He began discussing the early days when chemotherapy had just begun to be given to metastatic bladder cancer patients. In a study published in 2000 by Von der Masse, 405 metastatic patients who were not treated previously with chemotherapy were randomized to either methotrexate + vinblastine + doxorubicin + cisplatin (MVAC) protocol or to gemcitabine and cisplatin (GC).1 This study demonstrated comparable overall response rate, a metastasis progression-free survival of 7.7 and 8.3 months for GC and MVAC, respectively, with a hazard ratio of 1.09. Moreover, the overall survival rate was similar as well (14 vs. 15 months) with a 5-year overall survival rate of 13-15% in both arms, p=0.53. However, GC did demonstrate to harbor less grade 3 or 4 complications. This trial resulted in GC being the standard 1st line therapy in cisplatin eligible metastatic bladder cancer patients.
There have been many studies assessing various salvage therapies for metastatic urothelial cancer. However, they have shown a response rate of between 0-44%, with a median overall survival ranging between 3-10.8 months. 2 Due to these overall poor response rates and outcomes, it was decided to try other medical treatments in this setting, such as the immune checkpoint inhibitors, and several trials were initiated.
One of these ongoing trials is a phase 2 study from the Cleveland Clinic, led by Dr. Matthew Galsky (GU14-182). In this trial metastatic urothelial carcinoma patients after the first line, platinum-based chemotherapy were randomized to either intravenous Pembrolizumab 200 mg every three weeks or to placebo. If patients at the placebo arm had progressed, they underwent crossover to the Pembrolizumab arm.
Another similar ongoing trial is the randomized, open-label two-arm study led by Dr. Thomas Powles, randomizing metastatic bladder cancer patients after 1st line chemotherapy (4-6 cycles) to either the immune checkpoint inhibitor Avelumab + best supportive case, or to the arm of best supportive care alone.
The GO29293 (IMvigor 210) single arm phase two study in metastatic urothelial carcinoma was a study presented in ASCO 2016. 3. This study included patients with locally advanced or metastatic urothelial carcinoma who either had 1st line cisplatin-based chemotherapy or had no prior chemotherapy (because they were ineligible for cisplatin-based chemotherapy). All patients received intravenous Atezolizumab 1200 mg every three weeks for a total of 16 cycles (Figure 1). The results demonstrated that 46% of patients had a decrease in target lesions, with a greater reduction in tumor burden seen with a higher PD-L1 status.

Figure 1 – GO29293 (IMvigor 210) study scheme:
Another study (the Checkmate-275) assessed the role of Nivolumab as salvage therapy.4 In the 265 patients accrued for this trial, the overall response rate was 19.6% with complete response rate witnessed in only 2.3% of patients and disease progression was seen in 39.2% of patients. The overall response rate was higher in patients with a higher level of PD-L1 (PD-L1>=5% - 28.4%, PD-L1>=1%- 23.8%, and PD-L1<1% - 16.1%). Furthermore, the median overall survival was higher as well in patients with a higher PD-L1 level, as seen in Figure 2. Similar results have been shown when patients were given Durvalumab 5 and Avelumab6.
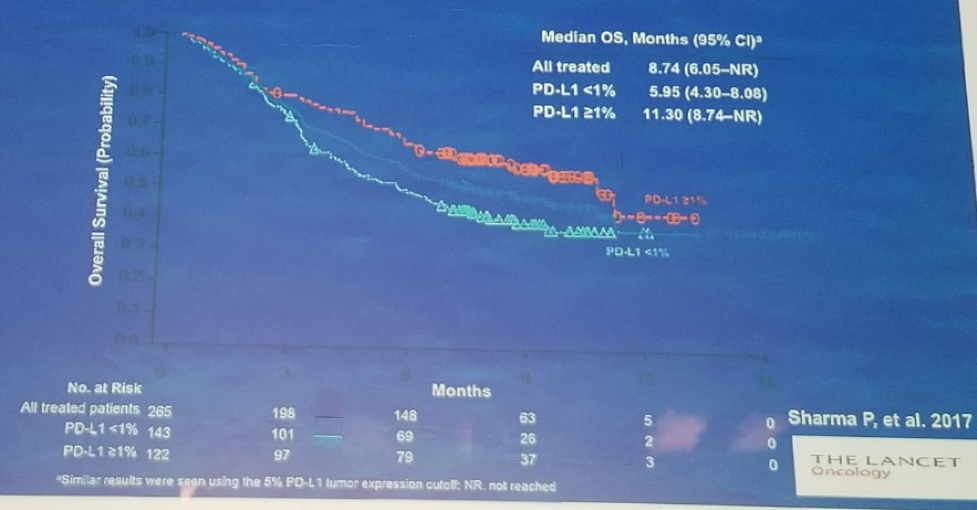
Figure 2- Overall survival rates in metastatic patients given salvage Nivolumab therapy stratified by PD-L1 level:
In the KEYNOTE-045 (NCT 02256436) trial 7 metastatic urothelial carcinoma patients after 1-2 lines of platinum-based chemotherapy or recurrence <12 months after perioperative platinum-based therapy, were randomized to either Pembrolizumab or chemotherapy (Paclitaxel, Docetaxel, and Vinflunine). Over 98% of patients in both these arms were in good performance status (ECOG 0,1), but almost 35% of patients in both arms had liver metastases, which is a poor prognostic sign. The results of this trial were quite promising, demonstrating a median survival of 10.3 months in the Pembrolizumab arm compared to 7.4 months in the chemotherapy arm, with a hazards ratio of 0.7 (95% C.I. 0.57-0.86), p<0.0001. Longer follow-up of this trial confirms initial data, and objective responses occurred rapidly and were generally durable, with duration of responses not yet reached. Lastly, the safety and tolerability support Pembrolizumab over the 2nd/3rd line chemotherapy.
