As follows is an overview figure of research topics in renal cancer papers stratified by the journal of publication: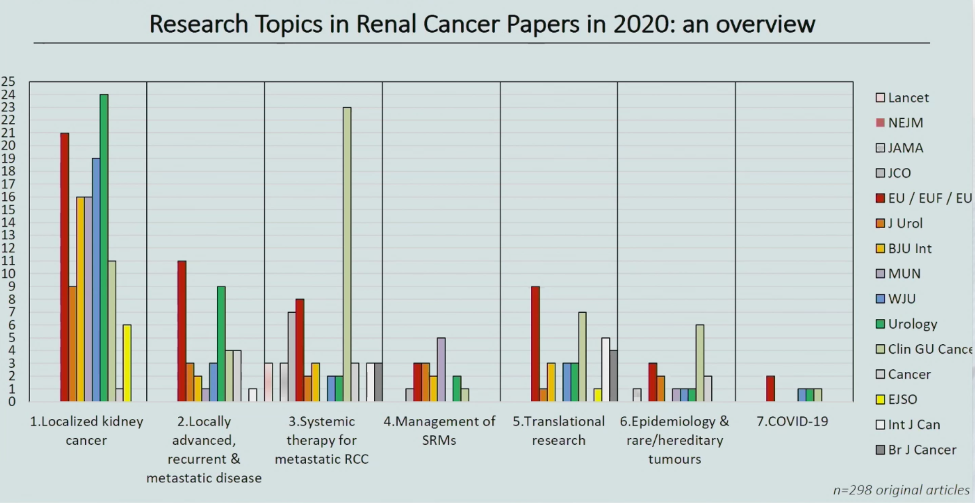
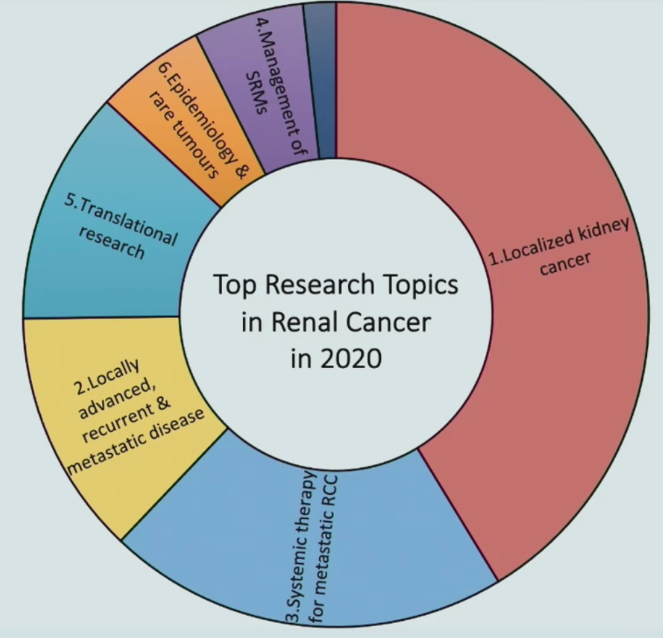
The first paper discussed by Dr. Campi was by Rossi et al. entitled “Essential Research Priorities in Renal Cancer: A Modified Delphi Consensus Statement” published in European Urology Focus1. The goal of this study was to identify research priorities in renal cell carcinoma through multidisciplinary collaboration between clinicians, researchers, and patients. In Phase I, 44 renal cell carcinoma experts provided 24 literature reviews within their field, summarizing key research gaps. Three expert discussion meetings and patient interviews were performed, and 39 potential research gaps were identified. In Phase II, experts (n=82) scored these gaps on a nine-point scale (1-3: not important; 4-6: important; 7-9: critical) through a multistep Delphi process involving three online surveys and two further consensus meetings. The process resulted in the identification of 14 crucial research gaps, across a broad range of renal cell carcinoma themes. As follows is a summary of the 14 crucial research gaps: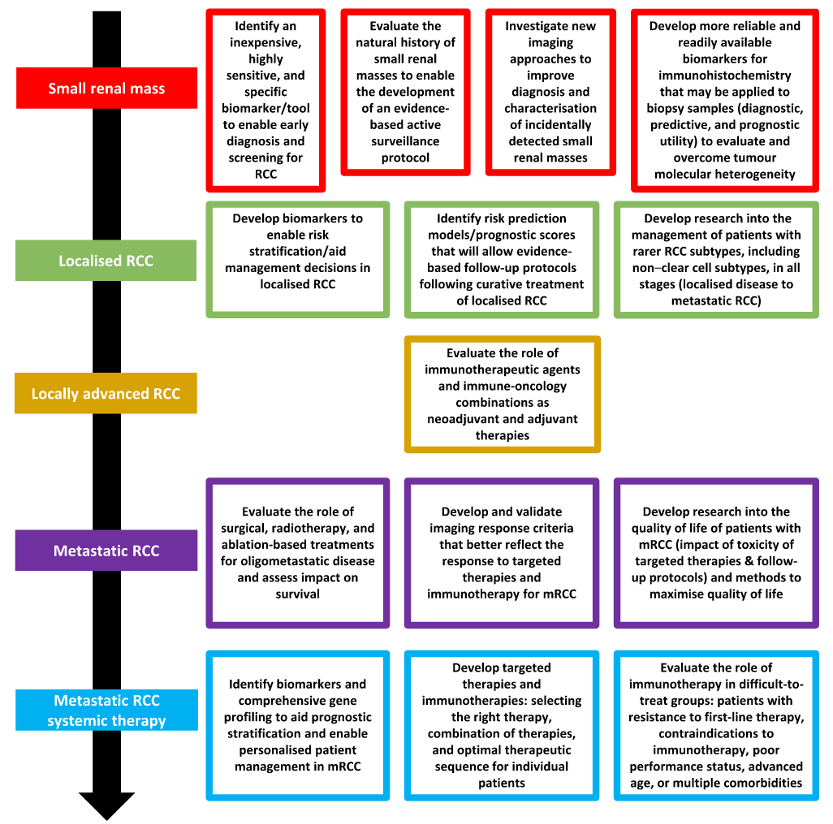
Two crucial research gaps relate to biomarkers and novel imaging approaches for both localized and metastatic disease, to enable prognostic risk stratification and individualize patient management.
