(UroToday.com) The 2025 ESMO annual meeting featured a metastatic castration-resistant prostate cancer (mCRPC) session and a presentation by Dr. Johann S. De Bono discussing emerging new therapeutic strategies for advanced prostate cancer. Dr. De Bono started his presentation by noting that there are several adaptations to androgen receptor blockade, which include:
- Androgen receptor increased expression, copy gain, mutation, splicing (loss of the ligand binding domain)
- Increased AKT phosphorylation due to feedback loops
- Chronic inflammatory cytokine release including IL-1β, IL-6, TGFβ1, CXCR2 ligands impacting T-cell function and myelomonocytic inflammation, with paracrine interactions between tumor cells and the stroma
- Lineage plasticity (reversible and ASCL1 dependent) associated with loss of androgen receptor dependency, epigenetic changes (EZH2/NSD2), including neuroendocrine and double negative prostate cancer (which is uncommon)
There are implications of this biology, specifically continued androgen receptor signaling in many if not most mCRPC. These tumors sometimes remain sensitive to targeting the androgen receptor ligand domain, for example with androgen receptor degraders. In the CC-94676-PCA-001 trial,1 BMS-986365 was tested in mCRPC patients who progressed on antiandrogen therapy including ≥ 1 androgen receptor pathway inhibitor (ie. enzalutamide, abiraterone). Patients had prior taxane chemotherapy unless ineligible or declined. Among the 68 patients, prior therapy included chemotherapy (n = 31; 46%), enzalutamide (n = 51; 75%), and abiraterone (n = 44; 65%). Overall, 46% received both enzalutamide and abiraterone. This study found that a clinical benefit of BMS-986365 was observed both in patients with androgen receptor ligand binding domain WT and mutant mCRPC:

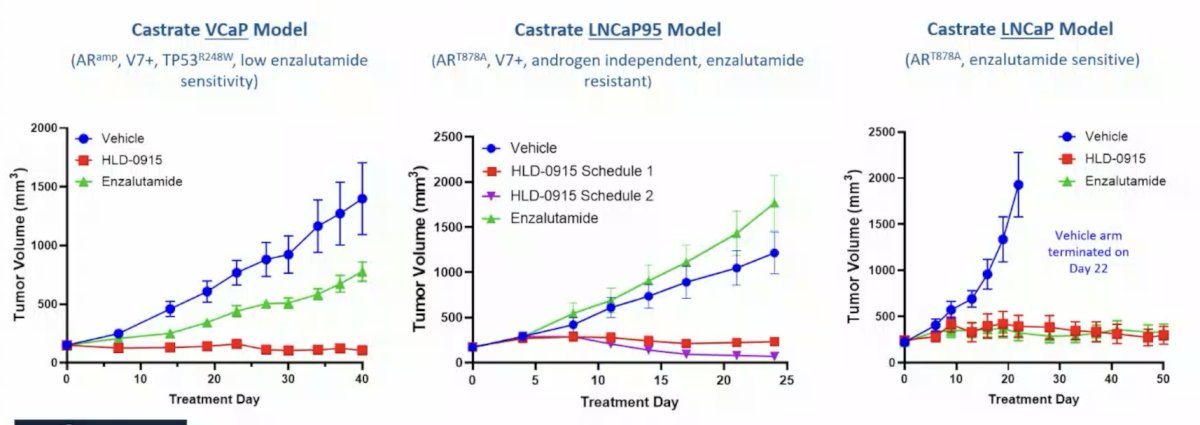
Androgen receptor signaling commonly remains a vulnerability, thus androgen receptor amino-terminus (targeting AR-SV signaling) has been a high priority, and RIPTACs can also target continued androgen receptor signaling as a bait to allow tumor targeting. Specifically, HLD-0915 is a RIPTAC with efficacy across preclinical CRPC models, showing tumor regression in enzalutamide insensitive models:
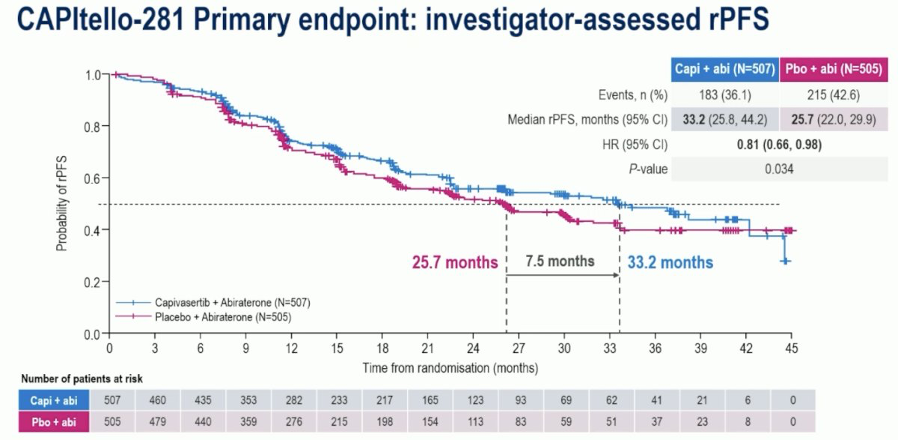
PI3K/AKT inhibitors have been assessed in clinical trials and may have molecular stratification challenges. Ipatasertib was shown to have a progression free survival benefit in androgen receptor pathway inhibitor mCRPC naïve patients in a phase 2 trial, as well as a phase 3 trial in combination with abiraterone versus abiraterone alone. However, the overall survival benefit prespecified requirements were not met. Capivasertib was assessed in a randomized phase 2 trial in mCRPC post androgen receptor pathway inhibitor, showing that in combination with enzalutamide versus enzalutamide alone, there was no progression free survival benefit. At ESMO 2025, Dr. Fizazi presented results of CAPItello-281, a randomized phase 3 trial in mHSPC assessing capivasertib + abiraterone versus abiraterone alone, demonstrating improved progression free survival (HR 0.81, 95% CI 0.66-0.98; p = 0.034), but with immature overall survival data:
Dr. De Bono also noted that abrogating myeloid infiltration abrogates androgen receptor pathway inhibitor resistance. In work from Guo et al.2, they showed decreased intratumor myeloid cells and resensitization to enzalutamide, as well as increasing chemokines activates CXCR1 after CXCR2 blockade:
![Dr. De Bono also noted that abrogating myeloid infiltration abrogates androgen receptor pathway inhibitor resistance. In work from Guo et al. [2], they showed decreased intratumor myeloid cells and resensitization to enzalutamide, as well as increasing chemokines activates CXCR1 after CXCR2 blockade:](/images/com-doc-importer/232-esmo-2025/esmo-2025-emerging-new-therapeutic-strategies-for-advanced-prostate-cancer/image-3.jpg)
In order to target lineage plasticity, elucidating strategies to block SNAI1 (impacts chromatin architecture) mediated EMT is required. Trials targeting EZH2/EED with androgen receptor blockade are ongoing, with data suggesting the presence of an RB1/E2F → EZH2 → NSD2 axis. EZH2 has canonical (H3K27me3) and non-canonical functions, and is part of the PRC2 complex that includes EED. Specifically, mevrometostat (an EZH2 inhibitor) phase 2 data has encouraged evaluation in a phase 3 trial.
