(UroToday.com) The 2025 ESMO annual meeting featured a biomarker-based personalization in metastatic prostate cancer session and a presentation by Dr. Neeraj Agarwal discussing exploitation of homologous recombination alterations across the spectrum disease stages. Over the last decade, it has been established that in advanced prostate cancer, the incidence of DNA repair pathway genetic alterations is ~25%.
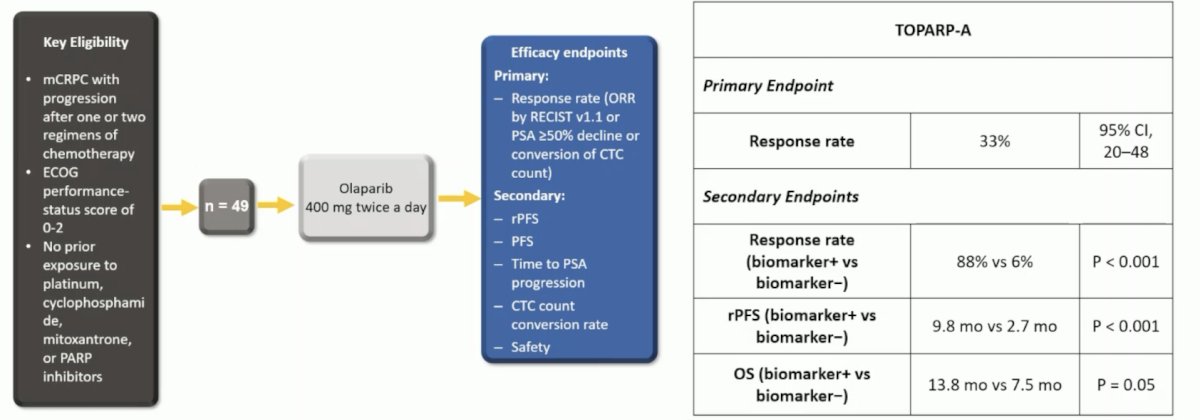
Dr. Agarwal highlighted key data from the PARP inhibitor monotherapy and combination therapy arms throughout this presentation. TOPARP-A was one of the first pivotal phase II trials of olaparib in mCRPC in which 50 patients were treated with olaparib 400 mg twice daily until disease progression.1 The primary endpoint was the composite response rate defined either as an objective response according to RECIST criteria, or PSA50, or a reduction in the CTC count from ≥ 5 per 7.5 ml of blood to < 5 per 7.5 ml. All patients had prior treatment with docetaxel and 49 (98%) with abiraterone or enzalutamide. Sixteen of 49 (33%) evaluable patients had a response. Overall, 14 of the 16 responders had homozygous deletions, deleterious mutations, or both in DNA-repair genes — including BRCA1/2, ATM, Fanconi’s anemia genes, and CHEK2. The response rate was 88% versus 6% for biomarker positive versus negative patients:
Both the PROfound2 and TRITON33 trials were phase III PARP inhibitor monotherapy trials. PROfound was a randomized, open-label, phase III trial of olaparib 300 mg twice daily versus physician’s choice of standard of care therapy in men with HRR-mutated mCRPC who had disease progression while receiving a novel hormonal agent (e.g., enzalutamide or abiraterone). Patients were assigned to one of two cohorts based on their HRR gene alteration. Cohort A included patients with BRCA1, BRCA2, or ATM alterations, irrespective of co-occurring alterations in any other HRR genes. Cohort B had patients with alterations in any of the other 12 HRR genes (BRIP1, BARD1, CDK12, CHEK 1/2, FANCL, PALB2, PPP2R2A, RAD51B, RAD51C, RAD51D, RAD54L). Patients within each cohort were randomized in 2:1 fashion to olaparib versus standard of care. The primary endpoint was the rPFS in cohort A.
TRITON3 was a randomized phase 3 trial of mCRPC patients with a BRCA1, BRCA2, or ATM alterations who experienced disease progression following treatment with a second-generation androgen-receptor pathway inhibitor. Patients underwent 2:1 randomization to receive oral rucaparib (600 mg twice daily) or a physician’s choice control (docetaxel or a second-generation ARPI [abiraterone acetate or enzalutamide]). The primary outcome was the median progression free survival according to independent review. Dr. Agarwal provided the following table emphasizing the results from these two phase 3 monotherapy PARP inhibitor trials:![TRITON3 was a randomized phase 3 trial of mCRPC patients with a BRCA1, BRCA2, or ATM alterations who experienced disease progression following treatment with a second-generation androgen-receptor pathway inhibitor. Patients underwent 2:1 randomization to receive oral rucaparib (600 mg twice daily) or a physician’s choice control (docetaxel or a second-generation ARPI [abiraterone acetate or enzalutamide]). The primary outcome was the median progression free survival according to independent review. Dr. Agarwal provided the following table emphasizing the results from these two phase 3 monotherapy PARP inhibitor trials:](/images/com-doc-importer/232-esmo-2025/esmo-2025-exploiting-homologous-recombination-alteration-across-the-spectrum-disease-stages/image-1.jpg)
Notably, both trials showed a radiographic progression free survival for PARP inhibitor monotherapy, however only PROfound demonstrated an overall survival benefit for olaparib.
