(UroToday.com) The Interdisciplinary Genitourinary Cancer Forum 2025, held in St. Petersburg, Florida, United States, was host to the Prostate Cancer Session 2: Local Treatments. Dr. Peter Carroll delved into Combination Therapies in the local treatment setting.
Dr. Carroll began his presentation by highlighting that prostate cancer represents a broad spectrum of disease. He emphasized that recent advancements in imaging, molecular and AI profiling, along with findings from landmark clinical trials, have redefined the landscape of prostate cancer management. He noted that treatment decisions are increasingly nuanced, taking into account tumor characteristics, patient age and health, and individual preferences. Ultimately, he underscored that patients and their families are most empowered to make confident decisions when provided with the most accurate and comprehensive information.
Combination or Sequential Therapy: The Case for Active SurveillanceGuidelines from the AUA, EAU, and NCCN1,2 consistently recommend active surveillance (AS) as the preferred management approach for low-risk prostate cancer (PCa). Although Gleason Grade Group 1 (GG1) disease is categorized as low-risk, it still carries the potential to progress to clinically significant cancer, prompting ongoing debate about whether GG1 should even be labeled as “cancer.”
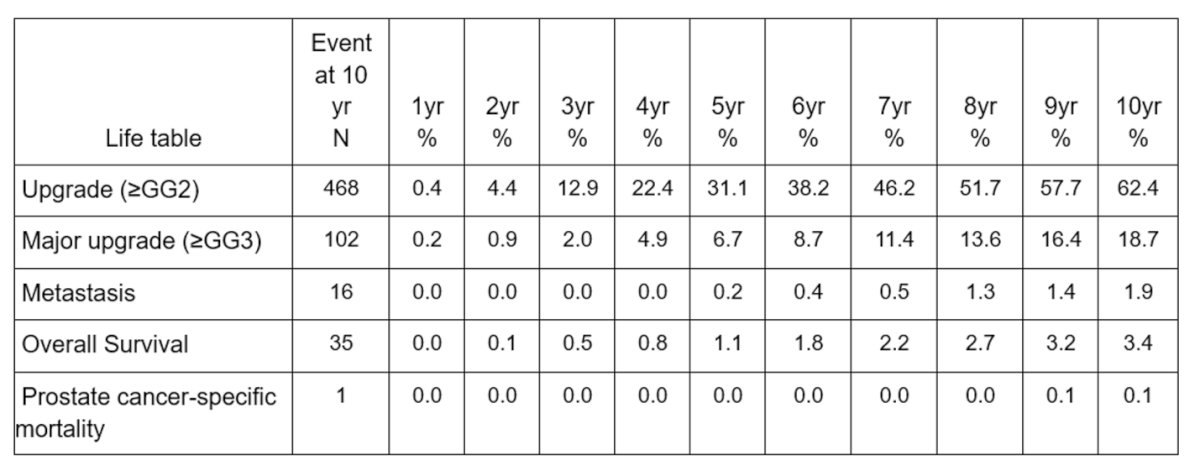
To explore the natural history of GG1 prostate cancer in the contemporary era of MRI and genomic testing, investigators from UCSF conducted an analysis using the Urologic Outcomes Database (UODB). They identified men with confirmed GG1 disease who had undergone at least two biopsies while on active surveillance. The study focused on key outcomes, including any pathologic upgrade (≥GG2), major upgrade (≥GG3), metastasis, overall mortality, prostate cancer–specific mortality, and transition to active treatment following an upgrade.
Among 1,429 men with confirmed GG1 prostate cancer on AS, the median follow-up was approximately 9 years. Over this period, 62.4% experienced any pathologic upgrade (≥GG2) and 18.7% had a major upgrade (≥GG3). However, long-term oncologic outcomes remained favorable: metastasis occurred in only 1.9% of patients, overall survival at 10 years was 96.6%, and prostate cancer–specific mortality was just 0.1%. These findings underscore that while grade progression is common, the risk of lethal disease among men with GG1 managed with modern surveillance protocols remains exceptionally low, as illustrated below.
Moreover, multivariable analysis identified older age, higher PSA density, and greater percentage of positive biopsy cores as independent predictors of upgrade (≥GG2) among men with GG1 prostate cancer on AS. However, initial positive mpMRI, changes in mpMRI, and high-risk genomic scores were not significantly associated with upgrading or adverse outcomes. Notably, upgrade to ≥GG3 was the only variable linked to transition to active treatment. These results support the safety of AS and highlight that currently used genomic and imaging biomarkers may have limited utility in predicting meaningful progression in this population.