Next. Dr. De Bono discussed cell surface protein targeting, which includes T-cell engagers, radiopharmaceuticals, and antibody drug conjugates. Dr. De Bono notes that there are many cell surface proteins for targeting:2
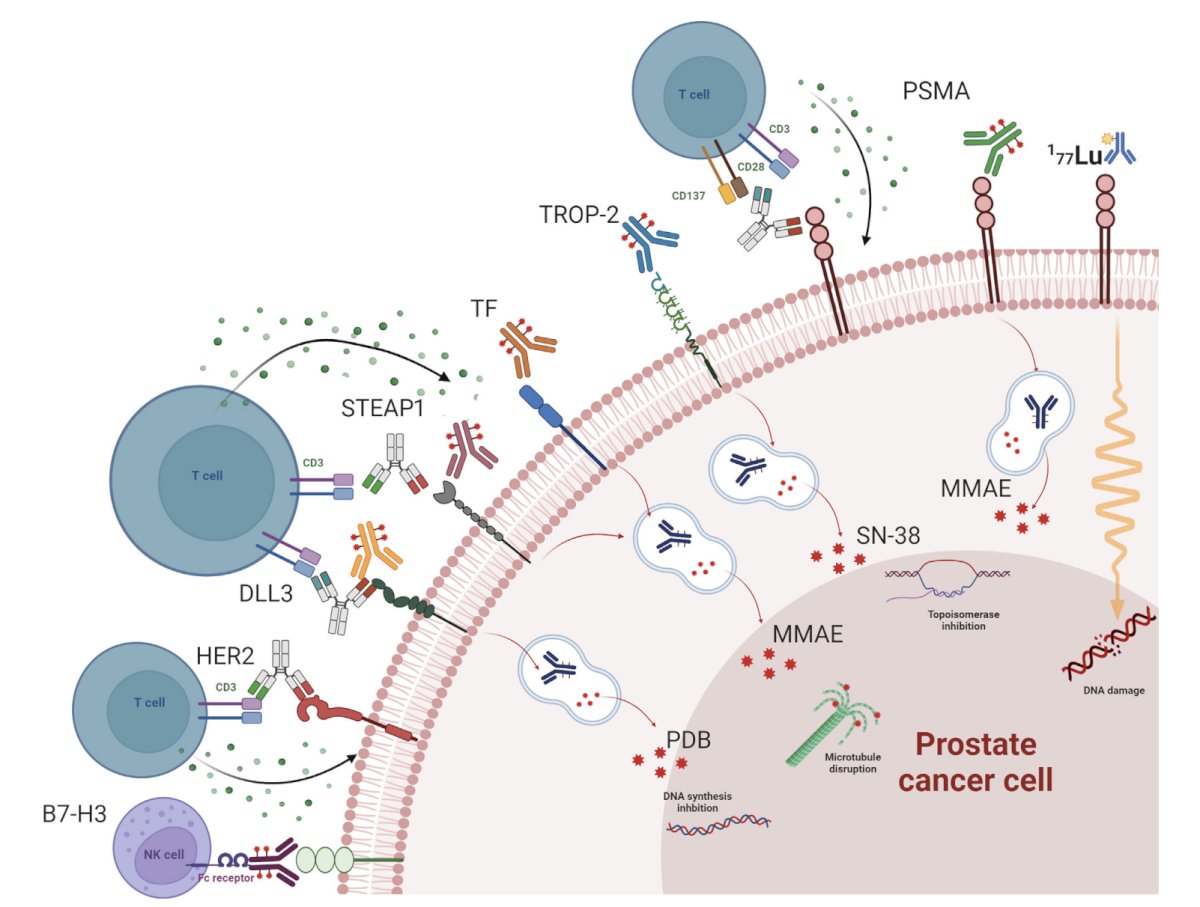
T-cell engagers have increasing IMP complexity, including (i) altered CD3 affinity (leading to decreased cytokine release syndrome), (ii) albumin binding (increasing half life), (iii) other t-cell targets (ie. CD137), (iv) bi-specific versus multi-specific (3/4) to increase specificity/decrease toxicity, (v) mask antigen binding sites to decrease cytokine release syndrome (enzymatic activation in tumors), and (vi) NK cell targets (or immune cell engagers). In prostate cancer, T-cell engagers may target:
- PSMA
- STEAP-1
- KLK2
- B7-H3
- DLL3
- Many others
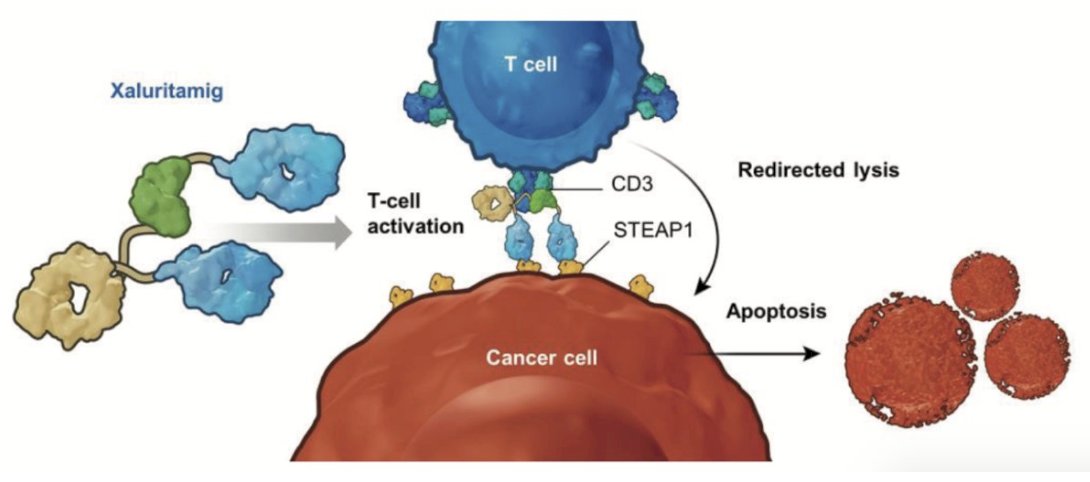
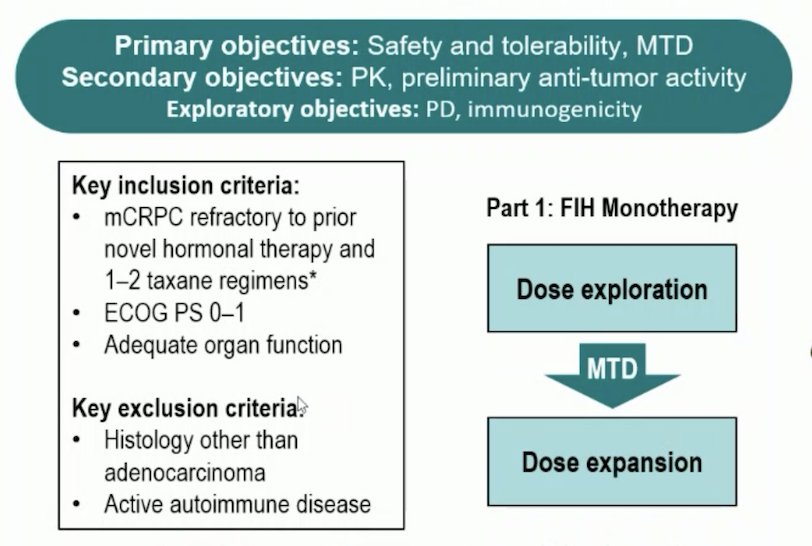