The second paper selected by Dr. Campi was by Porpiglia et al. and titled “Three-Dimensional Augmented Reality Robot-Assisted Partial Nephrectomy in Case of Complex Tumors (PADUA ≥ 10): A New Intraoperative Tool Overcoming the Ultrasound Guidance” published in European Urology.2 The objective of this study was to evaluate the accuracy of our three-dimensional static and elastic augmented reality systems based on hyper accuracy models (HA3D) in identifying tumors and intrarenal structures during transperitoneal robotic-assisted partial nephrectomy, compared with standard ultrasound:
Among 91 patients included in this study, the use of three-dimensional augmented reality guidance made it possible to correctly identify the lesion and intraparenchymal structures with a more accurate three-dimensional perception of the location and the nature of the different structures relative to the standard two-dimensional ultrasound guidance. This translates to a lower rate of global ischemia (45.8% in the three-dimensional group vs. 69.7% in the ultrasound group; p = 0.03), higher rate of enucleation (62.5% vs. 37.5% in the three-dimensional and ultrasound groups, respectively; p = 0.02), and lower rate of collecting system violation (10.4% vs. 45.5%; p = 0.003). Dr. Campi notes that the HA3D models that overlap in vivo anatomy during robotic-assisted partial nephrectomy for complex tumors can be useful for identifying the lesion and intraparenchymal structures that are difficult to visualize with ultrasound alone.