The Nature of Progression on Active Surveillance for Gleason Grade Group 2 Prostate Cancer
In a UCSF study using the Urologic Outcomes Database (UODB), researchers examined progression patterns in men with Grade Group 2 (GG2) prostate cancer managed with AS. While GG2 is categorized as favorable intermediate-risk, the study aimed to identify factors associated with progression to higher-risk disease (≥GG3) in the modern era of mpMRI-targeted biopsy. The analysis focused on core positivity and mpMRI features, with the goal of refining selection criteria and understanding the safety of AS in this subset.
In this cohort of 319 men with GG2 prostate cancer managed with active surveillance, the median follow-up was nearly 6 years. At 10 years, the upgrade rate reached 67%, with 19% of patients experiencing an increase in positive cores to over 50%. Two-thirds ultimately transitioned to active treatment. Despite this, the risk of metastasis remained low (3.4%), and no prostate cancer-specific mortality events were recorded, supporting the safety of AS in carefully selected patients with favorable intermediate-risk disease.
In patients with GG2 prostate cancer managed with active surveillance, increased PSA density ≥0.15 and a positive mpMRI (PIRADS 4–5) were independently associated with both disease progression and transition to active treatment. Initial core positivity and PSA density were also linked to increased tumor volume (>50% positive cores). Interestingly, genomic testing did not show a significant association with progression or treatment, highlighting the potential value of imaging and PSA kinetics over molecular profiling in risk stratification for this group.

Dr. Carroll noted the evolving trends at UCSF in the use of radical prostatectomy (RP) and AS, highlighting a shift in diagnostic Gleason grade distributions over time. For RP patients, there has been a marked decrease in GG1 cases and an increase in higher-grade disease (GG3–GG5), reflecting improved risk stratification and patient selection. In contrast, AS has seen a growing proportion of patients with GG2 and even GG3, suggesting expanding criteria and greater confidence in monitoring selected intermediate-risk cases conservatively.

Dr. Carroll questioned the conventional boundaries of what constitutes “clinically significant” prostate cancer, particularly in the context of intermediate-risk disease. While combination therapy is no longer considered relevant for very low and low-risk patients, the classification of GG2 as the threshold for clinical significance remains debated. He emphasized that this binary distinction may be overly simplistic, noting that even among GG3 cases, a notable proportion are downgraded at radical prostatectomy (16%) and over a third have low CAPRA-S scores, suggesting lower biologic risk.

Dr Carroll highlighted a study proposing a refined definition of adverse pathology in prostate cancer, aimed at improving the prediction of metastatic risk regardless of grade group or pathological stage. The authors developed a simplified histological grading system centered on large cribriform and intraductal carcinoma, optimizing sensitivity for metastatic potential.3
Adverse histology is defined as the presence of:
- Any Gleason pattern 5 component
- Any large cribriform morphology (>0.25 mm) or intraductal carcinoma
- Complex intraluminal papillary architecture
- Grade 3 stromogenic carcinoma
- Complex anastomosing cord-like growth
Notably, The Kaplan-Meier plots demonstrate that this histology-based definition (favorable vs unfavorable) stratifies patients by risk of biochemical recurrence, distant metastasis, and prostate cancer–specific mortality as shown below.

Dr. Carroll discussed whether androgen deprivation therapy (ADT) should be used universally in patients with high- or very high-risk prostate cancer treated with radiotherapy. He highlighted a study led by Dr. Spratt that used digital pathology and clinical data from 5,727 patients enrolled in five phase III randomized trials. These trials compared radiotherapy alone versus radiotherapy plus ADT.
This study showed that among predictive model–positive patients, ADT significantly reduced the risk of distant metastasis (sHR 0.34; 95% CI 0.19–0.63; p < 0.001). In contrast, predictive model–negative patients did not benefit significantly from ADT (sHR 0.92; 95% CI 0.59–1.43; p = 0.71). This suggests the model may help individualize decisions on ADT use in conjunction with radiotherapy.

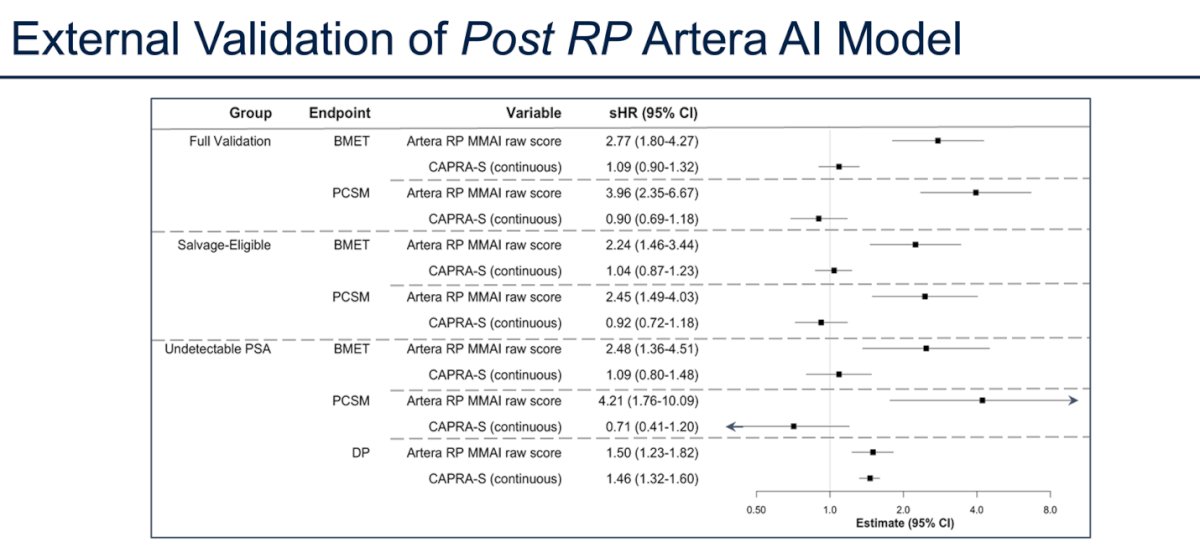
In a UCSF study, researchers evaluated the utility of the Metastatic Modeling with Artificial Intelligence (MMAI) score in predicting oncologic outcomes for patients who had undergone radical prostatectomy (RP). MMAI score was assessed for its ability to predict any metastasis (primary endpoint), bone metastasis, and disease progression (defined as two consecutive PSA values ≥0.2 ng/mL or receipt of salvage therapy). Subgroup analyses included patients with undetectable PSA (first post-RP PSA <0.05 ng/mL ≥6 months after RP) and those eligible for salvage therapy (detectable PSA ≥0.05 ng/mL and/or salvage treatment, with MMAI calculated using pre-salvage PSA). In the validation cohort, after adjusting for CAPRA-S, post-RP MMAI remained independently associated with adverse outcomes following surgery across clinical subgroups as shown below.
Historically, among patients experiencing biochemical persistence after radical prostatectomy, prostate cancer-specific mortality (PCSM) is around 1% and all-cause mortality 4.7% at a median follow-up of 4.2 years. Notably, 26% of these patients received no further treatment, and PSA velocity (PSAV) was associated with systemic relapse. In contrast, among patients with biochemical recurrence, metastasis-free survival (MFS) was 92%, PCSM was 3%, and ACM was 6% at 10 years, with 56% receiving no salvage treatment. High CAPRA-S scores and PSA doubling time (PSA-DT) <6 months were associated with the likelihood of undergoing salvage therapy.
Dr Caroll noted that improved PSA recurrence-free survival in high-risk CAPRA-S patients was associated with the use of adjuvant EBRT compared to early or late salvage EBRT. However, there was no observed benefit of salvage EBRT at varying PSA thresholds (<0.15, 0.15–<0.2, 0.2–<0.3, ≥0.3 ng/mL) in improving 5-year treatment-free survival based on multivariable Cox proportional hazard modeling as illustrated below.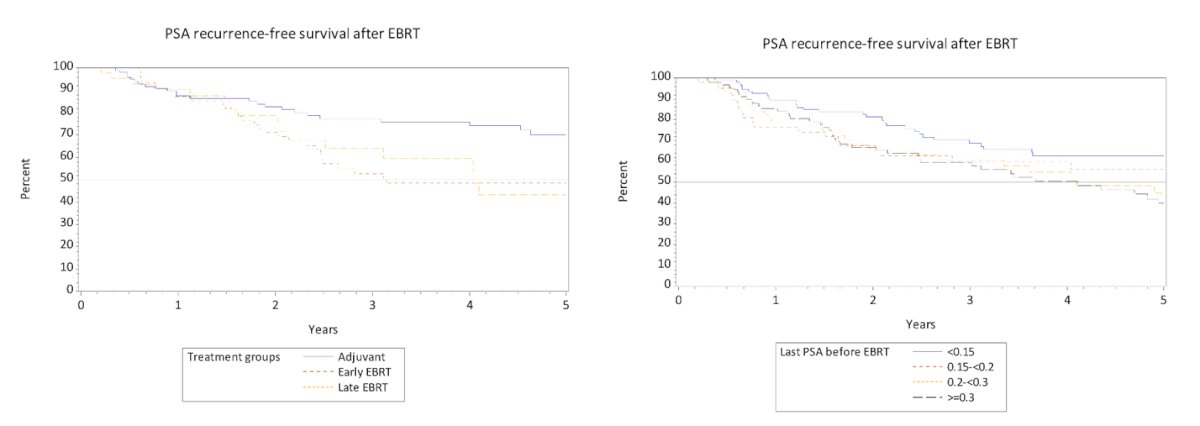
The cumulative incidence of bone metastasis or PCSM over time remains low across all treatment groups, including patients who received no additional therapy, RT + ADT, ADT alone, or interventions, suggesting that a delayed detectable PSA may not necessarily portend poor outcomes, particularly in the absence of other high-risk features.

