumab vedotin treatment-related adverse events were fatigue (45.5%), alopecia (36.4%), and dysgeusia (36.4%). There were 18.2% of patients that had Grade ≥3 enfortumab vedotin treatment-related adverse events. No surgeries were delayed due to enfortumab vedotin administration. There were three patients that had Grade 5 adverse events while on study that was unrelated to enfortumab vedotin, and in two patients these adverse events occurred > 30 days after radical cystectomy and pelvic lymph node dissection (one cardiac arrest, one pulmonary embolism):
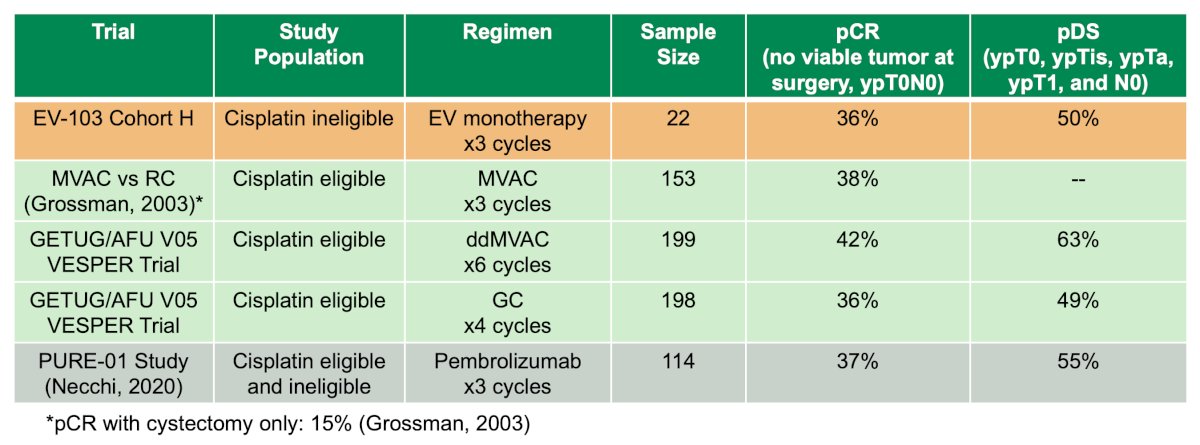
Dr. Petrylak noted that neoadjuvant enfortumab vedotin elicited pathological complete response rates in cisplatin-ineligible patients comparable to cisplatin-based chemotherapy in the cisplatin-eligible setting:
EV-103 cohort L was initially presented at ESMO 2023, assessing enfortumab vedotin monotherapy in cisplatin-ineligible patients with muscle invasive bladder cancer. Following enrollment, patients were given enfortumab vedotin monotherapy (1.25 mg/kg) in 3-week cycles on days 1 and 8 for 3 cycles total. Following surgery, patients received the same regimen for 6 cycles. The primary endpoint was pathological complete response, with secondary objectives of pathologic downstaging, event-free survival, disease-free survival, overall survival, and safety and tolerability:
Cohort L included 51 patients, with a median age of 74 years (range: 54-85), and 96% of patients having an ECOG performance status 0 – 1. The baseline stage was cT2N0 for 57% and cN+ for 10% of patients. 45% of patients had a creatinine clearance of 30 – 60 mL/min:

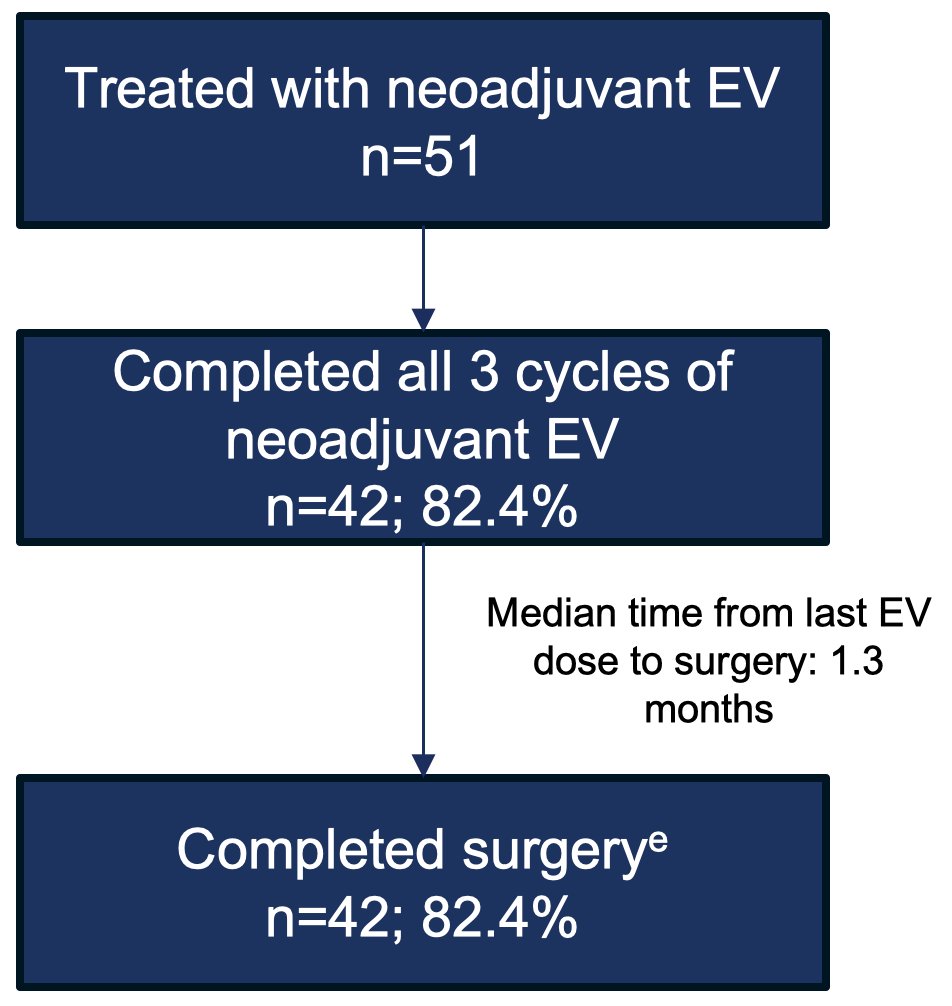
82.4% of patients completed all 3 cycles of neoadjuvant enfortumab vedotin, with all these patients completing surgery within a median time of 1.3 months from the last enfortumab vedotin dose:
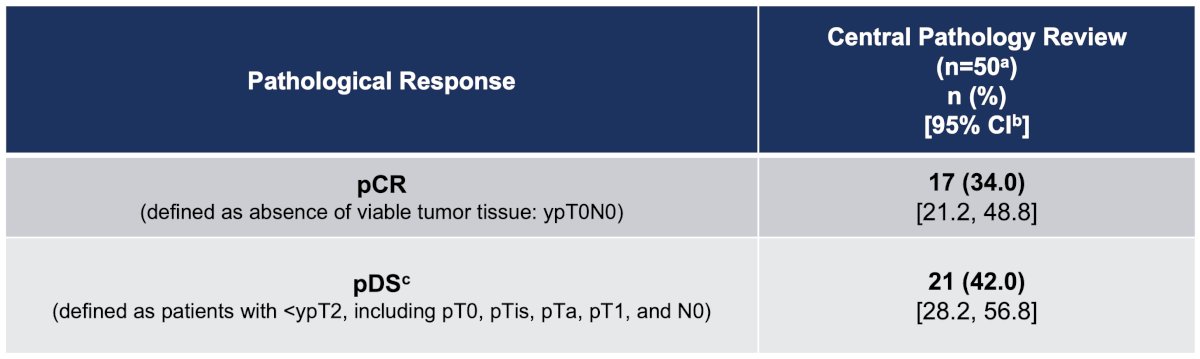
For pathologic outcomes, the pathological complete response rate was 34% and pathological downstaging occurred in 42% of patients:
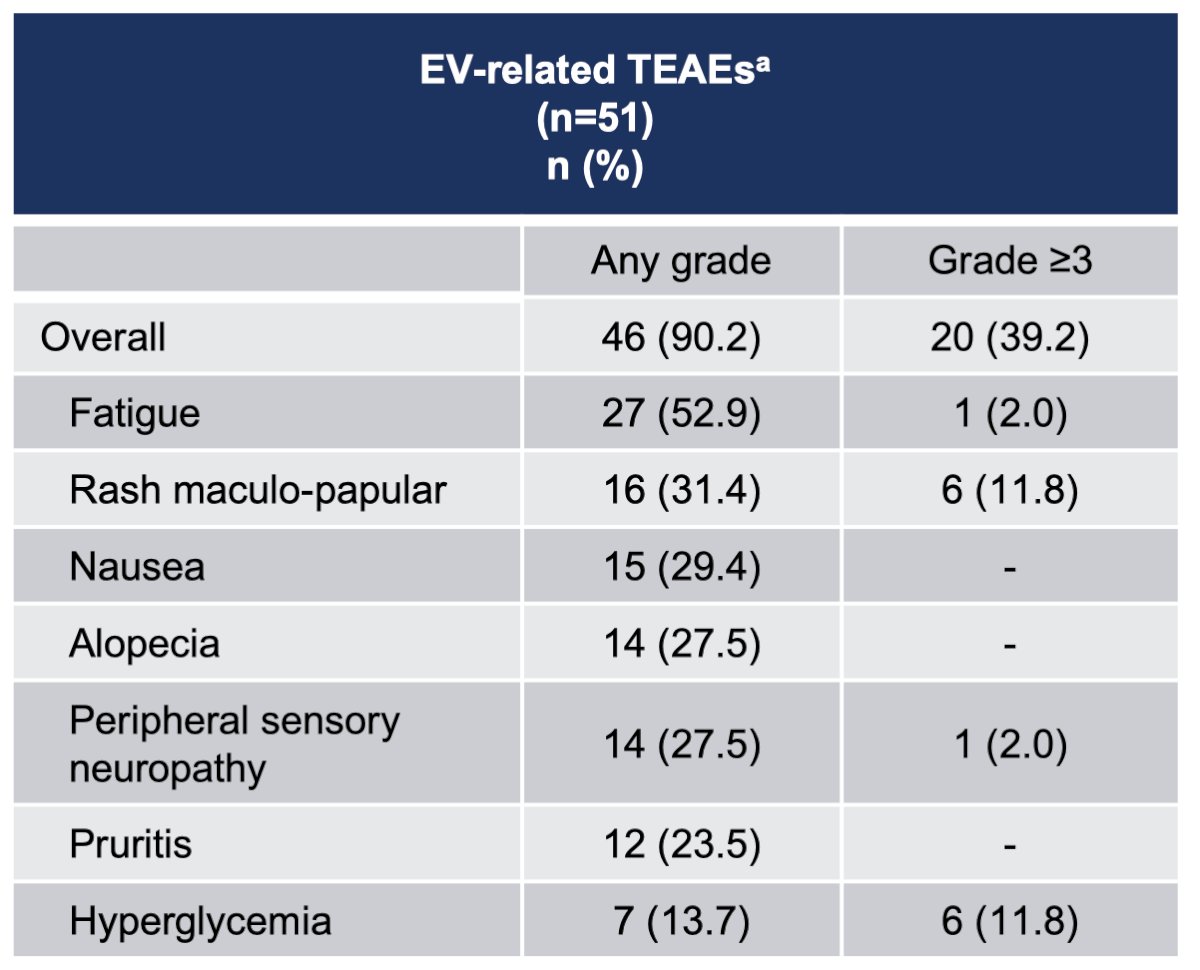
The majority of enfortumab vedotin-related adverse events were grade 2 or lower, with 57% of patients having skin reactions, and 1 patient dying of Stevens-Johnson syndrome. A third of patients had peripheral neuropathy. There were no delays to surgery secondary to enfortumab vedotin-related treatment-emergent adverse events. The most common grade 3 or worse surgery-related adverse events were anemia, ileus, and urinary tract infection:
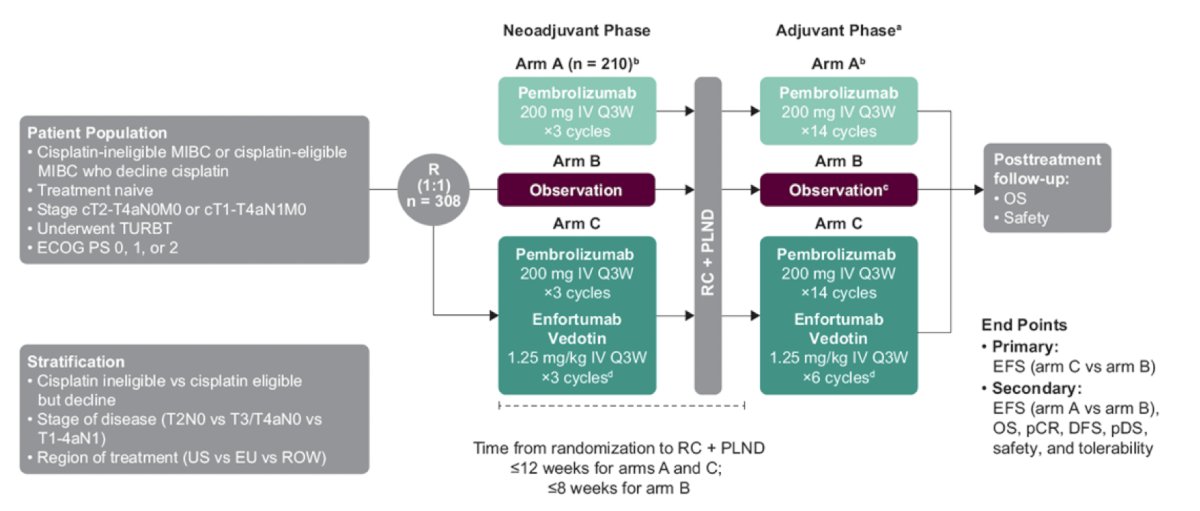
Dr. Petrylak finished his presentation discussing two key phase 3 trials in the perioperative therapy disease space. The first he discussed was the KEYNOTE-905/EV-303 trial assessing the efficacy and safety of perioperative pembrolizumab alone or combined with enfortumab vedotin versus radical cystectomy + pelvic lymph node dissection alone in patients with muscle invasive bladder cancer who are ineligible for or decline cisplatin-based treatment. Patients will be randomized to three arms:
- Arm A: neoadjuvant pembrolizumab 200 mg IV every 3 weeks for ≤3 cycles followed by radical cystectomy + pelvic lymph node dissection and adjuvant pembrolizumab 200 mg IV every 3 weeks for ≤14 cycles
- Arm B: radical cystectomy + pelvic lymph node dissection followed by observation (adjuvant nivolumab permitted based on clinical indication and regulatory approval)
- Arm C: neoadjuvant enfortumab vedotin 1.25 mg/kg + pembrolizumab 200 mg IV every 3 weeks for ≤3 cycles followed by radical cystectomy + pelvic lymph node dissection and adjuvant enfortumab vedotin + pembrolizumab for ≤6 cycles and adjuvant pembrolizumab 200 mg IV every 3 weeks for ≤8 cycles
In the neoadjuvant and adjuvant phases of arm C, pembrolizumab will be administered on day 1 and enfortumab vedotin will be administered on days 1 and 8 of each cycle. Enrollment is complete for arm A, whereas patients will continue to be randomly assigned 1:1 to arm B or arm C. The trial design for KEYNOTE-905/EV-303 is as follows:
The second trial is the VOLGA trial assessing durvalumab, tremelimumab, and enfortumab vedotin compared to durvalumab and enfortumab vedotin as neoadjuvant therapy for cisplatin-ineligible patients with muscle-invasive bladder cancer. Patients will be randomized to 3 arms, each receiving 3 cycles of neoadjuvant therapy every 3 weeks as follows:
- Arm 1: patients will receive durvalumab (1500 mg day 1) and tremelimumab (75 mg day 1) and enfortumab vedotin (1.25 mg/kg Days 1 & 8)
- Arm 2: patients receive durvalumab (1500 mg day 1) and enfortumab vedotin (1.25 mg/kg Days 1 & 8)
- Arm 3: patients receive no neoadjuvant treatment (standard of care)
Following radical cystectomy, patients in arm 1 will then receive 1 cycle of tremelimumab on Day 1 plus 9 cycles of durvalumab every 4 weeks while those in arm 2 receive 9 cycles of durvalumab every 4 weeks, and those in arm 3 receive either no adjuvant treatment (observation only) or adjuvant nivolumab in high-risk patients where available and approved (planned amendment). The trial design of VOLGA is as follows:
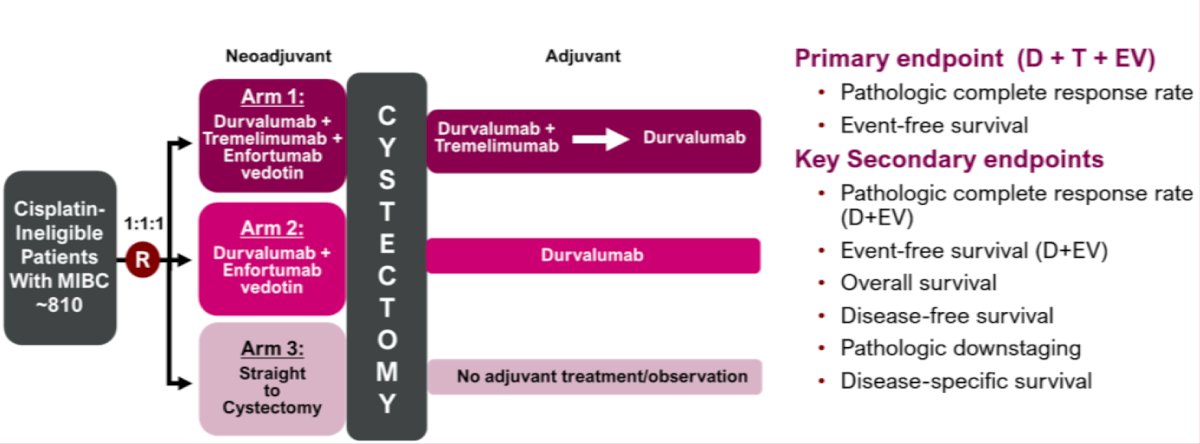
The dual primary endpoints are pathological complete response rate (defined as ypT0N0M0) and event-free survival.
Dr. Petrylak concluded his presentation discussing new approaches to neoadjuvant therapy for urothelial carcinoma with the following take home points:
- Gemcitabine + cisplatin + durvalumab is a standard of care for neoadjuvant therapy of muscle invasive bladder cancer
- Single agent enfortumab vedotin has a pathological complete response rate of 34 % in locally advanced cisplatin ineligible patients
- Phase III studies evaluating neoadjuvant enfortumab combined with checkpoint inhibitors have completed accrual
Presented by: Daniel Petrylak, MD, Professor of Medicine (Medical Oncology) and of Urology, Yale School of Medicine, New Haven, CT
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Interdisciplinary Genitourinary Cancer Forum, St. Petersburg, FL, Thurs, Jun 19 – Sat, Jun 21, 2025.