(UroToday.com) The 2025 ESMO annual meeting featured a urothelial carcinoma mini oral session and a presentation by Jiwei Huang, MD, discussing results from the phase II DISTINCT-I trial assessing disitamab vedotin + tislelizumab as nephron-sparing therapy for high-risk upper tract urothelial carcinoma.
Radical nephroureterectomy remains standard for localized high-risk upper tract urothelial carcinoma, while functional nephron preservation has emerged as a universal clinical priority to optimize long-term patient outcomes. This phase II trial (DISTINCT-I) evaluates a novel kidney-sparing strategy combining endoscopic thulium laser ablation/ureteral segmental resection with perioperative HER2-targeted therapy (disitamab vedotin) + immune checkpoint inhibitors in high-risk upper tract urothelial carcinoma.
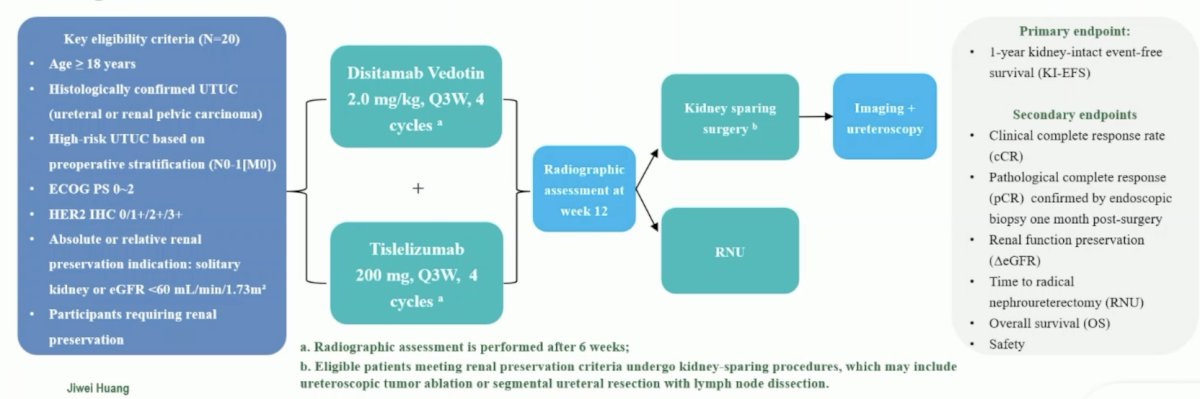
This ongoing study (NCT05912816, initiated September 2023 at Renji Hospital/Tianjin Second Hospital) enrolled high-risk upper tract urothelial carcinoma patients (N0-1[M0], absolute/relative renal preservation indications: solitary kidney or eGFR <60 mL/min/1.73m2). The protocol for this trial included endoscopic biopsy followed by 2-4 cycles of disitamab vedotin (2.0 mg/kg) + tislelizumab (200 mg) every 3 weeks for induction therapy, then kidney-sparing surgery. The primary endpoint was 1-year kidney-intact event-free survival (events: local recurrence, metastasis, death), and secondary endpoints included clinical complete response, renal function preservation, and safety (CTCAE v5.0). The trial design for DISTINCT-I is as follows:
Among 20 enrolled patients (median follow-up: 17.0 months, range: 12-26), the HER2 status by biopsy IHC was 3+ (n = 6), 2+ (n = 2), 1+ (n = 7), 0 (n = 4):
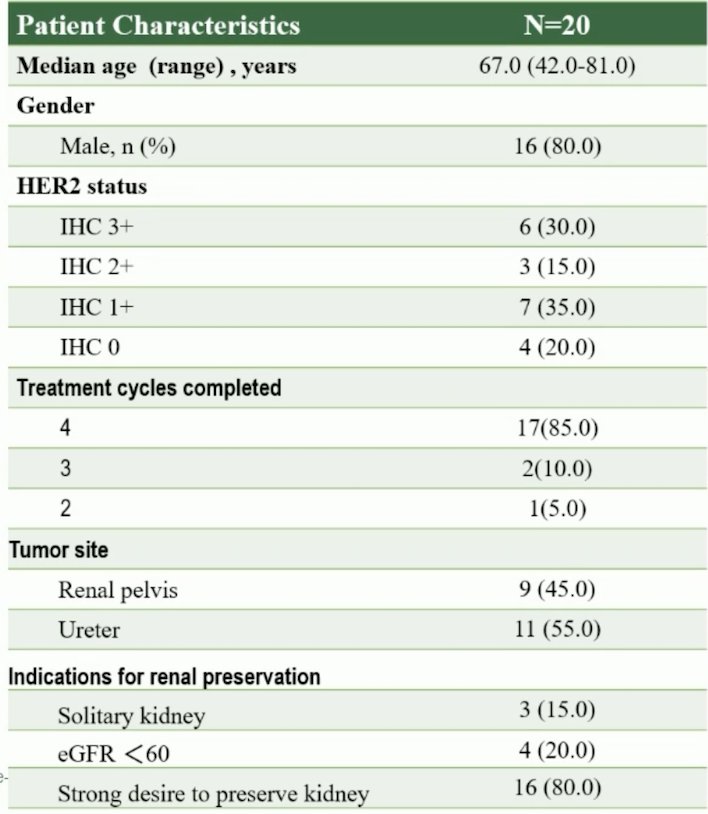
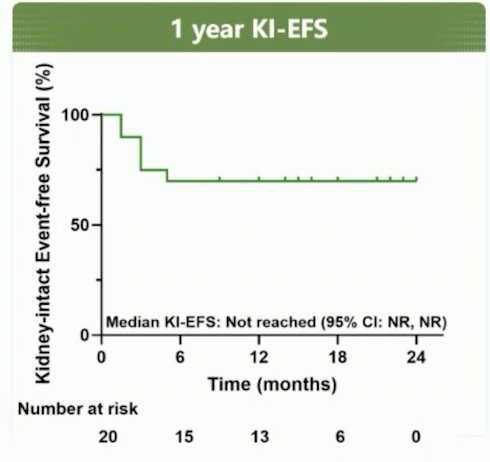
Most patients presented with cT1-2N0 disease (85%), with 3 patients having cT3N0/Nx disease (15%). The majority of patients (85%) successfully completed all 4 planned cycles of induction therapy. The kidney-intact event free survival at 1 year was 70%, and the clinical complete response rate increased from 25% after induction therapy to 75% following subsequent kidney sparing surgery (4-month assessment):
