(UroToday.com) In the Top Abstracts session of the 2021 International Kidney Cancer Symposium (IKCS): North America meeting, Dr. Tannir presented work, based on the CheckMate214 trial, examining long-term survival outcomes for patients treated with first-line nivolumab and ipilimumab compared to sunitinib in patients with metastatic renal cell carcinoma (mRCC).
Dr. Tannir began by reviewing the CheckMate214 trial which forms the basis for the nivolumab and ipilimumab as a first-line standard of care in patients with mRCC based on superior long-term survival compared to sunitinib. This presentation focused on a post hoc, exploratory analysis among patients who survived at least 5 years.
The methodology of the CheckMate-214 trial has been well described in prior presentations and publications. In short, patients with previously untreated clear cell mRCC were randomized 1:1 to receive either nivolumab and ipilimumab or sunitinib. Baseline characteristics among those who survived at least 5 years, as compared to the intention to treat population, demonstrated a higher proportion of IMDC favourable risk disease and a greater proportion of patients with a single target lesion.
Long-term survival was reported in 43% of all patients randomized to nivolumab and ipilimumab and 31% of those randomized to sunitinib. Among those with intermediate/poor-risk disease rates were 38% and 27%, respectively, while among those with favourable risk disease, rates were 58% versus 48%, respectively.
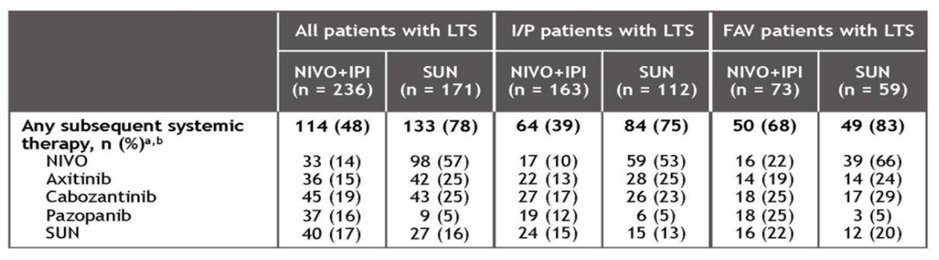
In this cohort, subsequent systemic therapy was administered more commonly among those randomized to sunitinib (78%) than those randomized to nivolumab and ipilimumab (48%).
Even among those with long-term survival, complete response rates were higher among patients who received nivolumab and ipilimumab (24%) compared to sunitinib (9%). This was true both overall, and among subgroups of patients with intermediate/poor-risk disease (25% vs 6%) and favourable risk disease (22% vs 14%). Further, the median time to response was shorter among those who received nivolumab and ipilimumab and the duration of response was longer (median not reached vs 39 months).
Treatment-free intervals were more common (54% vs 14% among patients with intermediate/poor-risk disease and 43% vs 10% among patients with favourable risk disease) and longer for patients receiving nivolumab and ipilimumab.
In terms of safety, among this cohort of patients who survived at least 5 years on trial, any-grade treatment-related adverse events leading to discontinuation were more common among patients receiving nivolumab and ipilimumab (28%) than those receiving sunitinib (16%), a difference which paralleled the overall study population (23% vs 13%).
In summary, this analysis of patients in CheckMate214 who had long-term survival highlighted the greater likelihood of long-term clinical benefit in patients receiving nivolumab and ipilimumab. Notably, baseline demographics and clinical characteristics generally did not distinguish patients who would experience long-term survival from the overall study cohort. Further, failing to achieve a complete response or partial response did not prevent some patients from achieving long-term survival.
Presented by: Nizar M. Tannir, MD, FACP, Department Chair ad interim, Deputy Department Chair, Ransom Horne, Jr. Professorship for Cancer Research, Department of Genitourinary Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, Texas