There is biological rationale for combining PARP inhibitors with androgen receptor pathway inhibitors. PARP inhibitors disrupt DNA single strand break repair, which leads to double strand breaks, whereas androgen receptor pathway inhibitors suppress androgen receptor activity. Co-inhibition of the androgen receptor and PARP may be efficacious in tumors with or without HRR gene alterations: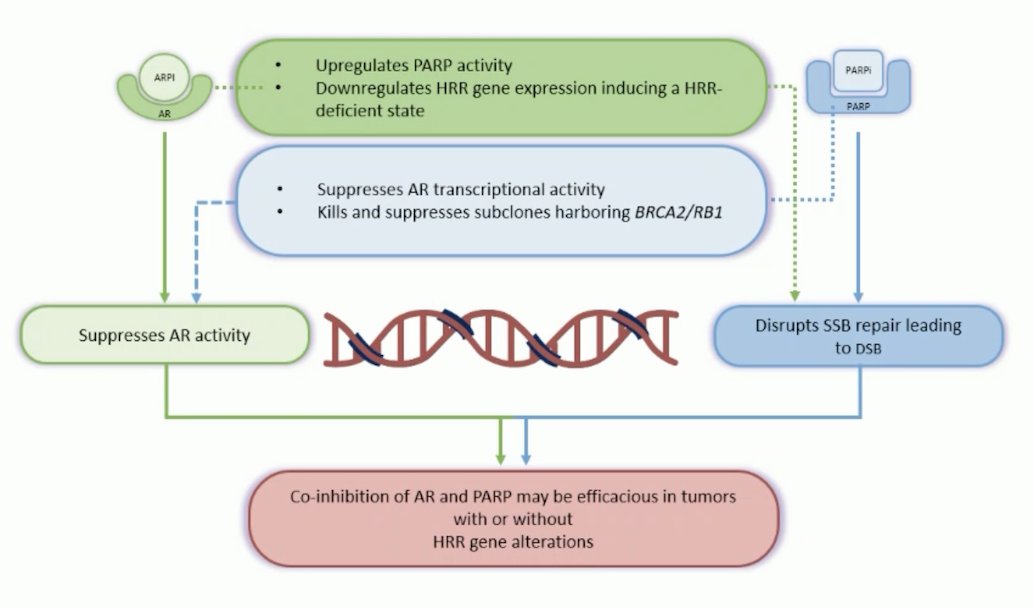
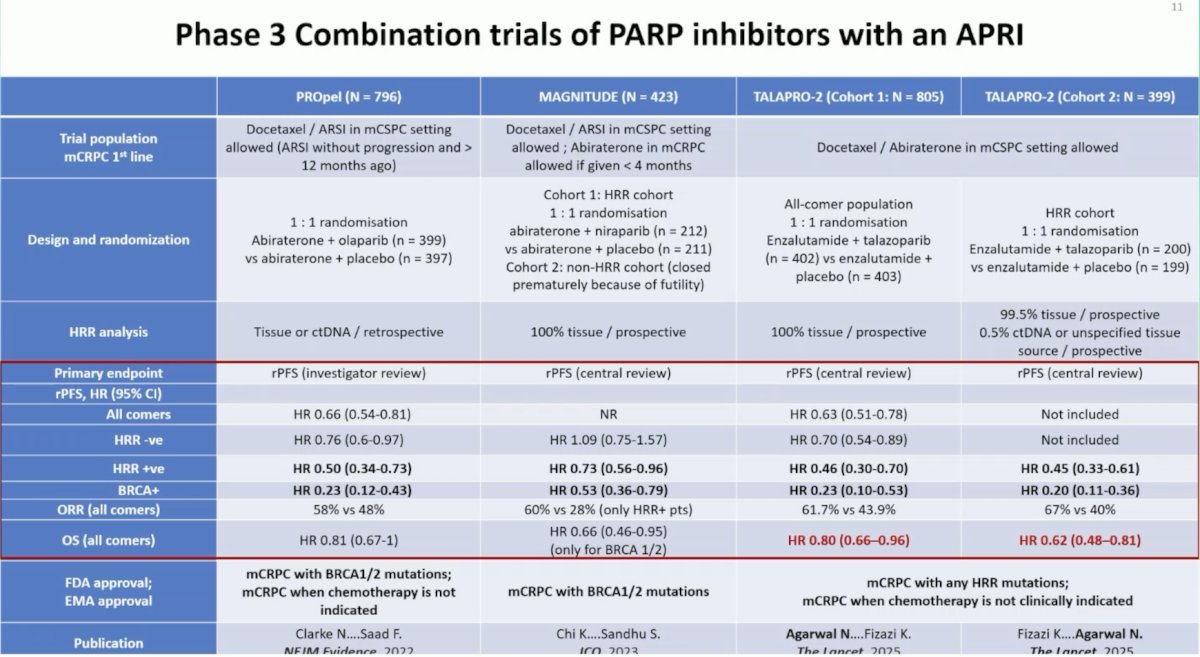
To date, there have been 3 phase III PARP inhibitor + androgen receptor pathway inhibitor trials in mCRPC: PROpel,4 MAGNITUDE,5 and TALAPRO-2.6 PROpel was a global, randomized, double-blind phase 3 trial of abiraterone and olaparib versus abiraterone and placebo in patients with mCRPC treated in the first-line setting. Patients in PROpel were enrolled irrespective of HRR mutational status, which was ascertained via ctDNA or tissue testing. Patients were randomized 1:1 to receive abiraterone (1000 mg once daily) + prednisone/prednisolone with either full dose olaparib (300 mg twice daily) or placebo. The primary end point was imaging-based progression-free survival, by investigator assessment.
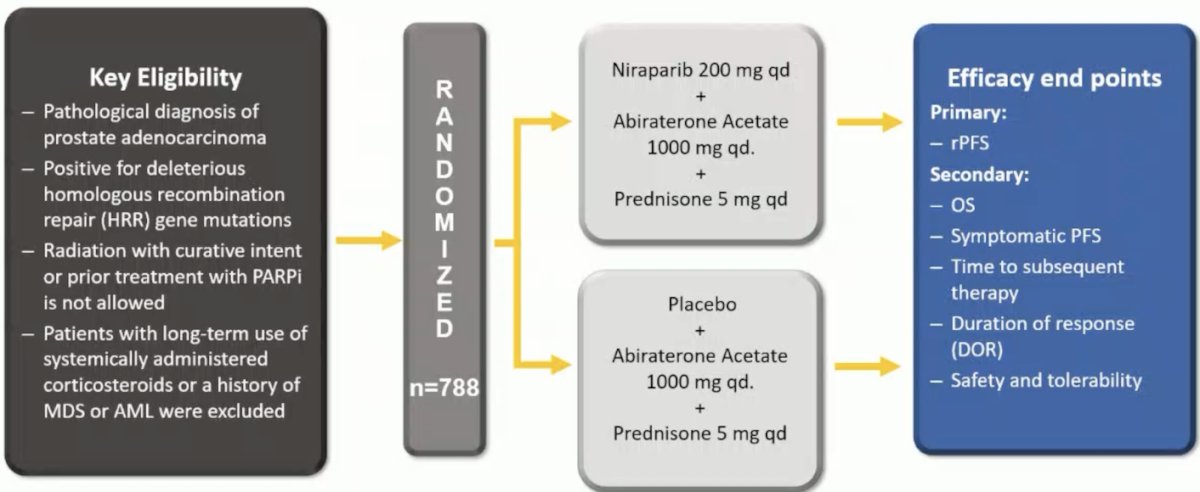
