Dr. Ribal notes that the reason the EAU guidelines are leaders in the field is because of the international engagement, Cochrane review methodology, multidisciplinary collaboration, and the EAU Guidelines Associates Programme.
With regards to diagnosis, therapy, and follow-up, the group delineated several levels of priority:
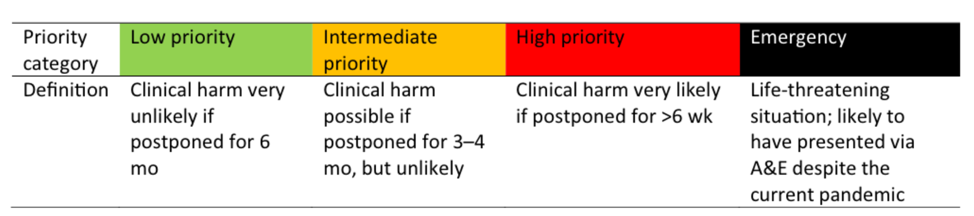
- Low priority: clinical harm very unlikely if postponed for 6 months
- Intermediate priority: clinical harm possible if postponed 3-4 months, but unlikely
- High priority: clinical harm very likely if postponed >6 weeks
- Emergency: a life-threatening situation, with the patient likely to have to present to the emergency department despite the current pandemic
The criteria for prioritization regarding procedure and disease established by the group are as follows:
- Impact of delay on primary outcomes (for instance overall survival in oncology, cancer-specific survival in oncology, risk of metastases, and kidney failure for transplant patients)
- Possibility of alternative methods that could replace the procedure with less operating room requirement. Presence of comorbidities and/or increased risk of complications
- Possibility of a threat to patient life if the procedure is not performed immediately
- Possibility of a threat of permanent dysfunction of the organ system if the treatment is not performed
- Probability of a risk of rapidly progressing severe symptoms that are time-sensitive
- Depending on the resources and capacity, the group recommends treating only high-priority and emergency cases surgically during the COVID pandemic
- Consider not only equipment, OR, and ICU bed capacity, but also blood supplies available and drug shortage, in order to prioritize surgeries
- Consider that even if capacity is available, low-priority patients increase the footfall and the risk of COVID transmission between patients and staff
- Consider that surgery has been reported to be harmful in asymptomatic patients who subsequently tested COVID positive
- Consider treating intermediate-priority patients if capacity is available but not during the COVID surge
- Consider older patients with comorbidities at severe risk of COVID infection and a fatal outcome. Therefore, carefully balance if surgery is the only alternative in high-priority cases
- Where ventilator capacity for COVID patients has been breached, high-priority surgical candidates requiring ICU ventilation should be triaged according to local recommendations—or if unavailable—age and comorbidity
- Follow the local recommendations to test staff and patients for COVID, if resources are available. These may differ across hospitals and countries and urologists should familiarize themselves with these recommendations and be aware that they may change as new information is coming in
- Follow the local recommendations for personal protective equipment (PPE), if resources are available; the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) advise full PPE irrespective of COVID status of the patient. Urologists should familiarize themselves with the SAGES recommendations
- Wear full PPE for COVID-positive patients according to the World Health Organization (WHO). This should include double gloves, gowns, face shields, and virus-proof masks
- Intubation and extubation should preferably take place in a negative pressure room if available
- All nonessential staff should stay outside the operating room during the procedure
- Set electrosurgery units to the lowest possible settings to reach the required effect
- Avoid or reduce the use of monopolar electrosurgery, ultrasonic dissectors, and advanced bipolar devices, as these can lead to particle aerosolization
- Use, if available, monopolar diathermy handheld devices with attached smoke evacuators
- Clean surgical equipment of COVID-positive or suspected patients separately
- Utilize telemedicine as much as possible
- Potential or proven COVID-19–positive patients must be treated according to local, national, and WHO requirements. In this case, a comprehensive and robust infection control workflow has to be followed
- A network of expert high-volume centres, at the regional, national, or even supranational level, should guarantee the continuity of the oncological care in an appropriate way, ensuring the availability of hospital beds and timely management of new patients
- Remote consultation and a multidisciplinary team are recommended to offer the optimum therapeutics
- Testing for SARS-CoV-2 should be considered before any high-dose chemotherapy
- Patients should be guided to get access to non-emergency medical services such as chronic disease treatment online to reduce the number of visitors in hospital
- Patients should be encouraged to take full advantage of digital self-service devices to avoid contact with others, to reduce the risk of cross infections
Dr. Ribal concluded her presentation with several take-home messages from the EAU Guidelines Office:
- The EAU is a family of 19,000 members and feels a huge sense of responsibility towards each and every urologist globally
- The extended family ethos is even more important at this point in time during the pandemic
- Despite these incredibly difficult times, key opinion leaders across the EAU membership have come together to provide these recommendations for managing COVID-19 and urologic patients
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia Twitter: @zklaassen_md during the 18th Meeting of the EAU Section of Oncological Urology (ESOU21), January 29-31, 2021
References:
- Ribal MJ, Cornford P, Briganti A, et al. European Association of Urology Guidelines Office Rapid Reaction Group: An Organization-wide Collaborative Effort to Adapt the European Association of Urology Guidelines Recommendations to the Coronavirus Disease 2019 Era. Eur Urol. 2020;78:21-28.