Notably, the cumulative incidence of urinary adverse events was highest in patients treated with combination therapy, particularly RP + EBRT, followed by BT + EBRT. In contrast, monotherapy approaches such as EBRT alone, RP alone, and brachytherapy had lower cumulative risks, with focal ablaiton showing the lowest incidence over time.

Moreover, Dr. Carroll highlighted the potential of better imaging to enhance surgical outcomes in prostate cancer, referencing a phase 1 study of IS-002, a PSMA-targeting fluorophore. This trial focused on high-risk patients (CAPRA ≥ 6) undergoing robotic prostatectomy, with the primary objective of assessing the safety and tolerability of intravenous IS-002. Secondary objectives included evaluating pharmacokinetics, while exploratory endpoints aimed to assess the agent's efficacy in detecting prostate cancer intraoperatively

The phase 1 study of IS-002 demonstrated promising intraoperative utility, with a strong fluorescent signal observed from the primary tumor and residual disease not visible under standard white light endoscopy. Fluorescent-guided biopsies confirmed adenocarcinoma, and IS-002 successfully highlighted lymph nodes with tumor involvement, later confirmed by frozen section. Residual local and regional disease was identified in 33% and 9% of patients, respectively, underscoring the potential of IS-002 to enhance real-time detection of prostate cancer during surgery.
Pathology analyses confirmed that IS-002 selectively targets prostate cancer tissue, with fluorescence imaging integrated into standard histopathology workflows. The observed fluorescence signal corresponded closely with cancerous regions identified on H&E staining by the study pathologist, supporting the specificity of IS-002 for prostate tumor visualization at the microscopic level.