The next study discussed by Dr. Campi was by Abu-Ghanem et al. entitled “The Impact of Histological Subtype on the Incidence, Timing, and Patterns of Recurrence in Patients with Renal Cell Carcinoma After Surgery—Results from RECUR Consortium” published in European Urology Oncology.3 The goal of this study was to determine the impact of renal cell carcinoma histological subtype on recurrence and to examine the incidence, pattern, and timing of recurrences. There were 3,331 patients that were included all of which were treated surgically with curative intention (ie, radical and partial nephrectomy) for nonmetastatic renal cell carcinoma (cT1-4, M0) between 2006 and 2011 across 15 centers from 10 countries. A total of 2,565 patients (77.0%) had clear-cell renal cell carcinoma, 535 (16.1%) had papillary renal cell carcinoma, and 231 (6.9%) had chromophobe renal cell carcinoma. The median postoperative follow-up period was 61.7 (interquartile range: 47-83) months. Patients with clear cell renal cell carcinoma had significantly poorer 5-yr recurrence-free survival (RFS) than patients with papillary and chromophobe renal cell carcinoma (78% vs. 86% vs. 91%, p = 0.001). The patterns of recurrence stratified by subtype are as follows:
The key take-home messages from this study according to Dr. Campi are as follows:
- For clear cell renal cell carcinoma, the most common site for recurrence was the lung in 50.4% of patients and the median time to recurrence was 21.2 months (IQR 7.9-41.1) months; 65 patients (13.5%) recurred >5 years after surgery
- For papillary renal cell carcinoma, the most common site of recurrence was the lung in 35.8% of patients and the median time to recurrence was 19 months (IQR 8.6-41.1) months; only 9 patients recurred >5 years after surgery
- For chromophobe renal cell carcinoma, the most common site of recurrence was bone in 29.4% of patients and the median time to recurrence was 37.4 months (IQR 11.1-64.6); six patients recurred >5 years after surgery
- The current results emphasize the need for evidence-based standards and risk assessment to counsel patients and tailor subtype-specific follow-up, and to avoid overuse or to increase the frequency of imaging modalities where necessary
The next paper discussed by Dr. Campi was by Ball et al. entitled “Growth Rates of Genetically Defined Renal Tumors: Implications for Active Surveillance and Intervention” published in the Journal of Clinical Oncology.4 The goal of this study was to evaluate the growth of genetically defined renal tumors and their association with patient clinical and genetic characteristics. In this cohort from the National Cancer Institute (NCI), there were 292 patients with 435 genetically defined tumors were identified, including 286 VHL-deficient, 91 FLCN-deficient, 52 MET-activated, and 6 BAP1-deficient tumors. The median follow-up was 3.6 years (IQR 2.0-5.6 years) and the median tumor growth rate for the entire cohort was 0.31 cm per year. Notably, BAP1-deficient tumors had the fastest median growth rate (0.6 cm/y, IQR 0.57-0.68 cm/y), followed by VHL-deficient tumors (growth rate 0.37 cm/y, IQR 0.25-0.57 cm/y), FLCN-deficient tumors (growth rate 0.10 cm/y, IQR 0.04-0.24 cm/y), and tumors with MET activation (growth rate 0.15 cm/y, IQR 0.053-0.32 cm/y; p < 0.001). When stratifying all tumors by histologic subtype, clear cell renal cell carcinoma had a significant growth rate of 0.37 cm/year, followed by papillary type 1 at 0.15 cm/year, chromophobe at 0.15 cm/year, and hybrid oncocytic tumors at 0.11 cm/year. Specifically related to VHL patients, young patients had faster-growing tumors: 0.40 cm/year vs 0.34 cm/year. As follows is a layered pie-chart of histology and genetic alteration: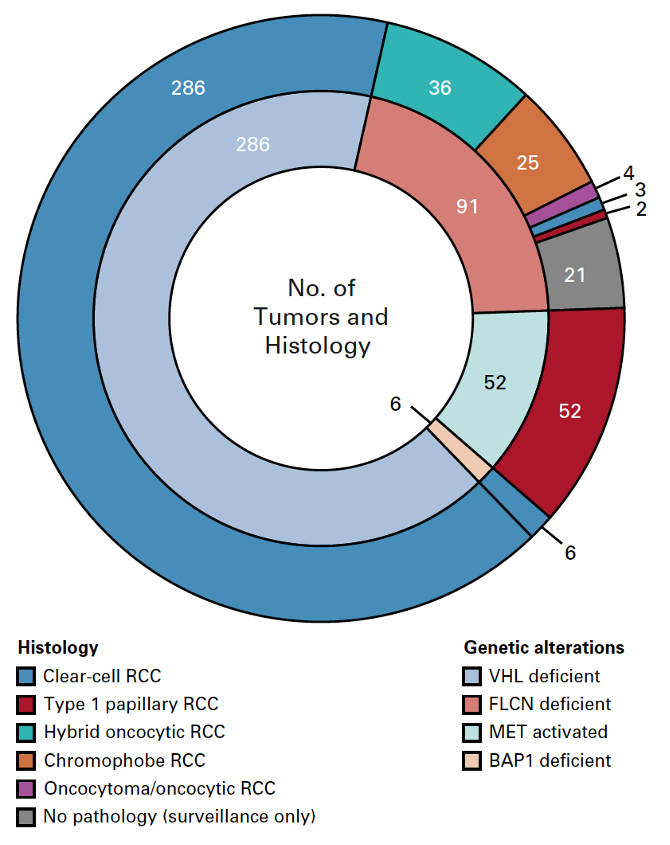
Dr. Campi notes that whereas the current study evaluated patients with germline variants, these findings have broader implications for patients with sporadic renal cell carcinoma. Taken together, these data suggest that understanding the biology of hereditary kidney cancer informs our understanding of both the biology and clinical management of sporadic kidney cancer. Additional studies are needed to determine the impact of somatic mutations on tumor development and growth kinetics and the role of somatic gene mutation analysis in the active surveillance management of patients with sporadic renal cell carcinoma.
The final paper discussed by Dr. Campi was by Derosa et al. entitled “Gut Bacteria Composition Drives Primary Resistance to Cancer Immunotherapy in Renal Cell Carcinoma Patients” published in European Urology.5 The objective of this study was to evaluate the predictive value of stool bacteria composition for immune checkpoint blockade efficacy in a cohort of advanced renal cell carcinoma patients. There were 69 fecal samples collected from advanced RCC patients treated with nivolumab and enrolled in the GETUG-AFU 26 NIVOREN microbiota translational substudy Phase II trial, in addition to 2,994 samples of feces from healthy volunteers. The authors found that recent antibiotic use (16%) reduced objective response rates from 28% to 9% (p < 0.03) and markedly affected the composition of the microbiota. The authors also performed concomitant preclinical studies in renal cell carcinoma-bearing mice that received a fecal transplant from renal cell carcinoma patients resistant to immune checkpoint blockade, which allowed assessment of a cause-effect relationship between gut bacteria composition and clinical outcomes for immune checkpoint blockade. They found that these mice were successfully compensated with either fecal transplant from responding renal cell carcinoma patients or beneficial commensals identified by whole-genome sequencing metagenomics data (Akkermansia muciniphila and Bacteroides salyersiae).
Presented by: Riccardo Campi, MD, Guidelines Office, European Association of Urology, Arnhem, The Netherlands
Written by: Zachary Klaassen, MD, MSc, Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Augusta, Georgia, Twitter: @zklaassen_md during the 18th Meeting of the EAU Section of Oncological Urology (ESOU21), January 29-31, 2021
References:
1. Rossi, Sabrina H., Christopher Blick, Catherine Handforth, Janet E. Brown, and Grant D. Stewart. "Essential research priorities in renal cancer: a modified delphi consensus statement." European urology focus 6, no. 5 (2020): 991-998.
2. Porpiglia, Francesco, Enrico Checcucci, Daniele Amparore, Federico Piramide, Gabriele Volpi, Stefano Granato, Paolo Verri et al. "Three-dimensional augmented reality robot-assisted partial nephrectomy in case of complex tumours (PADUA≥ 10): a new intraoperative tool overcoming the ultrasound guidance." European urology 78, no. 2 (2020): 229-238.
3. Abu-Ghanem, Yasmin, Thomas Powles, Umberto Capitanio, Christian Beisland, Petrus Järvinen, Grant D. Stewart, Eiríkur Orri Gudmundsson et al. "The Impact of Histological Subtype on the Incidence, Timing, and Patterns of Recurrence in Patients with Renal Cell Carcinoma After Surgery—Results from RECUR Consortium." European Urology Oncology (2020).
4. Ball, Mark W., Julie Y. An, Patrick T. Gomella, Rabindra Gautam, Christopher J. Ricketts, Cathy D. Vocke, Laura S. Schmidt et al. "Growth rates of genetically defined renal tumors: implications for active surveillance and intervention." Journal of Clinical Oncology 38, no. 11 (2020): 1146-1153.
5. Derosa, Lisa, Bertrand Routy, Marine Fidelle, Valerio Iebba, Laurie Alla, Edoardo Pasolli, Nicola Segata et al. "Gut bacteria composition drives primary resistance to cancer immunotherapy in renal cell carcinoma patients." European urology 78, no. 2 (2020): 195-206.