At ESMO 2024, Dr. William Kelly presented the initial results from a dose expansion cohorts in a phase 1 study exploring Xaluritamig, a STEAP1 x CD3 XmAb 2+1 immunotherapy, in patients with mCRPC. STEAP1 is a cell surface antigen highly expressed in prostate cancer, strongly expressed in >80% of mCRPC with bone or lymph node involvement, and often associated with poor survival. Xaluritamig is a novel bispecific XmAb 2+1 T-cell engager targeting STEAP1 and designed to facilitate T-cell–mediated lysis of STEAP1-expressing cells, such as prostate cancer cells:
Eligible patients had mCRPC that was refractory to prior novel hormonal therapy and 1–2 taxane regimens, with an ECOG performance status of 0–1 and adequate organ function. Patients were randomized 1:1:1 to receive IV xaluritamig monotherapy with target dosing regimens of 0.75 mg weekly, 1.5 mg weekly, or 1.5 mg every two weeks, utilizing a 2- or 3-step dosing approach during Cycle 1:
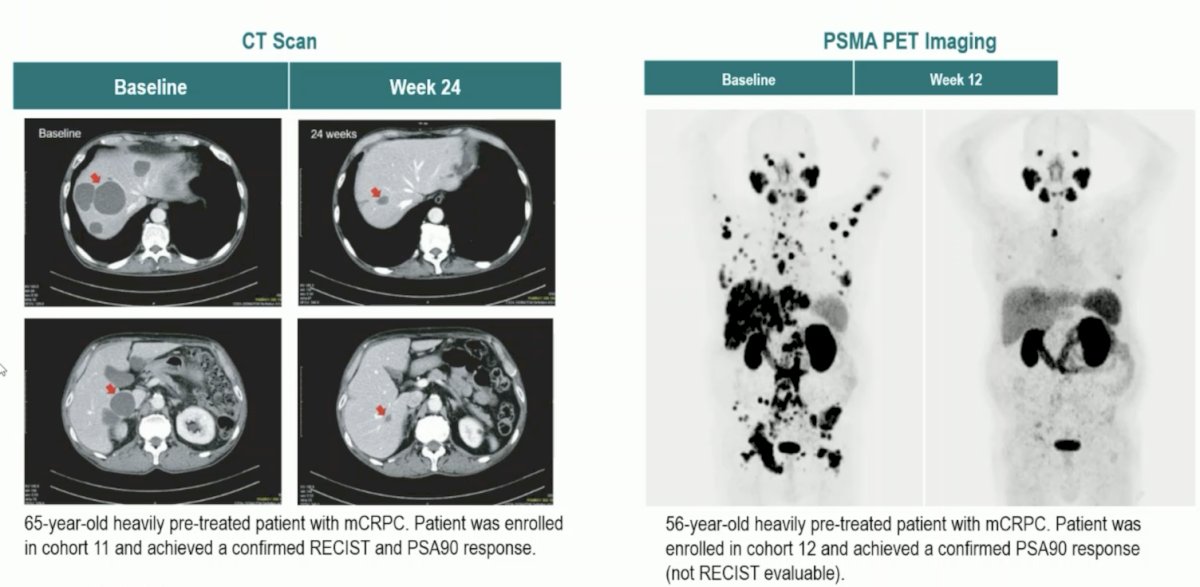
Ultimately, 49% of patients had a PSA50 and 28% had a PSA90 response. Overall, partial response was noted in 24% of patients, but up to 41% of patients in the high dose cohorts. These results correlated with improvement in CT scans and PSMA PET imaging:
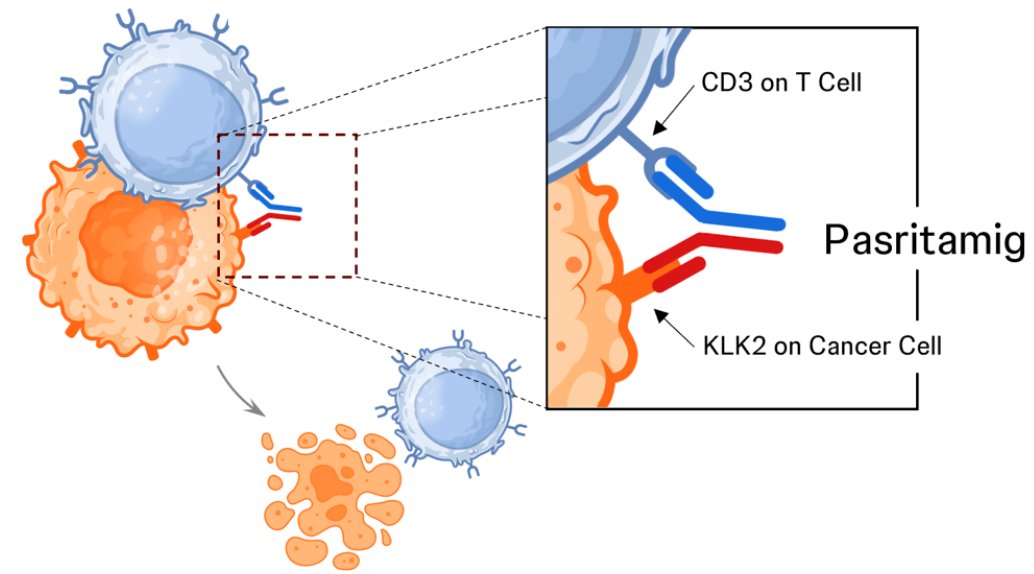
At ASCO 2025, Dr. Capucine Baldini presented phase 1 results of JNJ-78278343 (pasritamig - a first-in-class T-cell-redirecting bispecific antibody targeting human kallikrein 2) in mCRPC, targeting KLK2, a novel target expressed on prostate cancer cells with limited normal tissue expression. Pasritamig simultaneously binds KLK2 on prostate cancer cells and CD3 receptor complexes on T cells, leading to T-cell activation and subsequent lysis of cancer cells:
Pasritamig target doses were escalated from 0.5-2000 mg SC and 150-900 mg IV QW-Q6W, with various step-up dosing schedules. Pre-medication with dexamethasone (16 mg) was required in step-up and first target dose. The primary objective was to determine the safety and the recommended phase 2 dose, whereas secondary objectives included preliminary assessment of antitumor activity:
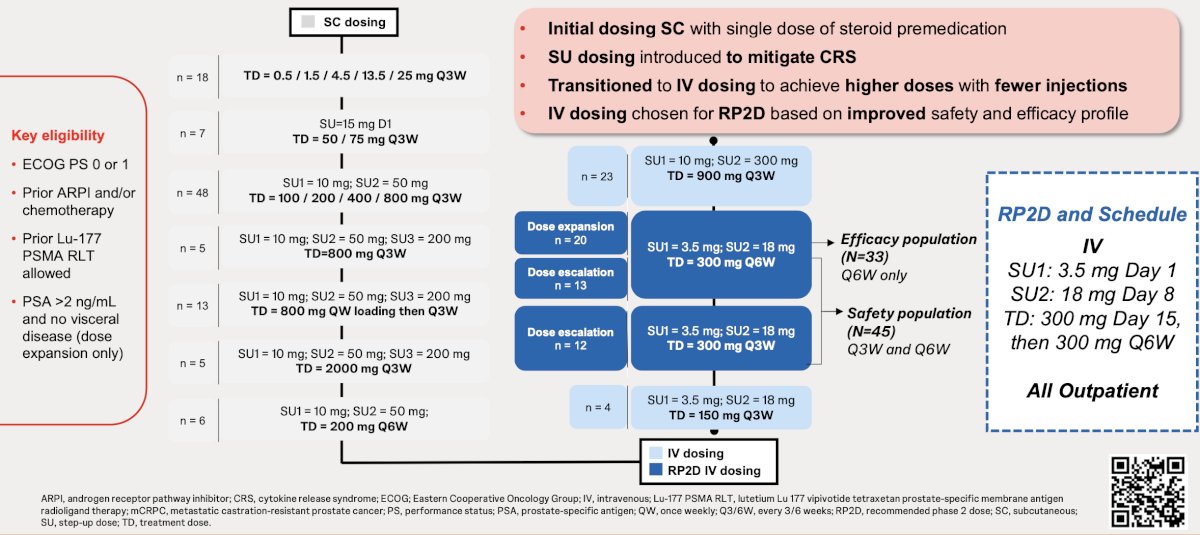
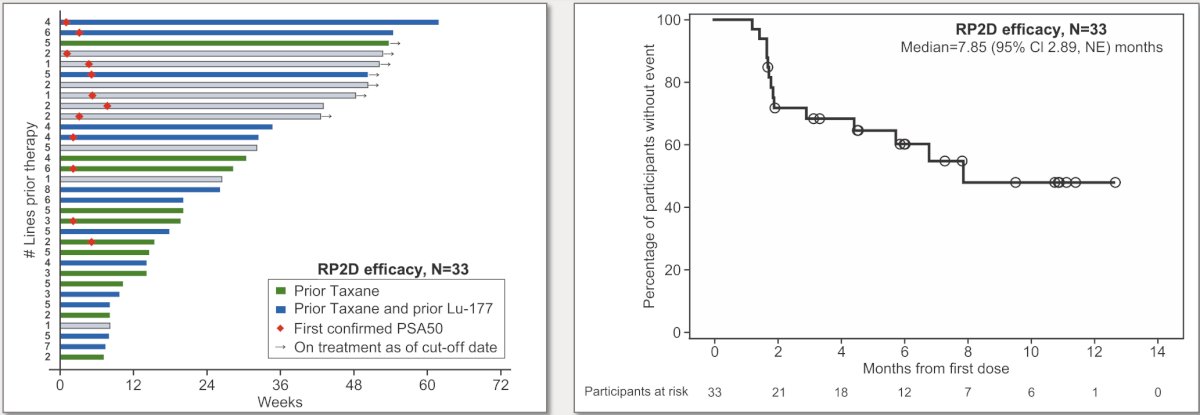
