Dr. Kamat talked about several barriers that currently restrict our progression in improving outcomes in NMIBC. The first barrier discussed was the fact that NMIBC is not a homogenous disease state. One of the major causes of heterogeneity in urothelial cancers is the existence of variant histology. Approximately 44% of cases with variant histology are not recognized by community pathologists, and the discordance rate between transurethral resection of bladder tumors (TURBT) and radical cystectomy is in the range of 39-47%.1,2 These variant histologies, often very aggressive histologies include lymphoepithelial, plasmacytoid, nested variant, micropapillary, and small cell histology.
Another problem is the lack of a standardized definition of disease risk groups among the guidelines. According to the European Association of Urology (EAU) guidelines any high-grade tumor, and T1 tumors are considered high-risk disease, while according to the American Urologic Association (AUA) guidelines, these are considered part of intermediate risk disease. Therefore, Dr. Kamat suggests using a more simplified definition, whereby low-risk disease is defined by solitary, primary, Ta low-grade tumors less than 3 cm, and high-risk disease is defined by any T1 or high-grade disease, including CIS. Anything not meeting the definition of high or low-risk disease is considered intermediate risk.3 According to Dr. Kamat, intermediate risk tumors can include 4 risk factors – multiple tumors, tumor size >=3 cm, early recurrence (<1 year), and frequent recurrences (>1/year). If none of these 4 risk factors are present, we should treat this patient as if he has low-risk disease. If 1-2 of these risk factors are present, the disease should be treated as an intermediate disease, and finally, if 3 or more risk factors are present, it should be treated as a high-risk disease4, as shown in Figure 1. Another cause of lack of homogeneity is the fact that bladder cancer has also had several molecular classifications to various subtypes through the years, originating from various institutions, as shown in Figure 2.
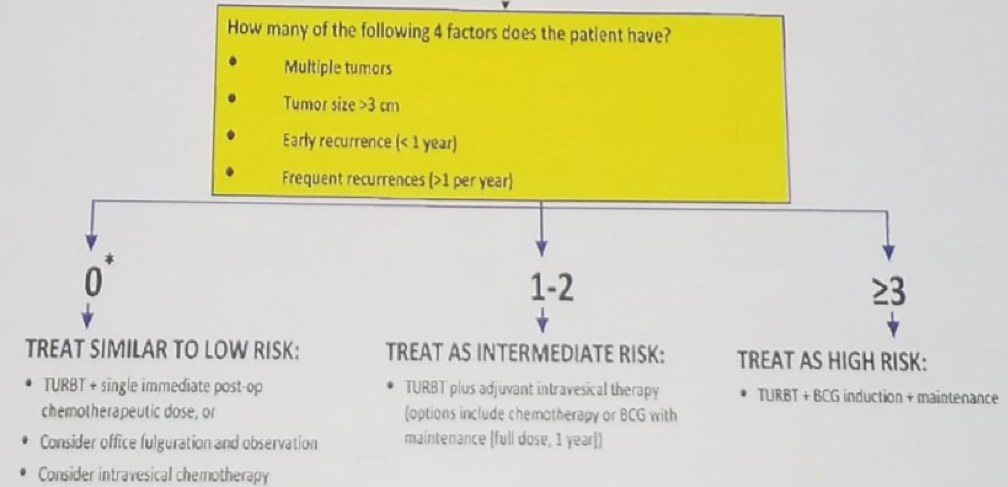
Figure 1 – How to treat intermediate-risk urothelial carcinoma:
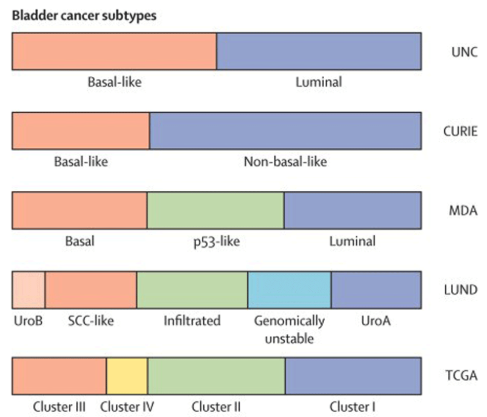
Figure 2 – Bladder cancer molecular subtypes
The second barrier discussed is the fact that the gold standard of tumor detection, which is cystoscopy, is considerably flawed. Data from several publications show that by using standard white light cystoscopy, the residual disease rate at prior TURBT sites range from 27%-62%, and the rate of missed diagnosis of invasive bladder cancer (pathological stage T2) can reach up to 10% 5, as shown in figure 3.

Figure 3 – Residual disease at prior TURBT site:
Because of this high residual rate, the concept of fluorescence cystoscopy (Cysview®) has been introduced. Cysview® is an optical imaging agent used in the cystoscopic detection of bladder carcinoma, including CIS. It is used with the KARL STORZ D-Light C Photodynamic Diagnostic (PDD) system enabling the performance of blue light cystoscopy, utilized as an adjunct to the white light cystoscopy. Pivotal studies have shown that blue light cystoscopy (Cysview®) had diagnosed a tumor in 16.4% of patients, and 32% were diagnosed with CIS, only when Cysview® was added. 6,7 Another added benefit of Cysview® is the significant increase in time to recurrence that it brings, from 9.4 months in standard white light cystoscopy to 16.4 months in Cysview®, p=0.04.8 Furthermore, a meta-analysis including five studies with 1301 patients demonstrated that it also causes a decrease in the rate of progression from 10.7% in white light cystoscopy to 6.8% in Cysview®. Lastly, it increases the time to progression. 9,10
The next barrier discussed is the fact that the definition of BCG failure has only recently been standardized. When BCG failure is diagnosed, it must include a clear definition of adequate of prior BCG therapy. This must include BCG induction (for six weeks) plus at least one BCG maintenance cycle (for three weeks). It is important to remember that BCG reduces progression rates only when maintenance therapy is used, according to a large meta-analysis.11 Different maintenance protocols have been assessed, but only the Southwest Oncology Group (SWOG) protocol (three weekly maintenance BCG instillations at 3, 6, 12, 18, 24, 30, and 36 months) have been demonstrated to decrease the rate of tumor recurrence.12 The timing of defining BCG failure must occur at the six months’ time point after diagnosis of high-risk tumor. 13
The last barrier discussed is the elusiveness of predictive markers. When trying to predict response to BCG therapy, some clinical factors have been shown to be useful. These include disease grade, stage, the presence of recurrent tumors, multiplicity, the presence of CIS, female gender and patient’s age. Other factors have shown to be probably useful. These include tumor molecular biomarkers and host genomic signature. Emerging strategies include the usage of bladder cancer molecular subtypes.14 It is known that bladder cancer is relatively a high immunogenic cancer with a high rate of neoantigen formation. The IMvigor 210 trial assessed the role of the Atezolizumab, an anti-PD-L1 monoclonal antibody in patients with locally advanced or metastatic urothelial bladder cancer. This trial showed that in patients who responded to treatment with Atezolizumab, there was a higher mutational load. This demonstrates the need for immunologic markers lighting the way and showing us which patients will better respond to immunologic treatment.
Dr. Kamat concluded his comprehensive talk stating that there are currently many early stage (NMIBC) urothelial carcinoma trials, assessing the role of immunologic therapy, with results anticipated in the next few years. Hopefully, these results will help us improve patient outcomes and assist us in overcoming the barriers of treating NMIBC patients.
Presented by: Ashish M. Kamat, MD is a Professor (Tenure) of Urology and Director of Urologic Oncology Fellowship at M.D. Anderson Cancer Center
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Twitter:@GoldbergHanan at the Global Conference on Bladder Cancer 2018 - September 20-21, 2018 Madrid, Spain
References:
1. Abd El Latif et al. J Urol 2013
2. Shah RB et al. Urol Onc 2012
3. Brausi M et al. IBCG 2011
4. Kamat et al. J Urol 2014
5. Jaske et al. Eur Urol 2004
6. Stenzl A et al. J Urol 2010
7. Burger M et al. EAU 2012
8. Grossman J et al. Urology 2012
9. Gakis et al. Bladder Cancer, 2016
10. Kamat et al. Bladder Cancer 2016
11. Sylvester RJ et al. J Urol 2002
12. Kamat A. & Porten, et al. Eur Urol 2014
13. Kamat et al. JCO 2016
14. Kamat et al. Eur Urol 2017
WATCH Video Interview: Setting the Stage for the BCG Unresponsive Population - Interview with Ashish Kamat