A trial with a similar patient population, the IMvigor2118 randomized patients to receive either Atezolizumab or the investigator’s choice of chemotherapy (figure 3). After a median follows up of 17.3 months, in the intention to treat analysis this trial showed an overall survival benefit to the Atezolizumab arm, with a median overall survival of 8.6 months compared to 8 months in the chemotherapy arm (figure 4).
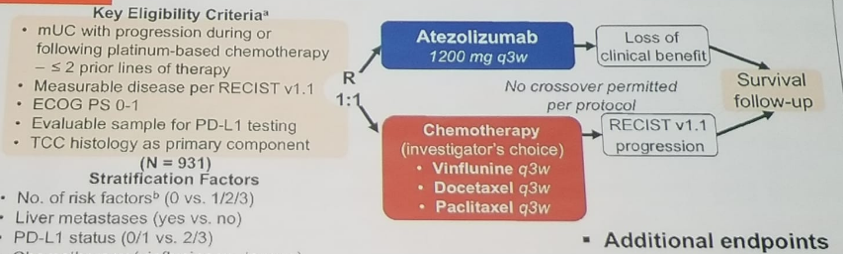
Figure 3 – The IMvigor 211 trial design:
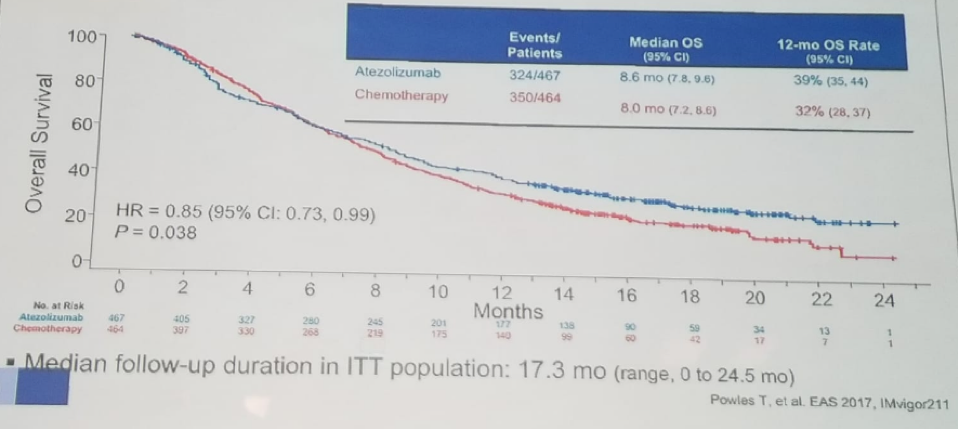
Figure 4 – Intention to treat overall survival analysis in the IMvigor 211 trial:
Table 1 summarizes the various immune checkpoint inhibitor trials in the salvage setting of metastatic bladder cancer, demonstrating the relatively similar overall response rate in all immune checkpoint inhibitors.
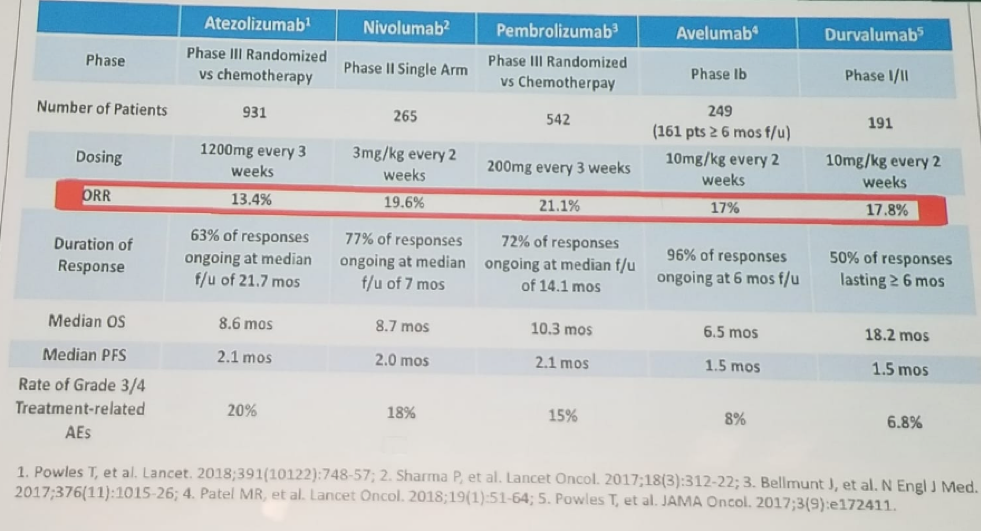
Table 1 – Summary of all immune checkpoint inhibitor trials in the salvage setting of metastatic bladder cancer:
The last topic discussed by Dr. Grivas was the role of immune checkpoint inhibitors as first-line therapy for cisplatin-ineligible patients in advanced urothelial carcinoma patients. There are overall two studies, examining Atezolizumab (the phase 2 IMvigor cohort one trial) 9, and Pembrolizumab (the phase 2 KEYNOTE-052 trial)10. Table 2 summarized these two studies demonstrating an overall response rate of between 23%-29% with complete response rates of 7-9%. The median overall survival was 15.9 months in the Atezolizumab and not yet reached in the Pembrolizumab trial. The grade 3 and four complication rates were 16-19%.
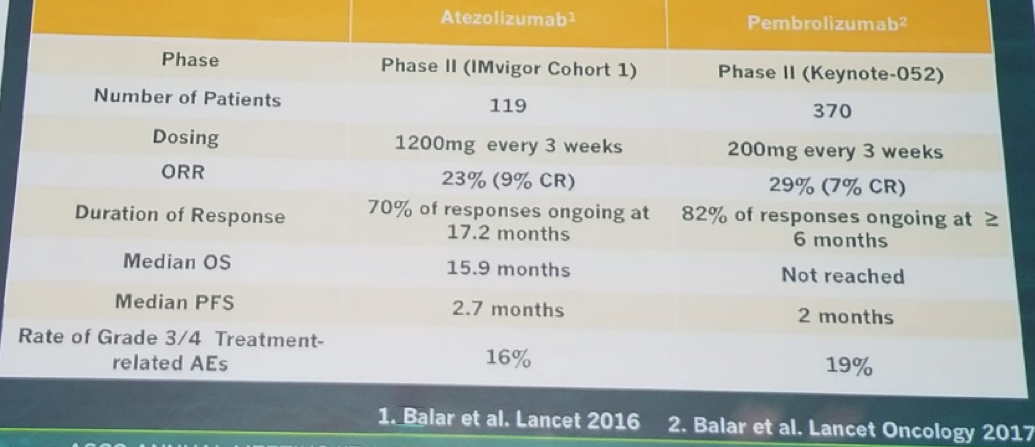
Table 2 – Summary of the two immune checkpoint inhibitor trials assessing Atezolizumab and Pembrolizumab as 1st line therapy for cisplatin ineligible advanced urothelial carcinoma patients.
Dr. Grivas concluded his encompassing talk by providing a very useful algorithm for the treatment of advanced urothelial carcinoma patients, based on the results of these recently discussed trials. This algorithm (Table 3) gives the level 1 evidence for each setting and stage of patients with advanced urothelial carcinoma. Dr. Grivas concluded and said that clinical trials are therefore critical throughout the disease spectrum and treatment settings.

Table 3 – Advanced urothelial carcinoma treatment algorithm based on level evidence acquired from recent trials:
Presented by: Petros Grivas, medical oncologist at Seattle Cancer Care Alliance, Clinical Director, of the Genitourinary Cancers Program at the University of Washington Medicine and an Associate Professor of the Department of Medicine, Division of Oncology at the University of Washington School of Medicine, Washington, US
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at the Global Conference on Bladder Cancer 2018 - September 20-21, 2018 Madrid, Spain
References:
1. Von der Masse H et al. J Clin Oncol 2000
2. Sonpavde G et al. Lancet Oncol 2010
3. Drecier R et al. ASCO 2016
4. Sharma P et al. Lancet Oncol 2017
5. Massard C et al. J Clin Oncol 2016
6. Patel et al. GU symposium ASCO 2017
7. Bajorin D et al. ASCO 2017
8. Powles T. et al. EAS 2017, IMvigor 211
9. Balar et al. Lancet 2016
10. Balar et al. Lancet Oncol 2017