(UroToday.com) The 2025 ESMO annual meeting featured a prostate cancer session and a presentation by Dr. Barak Talmor discussing de-escalation therapy in metastatic prostate cancer. ADT combined with androgen receptor pathway inhibitors is the standard initial treatment for metastatic prostate cancer. However, continuous treatment until progression leads to significant cumulative toxicities, impacting quality of life and incurring high financial costs. Intermittent therapy is an established strategy to mitigate treatment burden. This study presented at ESMO 2025 aimed to evaluate the clinical outcomes of a planned treatment break (de-escalation) in metastatic prostate cancer with a favorable response to initial therapy.
Dr. Talmor and colleagues retrospectively chart reviewed 350 patients with metastatic prostate cancer treated between 2014-2024 who received ADT + androgen receptor pathway inhibitor ≥12 months followed by a treatment break after a favorable response which was assessed holistically considering PSA decline, clinical improvement and/or PSMA PET/CT response per EAU/EANM criteria. There was no predefined PSA percentage decline or absolute PET response cut-off required. Upon disease progression, patients were offered re-challenge with the same systemic therapy, surveillance, or metastasis-directed radiotherapy. Disease progression was defined by clinical deterioration, PSA increase on ≥2 subsequent measurements, and/or new PSMA PET/CT lesions. The primary endpoint was treatment free survival, defined from treatment break start to disease progression. All patients had a minimum treatment-free follow-up period of ≥ 6 months.
Overall, 60 men with metastatic prostate cancer were included:
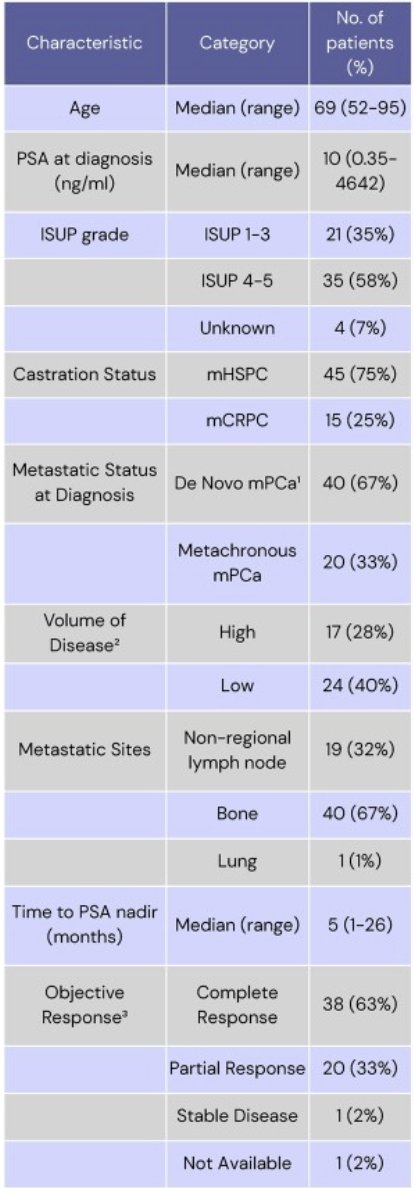
The median duration of ADT + androgen receptor pathway inhibitor therapy at the time of treatment break was 26 months (range: 12-74), and the median treatment free survival was 25 months (95% CI 20.8–28.8):
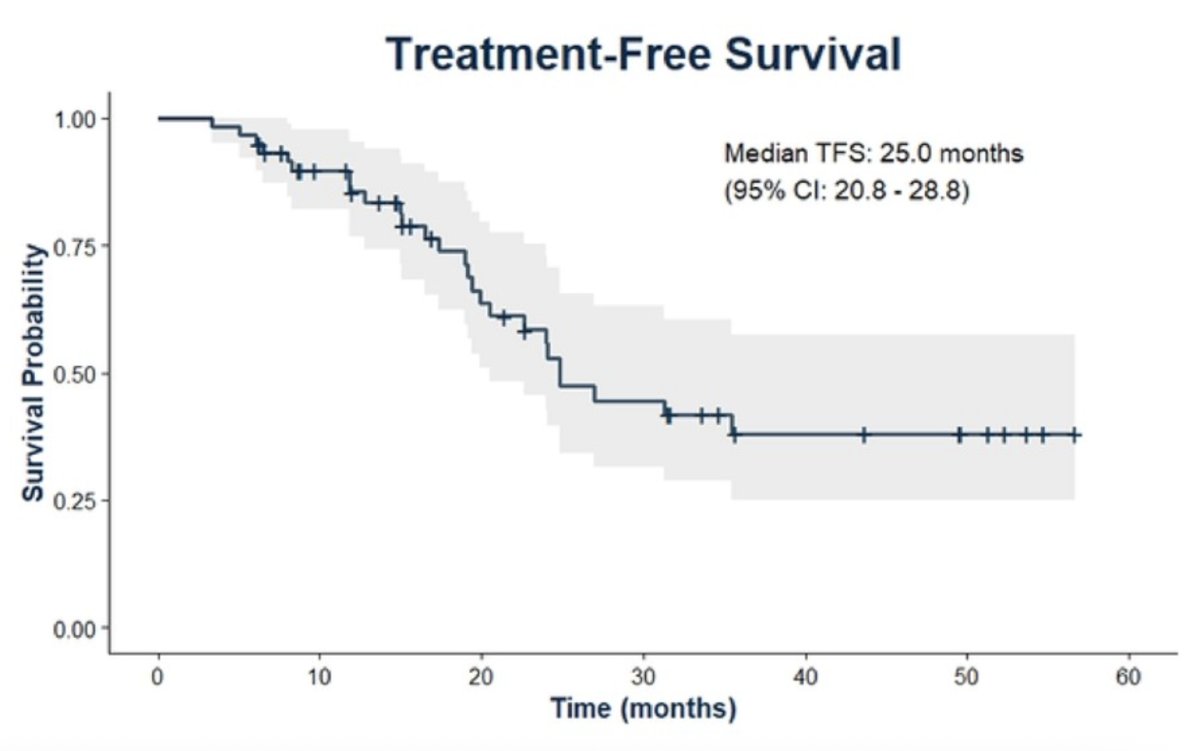
With a median follow-up of 26 months, 43% (26 patients) progressed. Factors significantly associated with longer treatment free survival included:
- Testosterone recovery to normal: 22.5 versus 19 months; HR 0.21, 95% CI 0.062-0.75, p = 0.016
- PSA nadir <8 months: 35 versus 15 months; HR 2.9, 95% CI 1.33-6.45, p = 0.007
- Complete response on PSMA PET/CT: not reached versus 20.5 months for partial response; HR 0.89, 95% CI 0.01-0.767, p = 0.028
- Prior prostate radiotherapy for metastatic prostate cancer: 35 versus 19 months; HR 0.32, 95%CI 0.14-0.73, p = 0.007
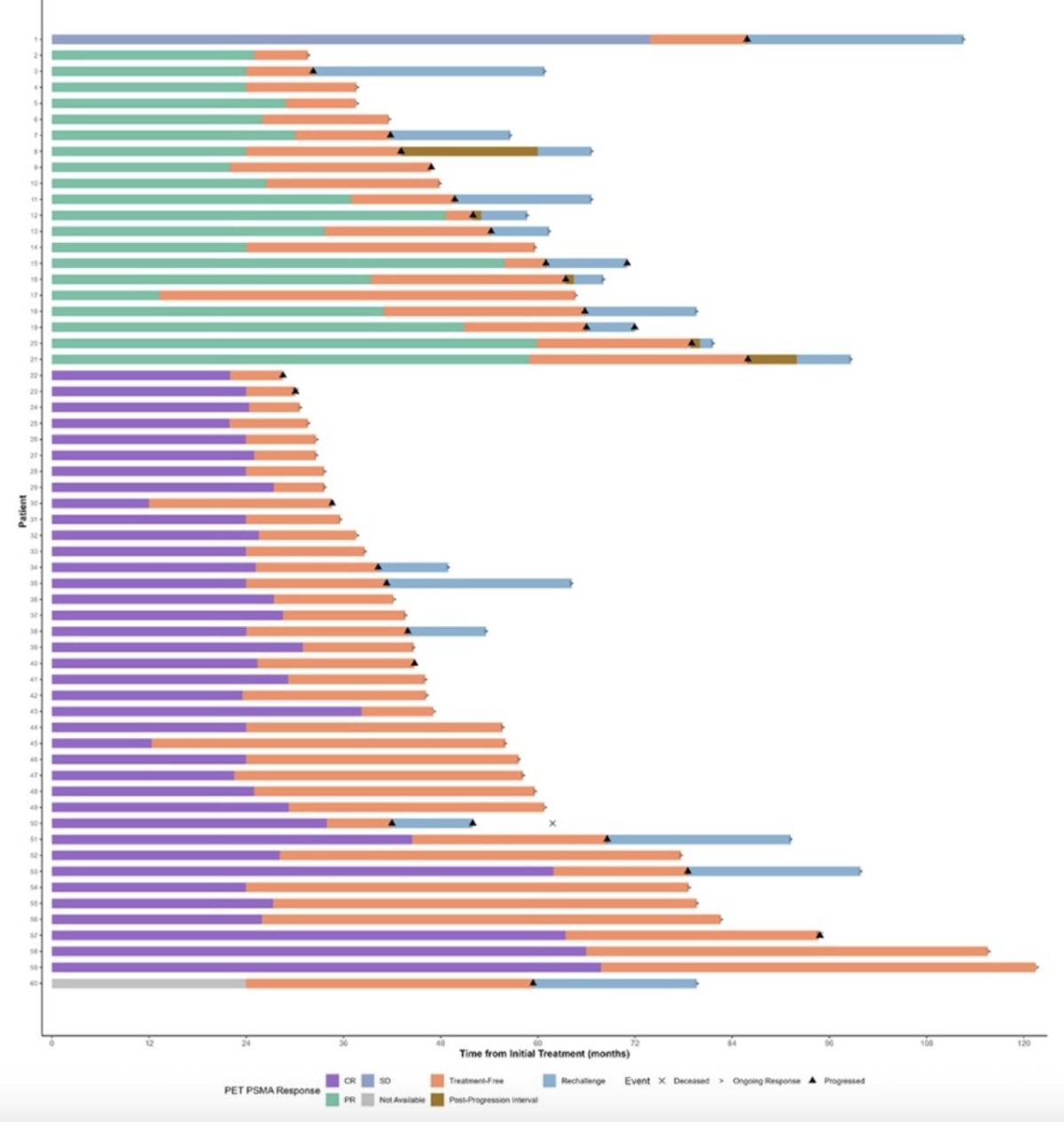
There were 20 patients rechallenged with the same androgen receptor pathway inhibitor regimen, with 95% (19/20) responding, with the median duration of response to rechallenge was 33 months. The Swimmers plot for the patient treatment journey and outcomes is highlighted below:
Dr. Talmor concluded his presentation discussing de-escalation therapy in metastatic prostate cancer with the following take home points:
- Intermittent androgen receptor pathway inhibitor therapy is feasible in selected metastatic prostate cancer patients and could be used to mitigate treatment-related toxicity
- Testosterone recovery, rapid PSA nadir, and complete response on PSMA PET were associated with treatment free survival, but further research is needed to validate predictive markers for patient selection
Presented by: Barak Talmor, The Kinghorn Cancer Centre, St. Vincent’s Hospital Sydney, Darlinghurst, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025