(UroToday.com) The 2025 Interdisciplinary Genitourinary Cancer Forum featured a management of non muscle invasive bladder cancer session and a presentation by Dr. Bernard Bochner discussing clinical trial design in this disease space. In 2013, the United States FDA and the American Urological Association co-sponsored a public workshop with the following proposed guidance statements:
- Single arm trials are appropriate where a randomized trial is unethical or not feasible
- Randomizing BCG-unresponsive patients to placebo or minimally effective drug raises ethical concerns
- Single arm trials are appropriate because “currently, no effective medical therapies are available, and the only alternative is radical cystectomy”
- If effective therapies become available, “a randomized trial may be appropriate”
Based on this public workshop, the following benchmarks were proposed:
- 6 month complete response rate: 40-50%
- 18-24 months durable response: >=30%, with the 95% confidence interval excluding 20%
Furthermore, the International Bladder Cancer Group set the following benchmarks for BCG-unresponsive CIS:
- Complete response rate of 50% at 6 months
- Durable response rates of 30% at 12 months and 25% at 18 months
There are numerous issues with evaluating treatment efficacy in single arm, non randomized non muscle invasive bladder cancer trials:
- What is the pre-treatment TURBT quality?
- What are the treatment center effects?
- What is the consistency of “enhanced” cystoscopy?
- What is the quality of initial treatments?
- Varying patient populations and tumor risk:
- Prior BCG naïve/exposed treatment history?
- What is the history of contemporary CIS?
- What is the impact of inter-pathologist variability?
- Trial design and methodology variations:
- Treatment failure definitions?
- Is re-treatment allowed?
- Are there protocol biopsies?
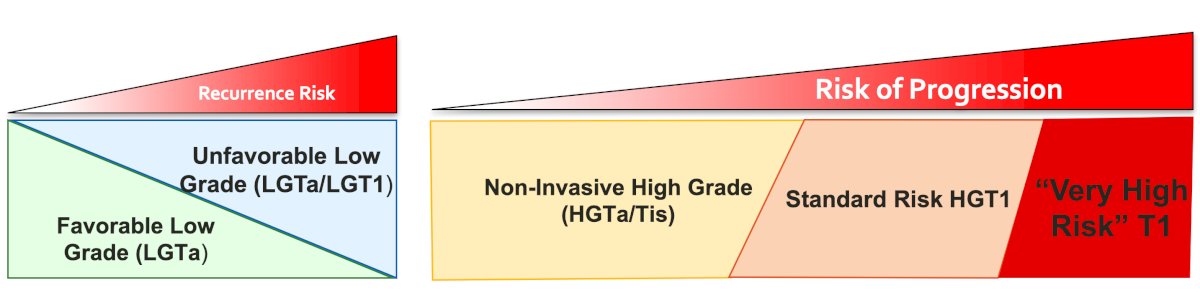
Dr. Bochner provided the following figure highlighting the clinical spectrum of non muscle invasive bladder cancer:
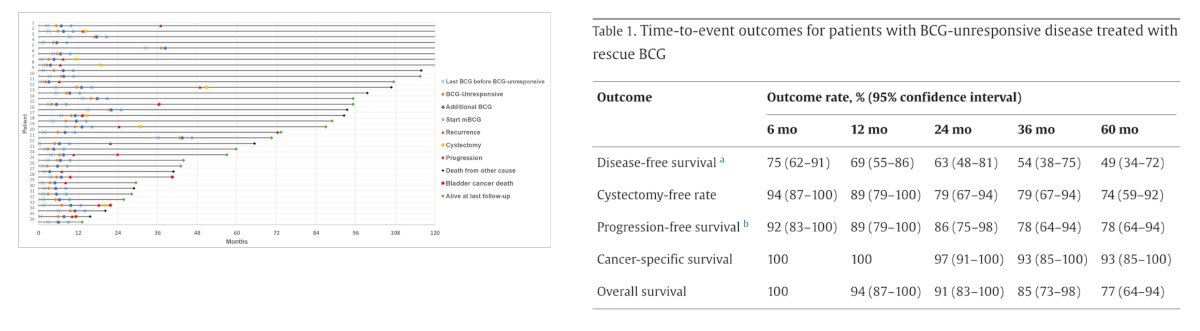
Dr. Bochner then discussed challenging the paradigm of “BCG-unresponsive” bladder cancer and the impact of additional BCG. Work from Dr. Kamat’s group showing that a sub-population of patients that have BCG-unresponsive CIS +/- Ta/T1 may have a response to additional BCG.1 Among 17 patients receiving additional BCG, 14 (83%) had a complete response:
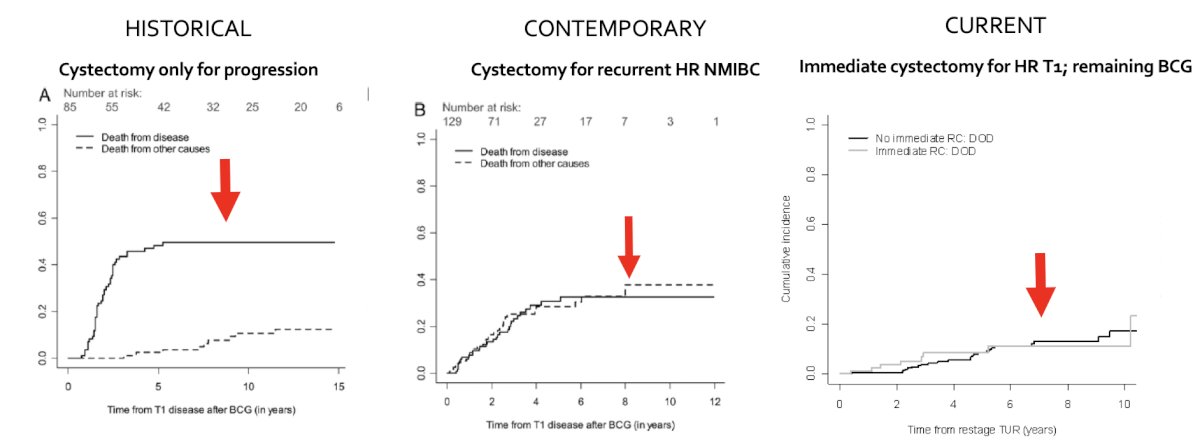
With regards to high risk (T1) bladder cancer, Dr. Bochner notes that there has been changing treatment patterns:
- Historical: cystectomy only for disease progression
- Contemporary: cystectomy for recurrent high risk non muscle invasive bladder cancer
- Current: Immediate cystectomy for high risk T1, with the remaining receiving BCG
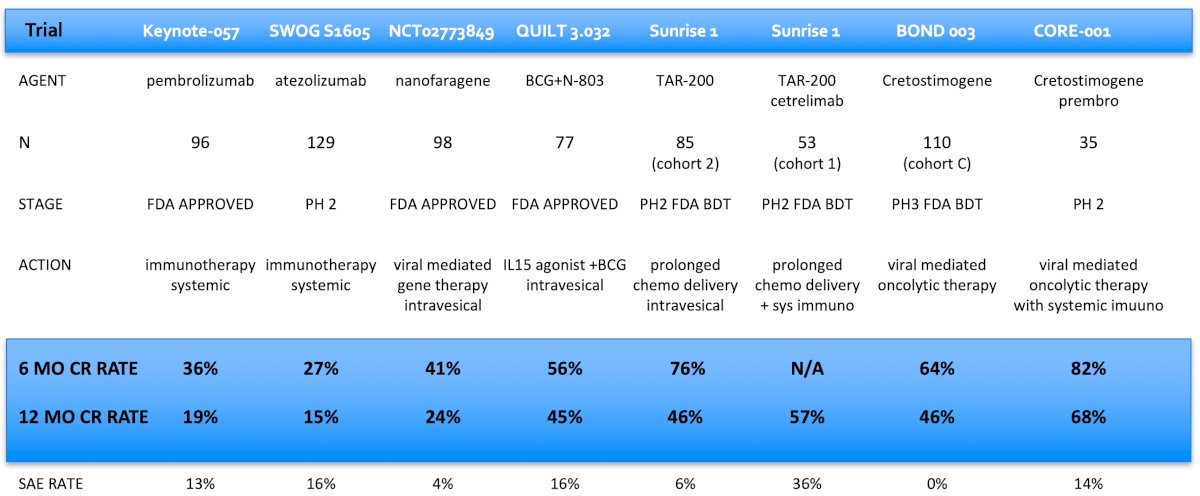
Dr. Bochner emphasized that cross trial comparisons are inappropriate, but we do them anyway. The following table highlights the efficacy and safety outcomes for new treatments for BCG unresponsive non muscle invasive bladder cancer with CIS +/- papillary disease:
 Finally, Dr. Bochner discussed gemcitabine + docetaxel, emphasizing that retrospective studies are not equivalent to prospective clinical trials. In 2020, Steinberg et al.2 investigated intravesical gemcitabine/docetaxel as rescue therapy for non muscle invasive disease. Among 276 patients over a median follow-up of 22.9 months, 39% of patients were CIS alone, 26% were Ta high grade, 21% were T1 high grade, and 13% were Ta low grade. Overall, 53% had one BCG induction course, and 46% had 2+ BCG induction courses, and 38% were “BCG unresponsive.” Of note, some responders went on to maintenance therapy (monthly versus the SWOG schedule) for 24 months. One and 2-year recurrence-free survival rates were 60% and 46%, and high grade recurrence-free survival rates were 65% and 52%, respectively:
Finally, Dr. Bochner discussed gemcitabine + docetaxel, emphasizing that retrospective studies are not equivalent to prospective clinical trials. In 2020, Steinberg et al.2 investigated intravesical gemcitabine/docetaxel as rescue therapy for non muscle invasive disease. Among 276 patients over a median follow-up of 22.9 months, 39% of patients were CIS alone, 26% were Ta high grade, 21% were T1 high grade, and 13% were Ta low grade. Overall, 53% had one BCG induction course, and 46% had 2+ BCG induction courses, and 38% were “BCG unresponsive.” Of note, some responders went on to maintenance therapy (monthly versus the SWOG schedule) for 24 months. One and 2-year recurrence-free survival rates were 60% and 46%, and high grade recurrence-free survival rates were 65% and 52%, respectively:
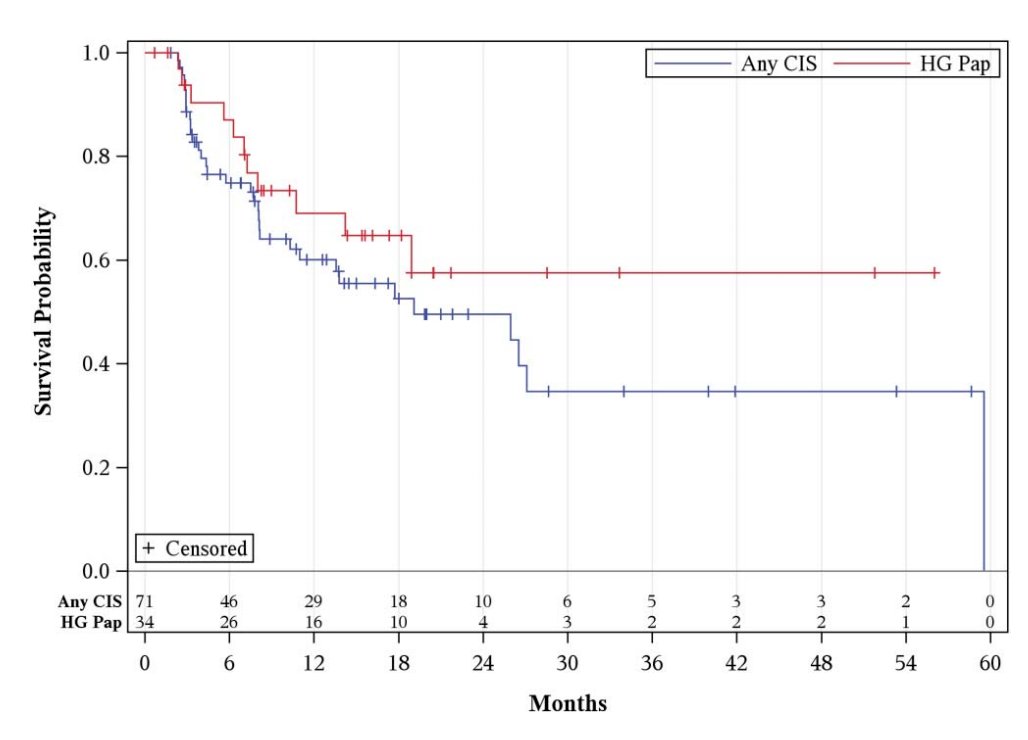
Ten patients (3.6%) had disease progression on transurethral resection, and 43 patients (15.6%) went on to cystectomy (median 11.3 months from induction), of whom 11 (4.0%) had progression to muscle invasion.
Dr. Bochner concluded his presentation discussing clinical trial design in non muscle invasive bladder cancer with the following take home points:
- We need better treatments:
- Single arm, non-randomized trials should go back to being “signal finding” studies
- It is ok to stick with “unresponsive” criteria
- There are an endless number of new treatments and potential combinations that need to be tested – can biomarkers (ie. urinary tumor DNA) serve as surrogate endpoints for quicker readouts?
- More stage specific clinical trials are needed: HGT1 + CIS is not equivalent to HGTa/CIS
- Single arm, non-randomized trials should go back to being “signal finding” studies
- Which current treatment is best?
- There is an urgent need for randomized clinical trials to evaluate approved treatments (and gemcitabine + docetaxel)
- Using a broader BCG failure definition than “unresponsive” improves accrual and generalizability of the data
- There is an opportunity for biomarker integration
- How to conduct these randomized clinical trials is the bigger question
- What is the incentive for pharmaceutical companies?
- Do the cooperative groups have the agility and nimbleness for such trials?
- There is an urgent need for randomized clinical trials to evaluate approved treatments (and gemcitabine + docetaxel)
Presented by: Bernard H Bochner, MD, FACS, Urologic Surgeon, Sir Murray Brennan Endowed Chair, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Interdisciplinary Genitourinary Cancer Forum, St. Petersburg, FL, Thurs, Jun 19 – Sat, Jun 21, 2025.
References:
- Myers AA, Tan WS, Grajales V, et al. Challenging the paradigm of “BCG-unresponsive” Bladder Cancer: Does Additional Bacillus Calmette-Guerin have an effect? Eur Urol. 2024 Oct;86(4):366-368.
- Steinberg RL, Thomas LJ, Brooks N, et al. Multi-Institution Evaluation of Sequential Gemcitabine and Docetaxel as Rescue Therapy for Nonmuscle Invasive Bladder Cancer. J Urol. 2020 May;203(5):902-909.