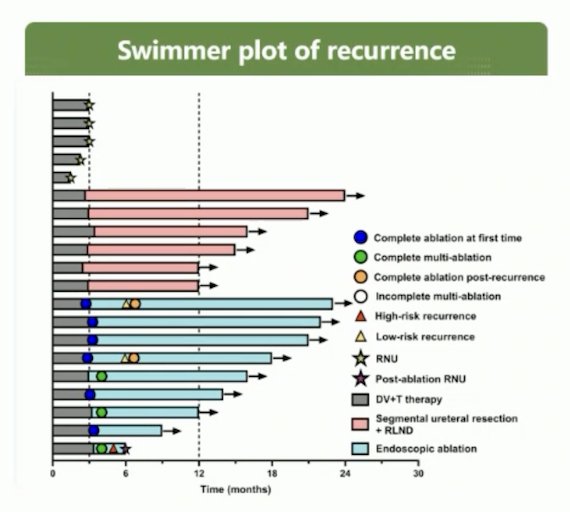
Kidney-sparing procedures included ureteral segmental resection (n = 5), endoscopic ablation (n = 9), and radical nephroureterectomy (n = 5). Regarding recurrence, three cases occurred in the ablation cohort, one of which was a high-risk recurrence at 5 months and underwent salvage radical nephroureterectomy. The other two were low risk recurrences at 6 months. The following figure highlights the swimmer plot of recurrence:
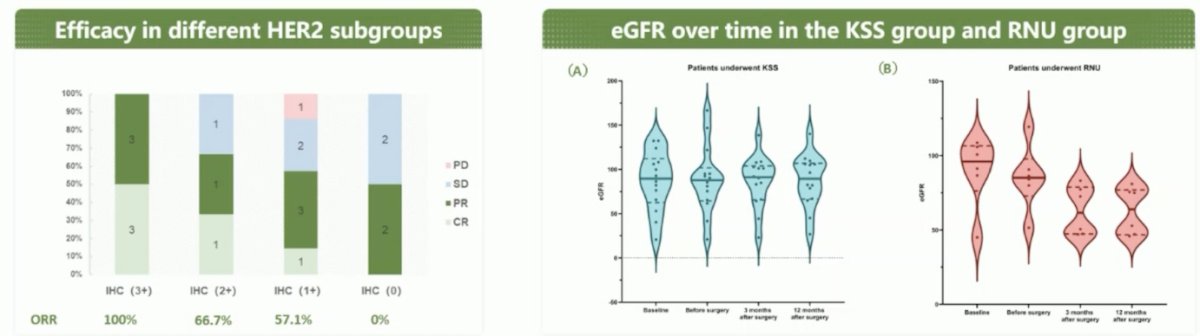
Tumor responses to induction therapy among the 20 patients included complete response (n = 5), partial response (n = 9), stable disease (n = 5), and progressive disease (n = 1), yielding an objective response rate of 70% and a disease control rate of 95%. Pathological examination confirmed a complete response in all 5 patients who had achieved a clinical complete response. Treatment efficacy was strongly linked to higher levels of HER2 overexpression (2+/3+). The following figures highlight the efficacy in different HER2 subgroups and eGFR over time in the kidney-sparing surgery group and the radical nephroureterectomy group:
There were no grade ≥3 systemic toxicities observed.
Dr. Huang concluded this presentation discussing results from the phase II DISTINCT-I trial with the following take-home points:
- The combination of disitamab vedotin and immune checkpoint inhibitors with kidney-sparing surgery demonstrates promising tumor downstaging and nephron preservation in high-risk upper tract urothelial carcinoma, with a favorable safety profile
- HER2 overexpression may predict enhanced response, supporting further biomarker validation
- This organ-preservation paradigm challenges the historical dominance of radical nephroureterectomy and represents a promising therapeutic strategy for selected patients with high-risk upper tract urothelial carcinoma
Presented by: Jiwei Huang, MD, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between September 17th and 21st.
Related Content:
Disitamab Vedotin plus Toripalimab in HER2-Expressing Advanced Urothelial Cancer