(UroToday.com) The Interdisciplinary Genitourinary Cancer Forum 2025, held in St. Petersburg, Florida, United States, was host to the Prostate Cancer Session 4: Molecular Targeted Imaging and Theranostics. Dr. David Albala discussed the role of Artificial Intelligence in Molecular Targeted Imaging and Theranostics.
Dr. Albala began by discussing the historical milestones that shaped the field of artificial intelligence, starting with Alan Turing's foundational work in the 1940s and the Dartmouth Workshop in the 1950s. He highlighted key developments such as the creation of the first chatbot and mobile robot in the 1960s–70s, the early cycles of enthusiasm and disillusionment in AI research, and the resurgence of interest in the 1990s. Major breakthroughs included IBM’s Deep Blue defeating a chess champion in 1996, the deployment of AI-equipped NASA rovers in 2004, and Watson’s Jeopardy win in 2011. He concluded by noting the evolution toward modern AI assistants like Siri and Alexa and the release of ChatGPT by OpenAI in 2022.
The applications of AI in nuclear medicine are rapidly evolving. Early efforts centered on improving diagnostic accuracy and outcome prediction using machine learning. With advances in deep learning, particularly convolutional and transformer-based networks, AI now enables more accurate image segmentation, low-dose imaging, and patient-specific dosimetry. Generative AI, powered by large language models and diffusion techniques, is beginning to support complex interpretation and synthesis of medical data. However, limitations such as data scarcity, heterogeneity, and ethical issues persist. Moving forward, interdisciplinary collaboration will be essential to foster adoption, enhance care, and optimize treatment outcomes.
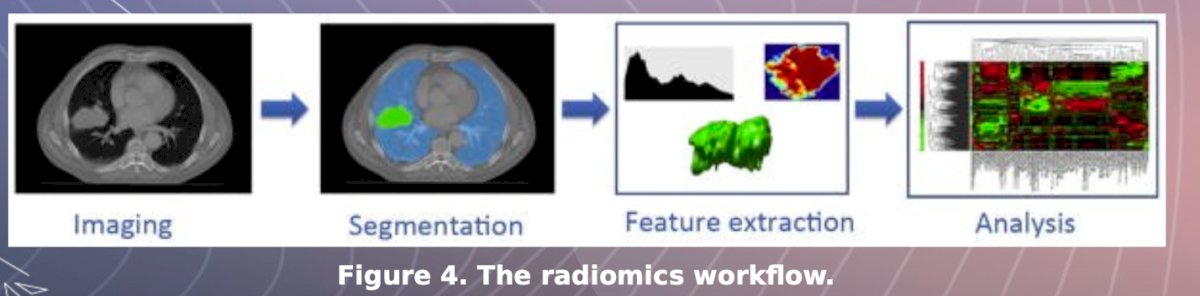
AI has played a transformative role in medical imaging, driven by the exponential growth of imaging data since the early 2000s and advances in computational power. A key milestone was the introduction of radiomics in 2012, which refers to the high-throughput extraction of quantitative features from medical images. This process, encompassing imaging, segmentation, feature extraction, and analysis, enables deeper insights into tumor characterization and supports more personalized, data-driven decision-making in oncology and other specialties as illustrated below.
The current role of AI in medical imaging is multifaceted, and can be divided in four key contributions:
- Efficiency: AI tools streamline workflows, enabling faster image interpretation and improving overall patient care.
- Efficacy: By supporting accurate image analysis, AI can help reduce diagnostic errors and enhance clinical decision-making.
- Assistance: As imaging volumes rise, AI helps bridge the gap caused by a shortage of radiologists by handling routine tasks and prioritizing critical cases.
- Productivity: Automation and intelligent triaging mitigate radiologist workload, reducing burnout and enabling focus on complex diagnoses.
AI algorithms are models developed to perform tasks that typically require human intelligence, such as data analysis, pattern recognition, image interpretation, or language processing. In medicine, physicians similarly rely on data from symptoms, clinical guidelines, and studies to diagnose and treat patients. Through training and experience, they learn which patterns of clinical features are associated with specific conditions. As new information becomes available (e.g., lab tests or imaging), they refine their hypotheses and arrive at more precise diagnoses. AI mirrors this process by using data and pattern recognition to inform decision-making.
Machine LearningMachine learning is a branch of AI in which models learn patterns from data and use these patterns to make predictions, without needing explicit programming. While powerful, machine learning still relies on human input to define and extract relevant features from raw data. In nuclear medicine, early applications focused on improving diagnostic accuracy by using machine learning algorithms for disease classification and outcome prediction for example, clustering patient data based on feature similarities.
Deep Learning Systems (DLS)Deep learning is a subset of machine learning that utilizes deep neural networks to handle more complex tasks with minimal human input. Unlike traditional models, deep learning systems can process raw inputs such as image pixels or text directly. Their effectiveness depends heavily on data availability, allowing them to learn patterns directly from large datasets. Recent advances especially in convolutional and transformer-based networks have significantly improved diagnostic precision, image segmentation, and personalized dosimetry in nuclear medicine.
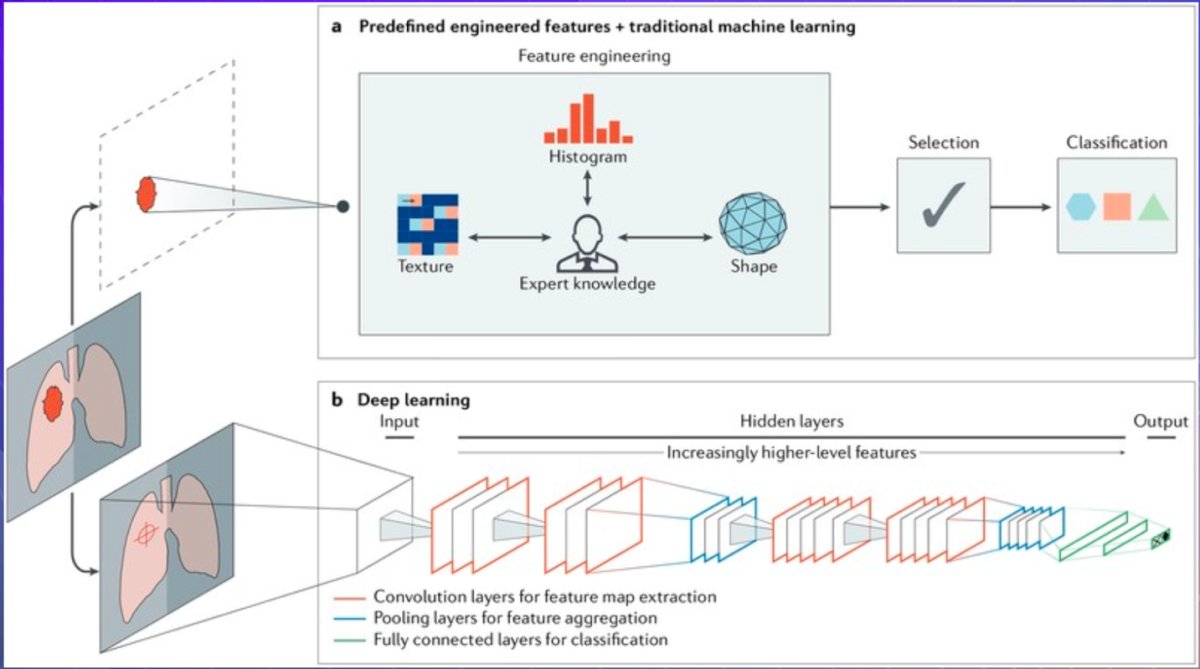
AI methods in medical imaging can be broadly categorized into machine learning and deep learning approaches. The figure below highlights key differences between the two, including how features are extracted and interpreted

Traditional machine learning in medical imaging relies on predefined features such as texture, shape, and intensity, typically selected based on expert knowledge and processed through a classifier. In contrast, deep learning automates this process by simultaneously extracting, selecting, and classifying features through layered neural networks. This data-driven approach enables more efficient and scalable analysis, with the potential to improve accuracy in distinguishing malignant from benign tissue as illustrated below.1
In a comparison of classification performance using breast and lung imaging datasets, deep learning systems (DLS), specifically the stacked denoising autoencoder (SDAE), outperformed traditional engineered feature platforms such as RANK, CURVE, and MORPH. This superiority was consistent across both accuracy (ACC) and area under the curve (AUC) metrics, supporting the growing evidence that DLS approaches offer greater diagnostic reliability in medical imaging applications.2
Moreover, radiomics and DLS represent powerful AI tools in oncology and disease modeling. By extracting and analyzing quantitative imaging features, these methods enable phenotypic decoding of tumors, allowing for prediction of survival time and treatment outcomes even before therapy is initiated.
AI in nuclear medicine is driving advances across multiple domains. For diagnostic purposes, classification models are commonly used to interpret imaging features and accurately identify diseases or their stages. Prognostic models are being applied to predict patient outcomes and treatment responses. AI also plays a key role in enhancing image quality through techniques such as reconstruction, attenuation correction, and denoising, ultimately improving diagnostic accuracy while minimizing radiation exposure. In theranostics, AI supports more precise dosimetry and individualized treatment planning, particularly with radioligands like Lutetium-177 PSMA.
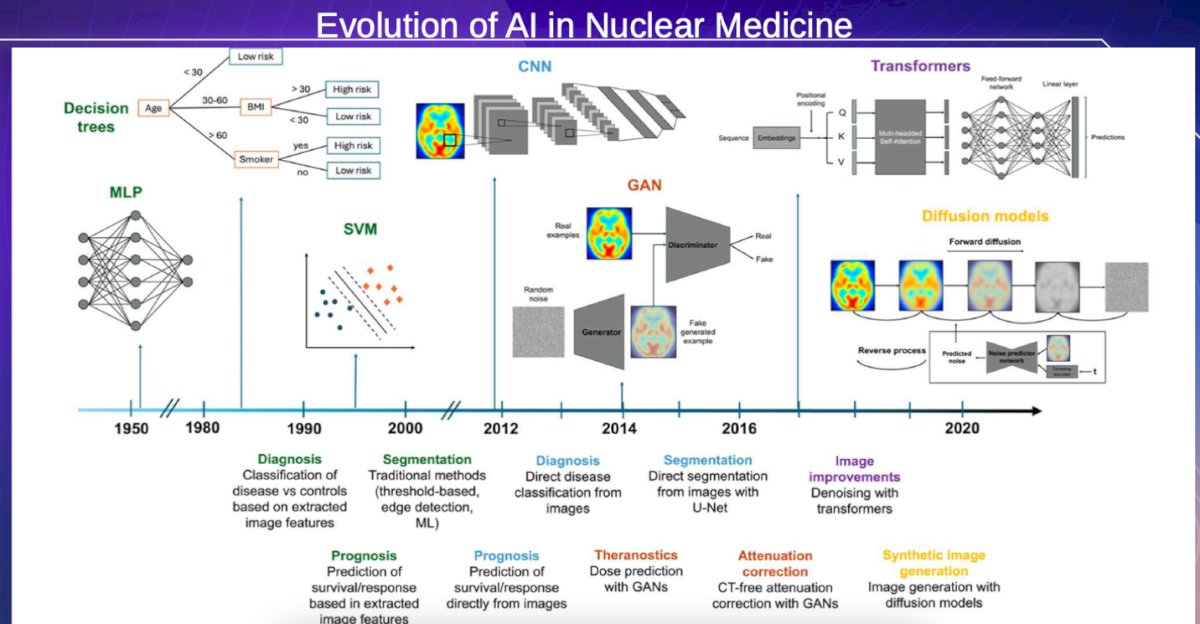
Dr Albala highlighted the progression of AI applications in nuclear medicine, tracing the shift from early rule-based decision trees and basic neural networks (MLP) to more complex architectures such as CNNs, GANs, and transformers. Initially focused on disease classification using extracted image features, AI models evolved to handle segmentation, prognosis prediction, and direct image interpretation. Over the past decade, innovations like GANs have enabled dose prediction and CT-free attenuation correction, while recent advances in transformers and diffusion models have improved image denoising and facilitated synthetic image generation, paving the way for more precise, efficient, and personalized nuclear medicine. The evolution of AI in nuclear medicine is shown below.
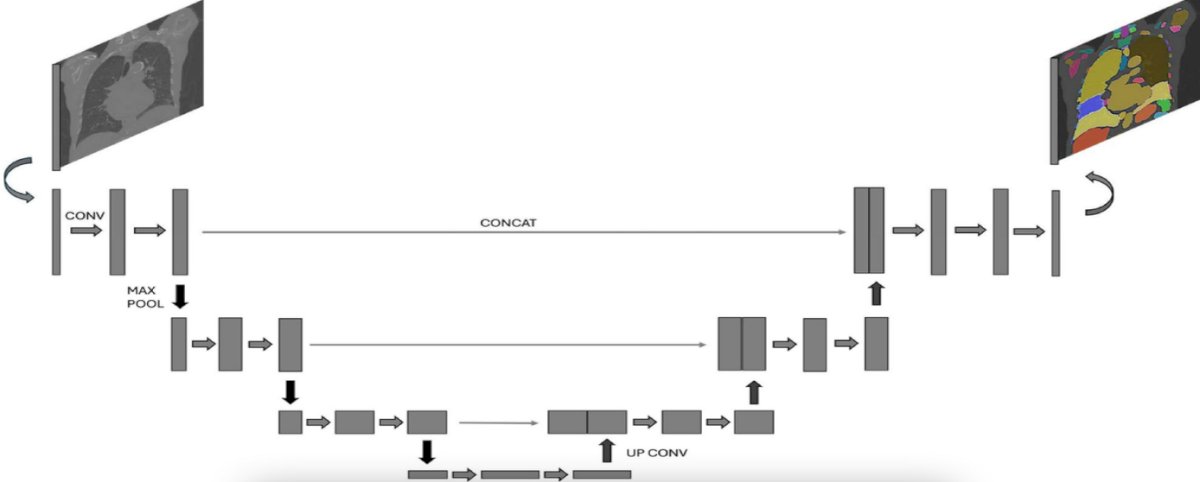
U-Net is a widely used deep learning architecture for medical image segmentation. It follows a symmetric encoder-decoder structure where the input image is first compressed through convolution and max-pooling layers to extract contextual features, then expanded via up-convolution to recover spatial resolution. Skip connections directly link the encoder and decoder layers at corresponding levels, allowing detailed localization information to be preserved. This architecture is particularly effective for pixel-wise segmentation tasks such as identifying organs or tumors in CT or MRI scans.3
Furthermore, Dr Albala noted that AI-based tools are increasingly being applied for diagnostic and prognostic tasks in nuclear medicine. Machine learning models have been used to assess cancer response on PET/CT, predict outcomes from myocardial perfusion SPECT, and identify progression from cognitive impairment to Alzheimer’s disease using FDG-PET. PET imaging with radiolabeled probes, including those targeting PSMA, provides precise phenotyping that supports treatment decision-making. Additionally, ML has enabled radiomic-based subtype classification, tumor grading, and survival prediction. Deep learning models, which eliminate the need for manual feature extraction, have shown robust performance in classifying imaging data across cancer types and clinical applications.
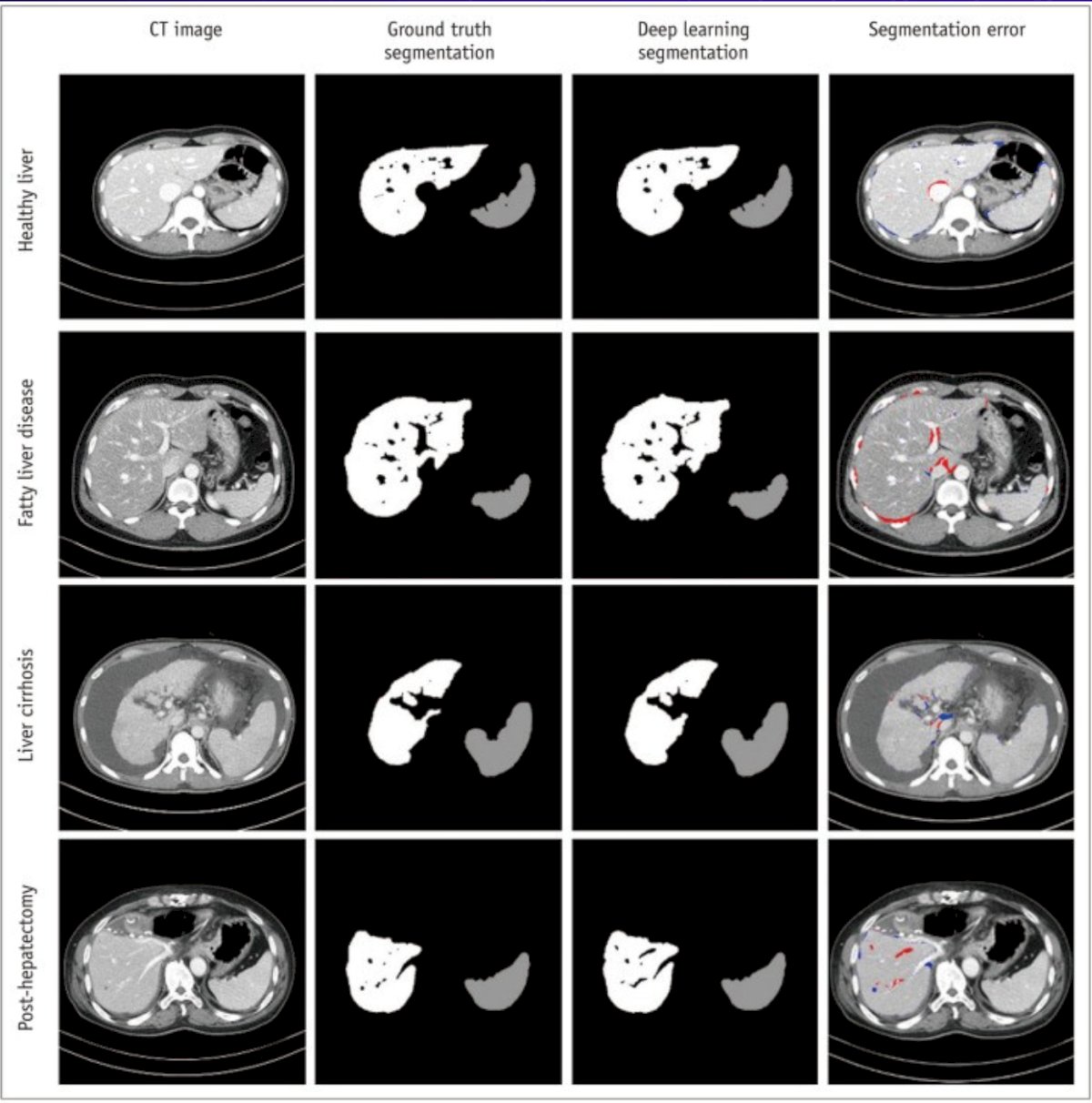
Dr Albala highlighted a study in which a deep learning system was evaluated for automated liver and spleen segmentation on CT in patients with various liver pathologies. In a cohort of 150 patients, the model achieved high Dice similarity scores (DSS) of 0.973 for liver and 0.974 for spleen, indicating excellent segmentation performance. The DLS showed no significant bias in liver volume or liver-to-spleen volume ratio. However, it tended to underestimate spleen volume, with a statistically significant difference (p < 0.001).4
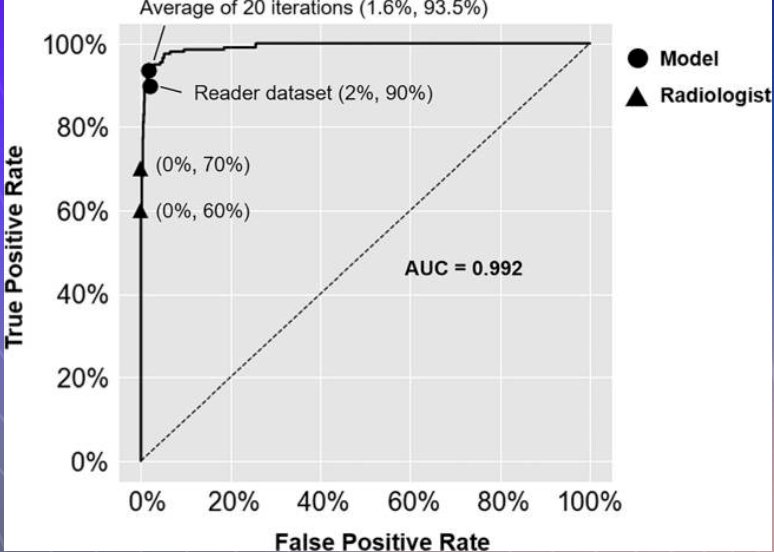
Similarly, a convolutional neural network-based deep learning system demonstrated strong performance in classifying hepatic lesions on multi-phasic MRI, particularly for hepatocellular carcinoma (HCC). In a study analyzing 494 hepatic lesions, the DLS achieved 90% sensitivity for HCC classification outperforming radiologists who achieved 60–70% sensitivity. The model maintained a high true positive rate of 93.5% and a low false positive rate of 1.6%, with an AUC of 0.992 and a computation time per lesion of just 5.6 milliseconds.5
AI integration in PET imaging enhances multiple aspects of the workflow, from acquisition to interpretation. It facilitates improved image quality, tumor delineation, registration, and quantitative analysis. Additionally, AI supports dose optimization, automated abnormality detection, and longitudinal image comparison to monitor therapeutic response. It can also generate interpretive reports and integrate imaging findings with clinical data for more comprehensive patient evaluation.
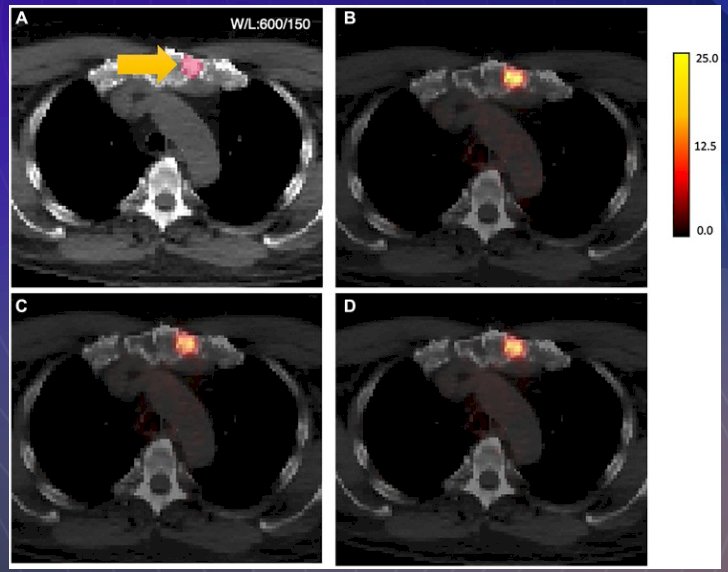
More specifically, in PSMA PET imaging, in a study of 302 prostate cancer patients undergoing 18F-DCFPyL PSMA PET-CT, AI-driven deep learning systems were able to generate attenuation-corrected PET (AC-PET) images from non-attenuation-corrected (NAC) data. The AI-generated images showed strong concordance with standard AC-PET, with ICC values for SUV_max and SUV_mean of 0.88 and 0.89, respectively. Performance metrics in the test cohort included a NMSE of 13.26%, MAE of 3.59%, SSIM of 0.891, and PSNR of 26.82, supporting the feasibility of AI-based reconstruction without the need for attenuation correction CT.6
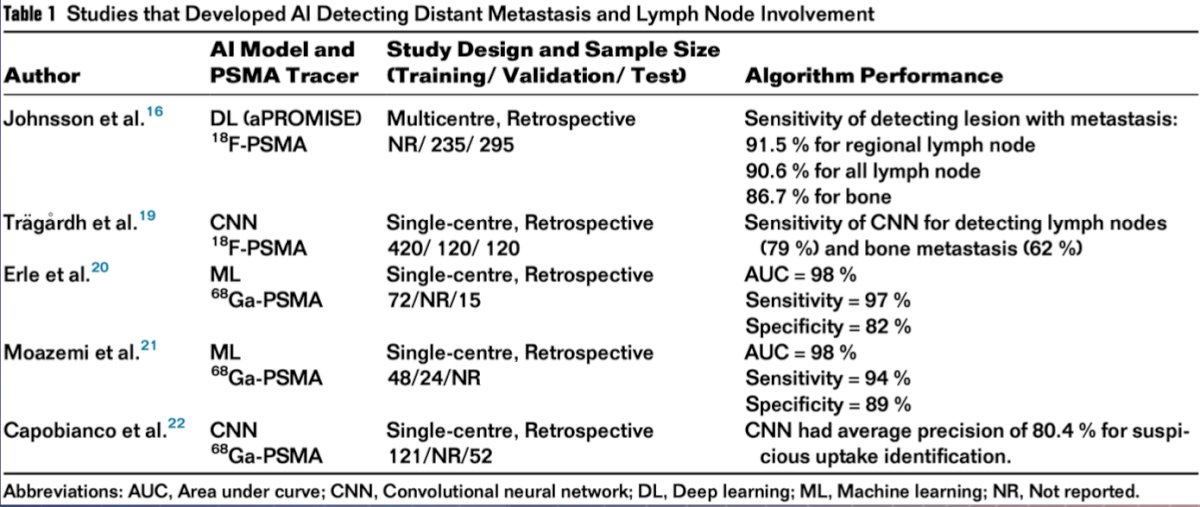
Furthermore, the FDA-approved aPROMISE platform enables automated and standardized evaluation of PSMA PET scans by integrating CT-based anatomical data with tracer uptake information. This AI tool demonstrated high sensitivity for detecting bone metastases (86.7%) and lymph node involvement (90.6%). Assessing metastatic burden using tools like aPROMISE can help inform decisions regarding radiotherapy and potentially guide future metastasis-directed interventions. Other independent AI models, including CNN-based algorithms, are also being developed to improve detection accuracy in the metastatic prostate cancer setting.
Dr Albala summarized in the table below the studies that developed AI detecting distant metastasis and lymph node involvement. Notably, the sensitivity across all studies is above 90%.
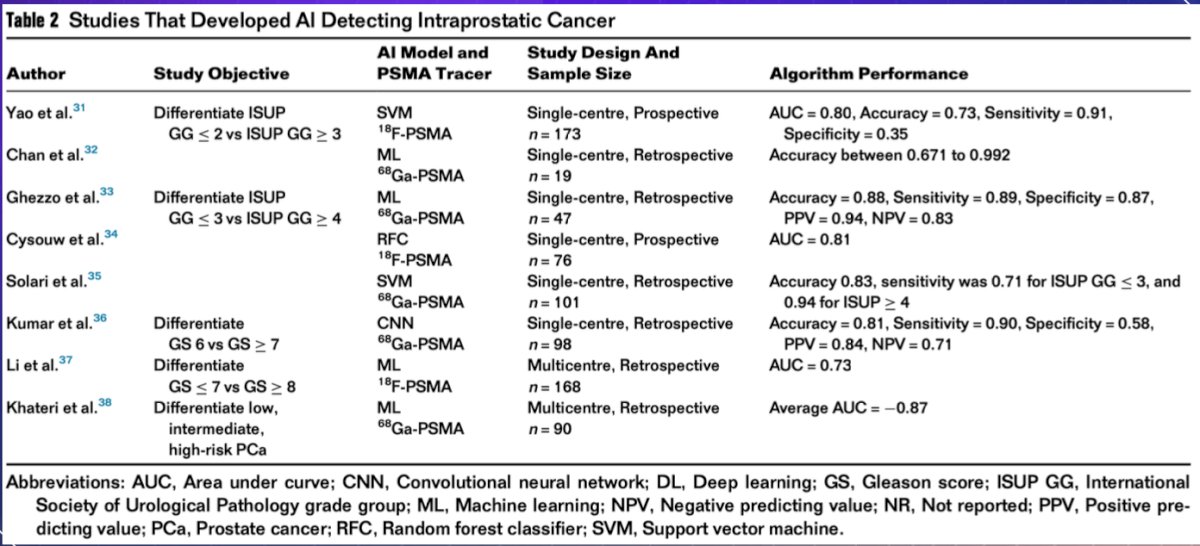
Moreover, several AI models using PSMA PET imaging have been developed to noninvasively characterize intraprostatic tumors. The table below highlights key studies differentiating ISUP grade groups, Gleason scores, and risk stratification using machine learning and deep learning techniques.
Dr. Albala acknowledged key limitations to AI’s implementation in PET scanning, highlighting four major domains: manufacturing variability, where differences in scanner parameters across vendors affect consistency; analysis, where variations in acquisition, reconstruction, and segmentation can compromise biomarker reliability; standardization, due to the absence of a unified uptake value to define lesions for AI training; and training, where the need for large annotated datasets hampers AI performance in smaller or less curated data environments.
In addition to technical constraints, Dr. Albala noted broader limitations to AI implementation in medical imaging, including the lack of high-quality, large-scale longitudinal datasets, inconsistent imaging protocols across institutions, and the complexity of clinical scenarios that challenge standardization. He also emphasized the difficulty of harmonizing data from diverse sources and raised important ethical and legal concerns, particularly regarding responsibility when AI-assisted diagnoses are incorrect.
Dr. Albala concluded the presentation by emphasizing the humanistic potential of AI in medicine, echoing Dr. Eric Topol’s view that AI can “make health care human again” by restoring time and focus to the physician–patient relationship. By reducing the administrative burden and data entry fatigue that often detracts from direct patient care, AI can help clinicians reconnect with the core values of their profession.
Presented by: David M. Albala, MD, Chief of Urology Crouse Hospital, Syracuse, NY Associated Medical Professionals of NY, Syracuse, NY.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the Interdisciplinary Genitourinary Cancer Forum 2025, between June 19 – 22, 2025 in St. Petersburg, Florida, United StatesReference:
- Hosny A, Parmar C, Quackenbush J, Schwartz LH, Aerts HJWL. Artificial intelligence in radiology. Nat Rev Cancer. 2018 Aug;18(8):500-510. doi: 10.1038/s41568-018-0016-5. PMID: 29777175; PMCID: PMC6268174.
- Cheng JZ, Ni D, Chou YH, Qin J, Tiu CM, Chang YC, Huang CS, Shen D, Chen CM. Computer-Aided Diagnosis with Deep Learning Architecture: Applications to Breast Lesions in US Images and Pulmonary Nodules in CT Scans. Sci Rep. 2016 Apr 15;6:24454. doi: 10.1038/srep24454. PMID: 27079888; PMCID: PMC4832199.
- Lopes L, Lopez-Montes A, Chen Y, Koller P, Rathod N, Blomgren A, Caobelli F, Rominger A, Shi K, Seifert R. The Evolution of Artificial Intelligence in Nuclear Medicine. Semin Nucl Med. 2025 May;55(3):313-327. doi: 10.1053/j.semnuclmed.2025.01.006. Epub 2025 Feb 10. PMID: 39934005.
- Ahn Y, Yoon JS, Lee SS, Suk HI, Son JH, Sung YS, Lee Y, Kang BK, Kim HS. Deep Learning Algorithm for Automated Segmentation and Volume Measurement of the Liver and Spleen Using Portal Venous Phase Computed Tomography Images. Korean J Radiol. 2020 Aug;21(8):987-997. doi: 10.3348/kjr.2020.0237. PMID: 32677383; PMCID: PMC7369202.
- Hamm CA, Wang CJ, Savic LJ, Ferrante M, Schobert I, Schlachter T, Lin M, Duncan JS, Weinreb JC, Chapiro J, Letzen B. Deep learning for liver tumor diagnosis part I: development of a convolutional neural network classifier for multi-phasic MRI. Eur Radiol. 2019 Jul;29(7):3338-3347. doi: 10.1007/s00330-019-06205-9. Epub 2019 Apr 23. PMID: 31016442; PMCID: PMC7251621.
- Ma KC, Mena E, Lindenberg L, Lay NS, Eclarinal P, Citrin DE, Pinto PA, Wood BJ, Dahut WL, Gulley JL, Madan RA, Choyke PL, Turkbey IB, Harmon SA. Deep learning-based whole-body PSMA PET/CT attenuation correction utilizing Pix-2-Pix GAN. Oncotarget. 2024 May 7;15:288-300. doi: 10.18632/oncotarget.28583. PMID: 38712741; PMCID: PMC11075367.