In the recommended phase 2 dose efficacy population (n = 33; 3.5 mg [Day 1], 18 mg [Day 8], 300 mg Q6W IV), PSA50 was 42.4% (14/33):
![In the recommended phase 2 dose efficacy population (n = 33; 3.5 mg [Day 1], 18 mg [Day 8], 300 mg Q6W IV), PSA50 was 42.4% (14/33):](/images/com-doc-importer/232-esmo-2025/esmo-2025-emerging-new-therapeutic-strategies-for-advanced-prostate-cancer/image-10.jpg)
The objective response rate in the 84 patients with measurable disease was 8.3% and the median duration of response of 8.9 (95% CI 3.6, NE) months. In the recommended phase 2 dose efficacy population, the median radiographic progression free survival was 7.9 (95% CI 2.9, NE) months, with 21.2% of patients with treatment ongoing. PSA50 responses and durable disease control were observed irrespective of prior treatment with taxanes or PSMA targeted radioligand therapy:
With regards to radiopharmaceuticals, Dr. De Bono notes that there are likely targets beyond PSMA, as well as other isotopes such as metals (ie. Pb), alpha emitters, beta emitters, or perhaps both. For antibody drug conjugates, tumor-associated target drives selective tumor cell kill, sparing normal cells. The linker biology must limit payload release distant to tumor cells, and multiple molecule payload loading can increase therapeutic index. However, payload selection is key:
- Tubulin binding drugs post-taxanes have limited efficacy
- DNA targeting payloads may have cross-resistance with radiopharmaceuticals, PARP inhibitors, and other DNA damaging drugs
- Senolytic payloads are needed
Dr. De Bono concluded his presentation discussing emerging new therapeutic strategies for advanced prostate cancer with the following take home points:
- There are many new therapeutic strategies under evaluation
- We will likely see many new approvals over the next decade
- Treatment cross-resistance is a concern
- Treatment induced morbidity must also be considered
- Therapy sequencing studies are required
- We may start curing advanced prostate cancer
Presented by: Johann S. De Bono, Royal Marsden NHS Foundation Trust, Sutton, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
References: