Known risk factors include phimosis, chronic penile inflammation, sporalene and ultraviolet A phototherapy for various dermatological conditions such as psoriasis. Additional risk factors include smoking, human papilloma virus infection, rural areas and low socioeconomic status, and history of multiple sexual partners with early age at first intercourse. Figure 1 demonstrates the distribution of cases diagnosed by anatomical site, and figure 2 shows the most recent 8th TNM staging of penile cancer.
The traditional management included radical surgery, with excision of the lesion and a 2 cm margin. This resulted in excellent oncological control with a 0.7% and 4.6% recurrence rate after total penectomy and partial penectomy, respectively. However, this also resulted in poor cosmetic and functional results with significant psychological and sexual morbidity. It has been shown that patients having more mutilating surgery, were more likely to have impaired well-being, pathologic anxiety (31%), post-traumatic stress disorder (40%), and avoidance behavior (25%). Therefore, there has been an attempt to use penile preserving surgery instead, in order to avoid the significant emotional and sexual morbidity associated with radical surgery.
The European association of Urology (EAU) guidelines recommend obtaining a penile MRI with artificial erection in cases for which organ preserving is intended. MRI results have demonstrated good correlation to histologic staging, with the following stage specific sensitivities and specificities calculated: T1 (85%, 83%), T2 (75%, 89%), and T3 (88%, 98%). MRI accurately predicted corpora cavernosum invasion in all cases of pathologically proven disease.
There is lack of high quality data regarding quality of life in penile cancer. Most studies are retrospective with small numbers of patients, with no standardization of methodology, or of treatment groups. It is important to standardize the method of assessment to accurately clarify the impact of disease and treatment type on quality of life, so that we could further refine management.
Figure 1: Distribution of penile cancer cases by anatomical site

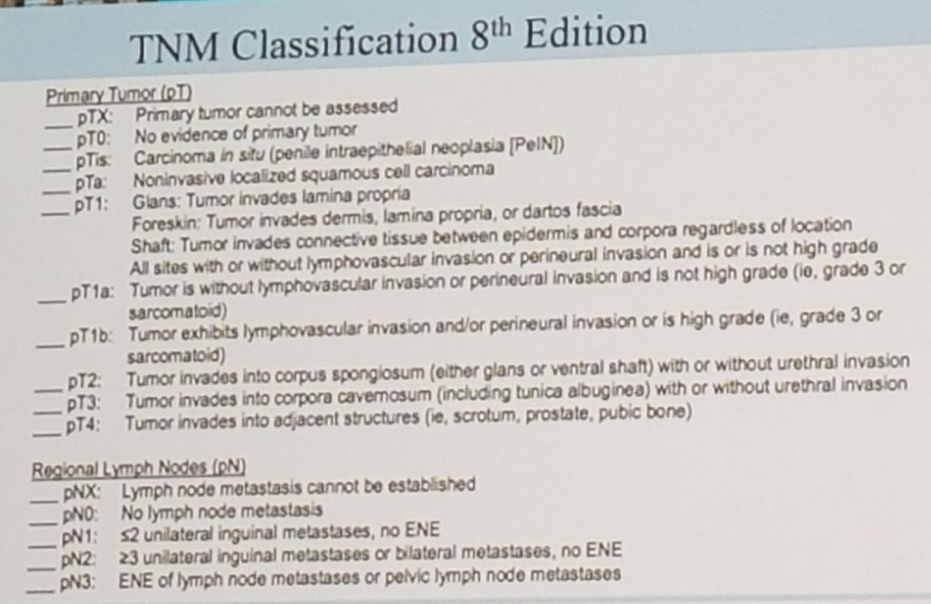
Figure 2: Penile cancer 8th TNM staging:
Speaker: Suks Minhas, University College Hospital London, United Kingdom
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at The 15th Meeting of the EAU Section of Oncological Urology ESOU18 - January 26-28, 2018 - Amsterdam, The Netherlands