Dr. Carroll highlighted that IS-002 was safe and well tolerated, with the most common adverse event being Grade 1 urine discoloration (observed in 22 of 24 patients), and no Grade 2 or higher events reported. At the 25 µg/kg dose, IS-002 demonstrated promising exploratory efficacy, with negative and positive predictive values of 97% and 45% for lymph node detection, and 100% and 80% for residual or loco-regional disease, respectively. These findings suggest IS-002 could enable real-time intraoperative tumor identification beyond what is possible with standard imaging.5
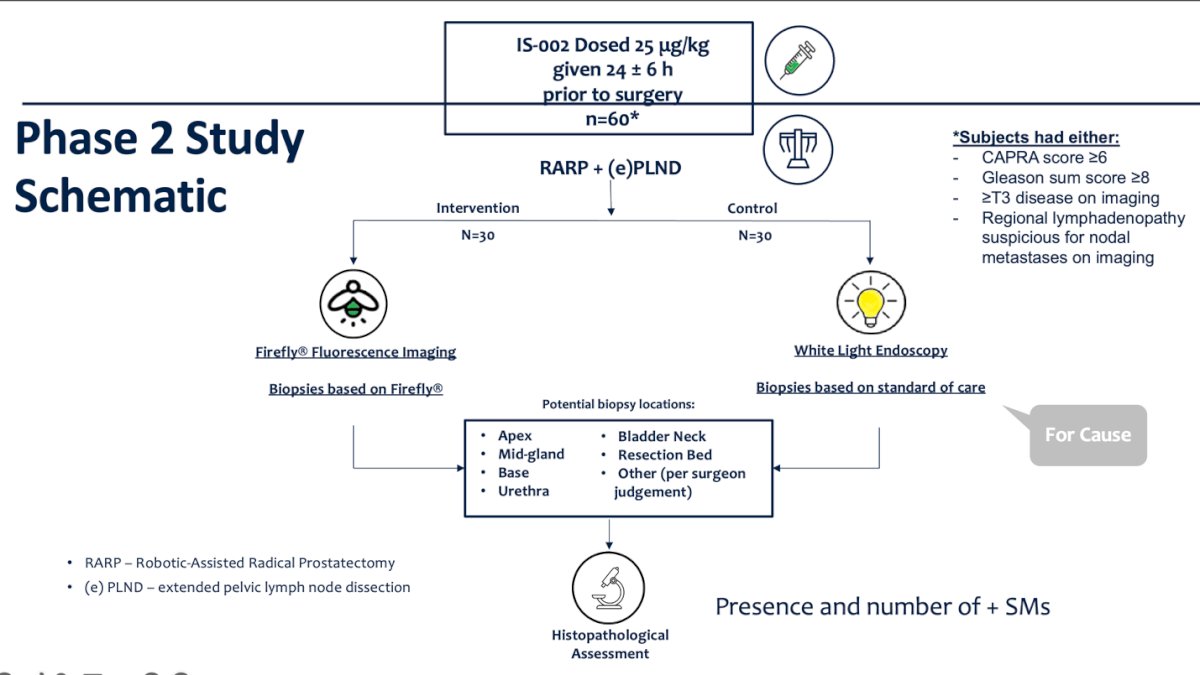
Dr. Carroll presented the Phase 2 study design for IS-002, which will enroll patients aged 18 to 75 with histologically confirmed prostate adenocarcinoma. Eligible patients must meet at least one high-risk criterion, including CAPRA score ≥6, Gleason score ≥8, ≥T3 disease on imaging, or regional lymphadenopathy suspicious for nodal metastasis. The protocol also incorporates histopathological reconciliation to potentially downgrade positive margins, refining post-operative assessment and treatment decisions.
Dr Carroll concluded his presentation with the following final thoughts:
- Prostate cancer is a spectrum of disease, and its management is similarly a spectrum
- Advances in imaging, molecular diagnostics, germline testing, and AI have refined treatment strategies
- Some historic combination approaches have been refined to monotherapy
- Those that benefit most from combination therapy have been better defined
Presented by: Peter R. Carroll, MD, MPH, Department of Urology, University of California, San Francisco, San Francisco, CA.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the Interdisciplinary Genitourinary Cancer Forum 2025, between June 19 – 22, 2025 in St. Petersburg, Florida, United States
Reference:
- Mohler JL, Antonarakis ES, Armstrong AJ, D’Amico AV, Davis BJ, Dorff T, et al. Prostate cancer, version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2019;17(5):479–505.
- Cornford P, Bellmunt J, Bolla M, Briers E, De Santis M, Gross T, et al. EAU–EANM–ESTRO–ESUR–SIOG Guidelines on prostate cancer. Eur Urol. 2017;71(4):618–29.
- Nguyen JK, Harik LR, Klein EA, Li J, Corrigan D, Liu S, Chan E, Hawley S, Auman H, Newcomb LF, Carroll PR, Cooperberg MR, Filson CP, Simko JP, Nelson PS, Tretiakova MS, Troyer D, True LD, Vakar-Lopez F, Weight CJ, Lin DW, Brooks JD, McKenney JK. Proposal for an optimised definition of adverse pathology (unfavourable histology) that predicts metastatic risk in prostatic adenocarcinoma independent of grade group and pathological stage. Histopathology. 2024 Oct;85(4):598-613. doi: 10.1111/his.15231. Epub 2024 Jun 3. PMID: 38828674; PMCID: PMC11365761.
- Spratt DE, Tang S, Sun Y, Huang HC, Chen E, Mohamad O, Armstrong AJ, Tward JD, Nguyen PL, Lang JM, Zhang J, Mitani A, Simko JP, DeVries S, van der Wal D, Pinckaers H, Monson JM, Campbell HA, Wallace J, Ferguson MJ, Bahary JP, Schaeffer EM; NRG Prostate Cancer AI Consortium; Sandler HM, Tran PT, Rodgers JP, Esteva A, Yamashita R, Feng FY. Artificial Intelligence Predictive Model for Hormone Therapy Use in Prostate Cancer. Res Sq [Preprint]. 2023 Apr 21:rs.3.rs-2790858. doi: 10.21203/rs.3.rs-2790858/v1. Update in: NEJM Evid. 2023 Aug;2(8):EVIDoa2300023. doi: 10.1056/EVIDoa2300023. PMID: 37131691; PMCID: PMC10153374.
- Nguyen HG, van den Berg NS, Antaris AL, Xue L, Greenberg S, Rosenthal JW, Muchnik A, Klaassen A, Simko JP, Dutta S, Sorger JM, Munster P, Carroll PR.Eur Urol Oncol. 2024 Feb;7(1):63-72. doi: 10.1016/j.euo.2023.07.004. Epub 2023 Jul 27.