MAGNITUDE was a phase III, randomized, double-blind, placebo-controlled, multicenter trial that evaluated the combination of niraparib + abiraterone acetate + prednisone in mCRPC patients receiving first-line treatment. In contrast to PROpel and TALAPRO-2, this trial included biomarker pre-screened cohorts, meaning that all patients had HRR mutational status determined prior to study enrollment. Patients with a gene alteration (ATM, BRCA1/2, BRIP1, CDK12, CHEK2, FANCA, HDAC2, or PALB2) detected by ≥1 assay were assigned to the HRR+ cohort, whereas those with both assays negative were included in the HRR- cohort. Patients in the HRR+ and HRR- cohorts underwent 1:1 randomization to receive either reduced-dose niraparib 200 mg once daily (usual dose: 400 mg) and abiraterone acetate 1,000 mg once daily plus prednisone 5 mg twice daily or placebo + abiraterone + prednisone.
TALAPRO-2 was a phase III randomized, double-blind, placebo-controlled trial that randomized mCRPC patients 1:1 to talazoparib 0.5 mg once daily (reduced dose from standard of 1 mg) plus enzalutamide 160 mg once daily versus placebo + enzalutamide. Prior use of docetaxel and abiraterone in the mHSPC, but not in the mCRPC setting, was permitted. No prior use of an androgen receptor pathway inhibitor was permitted. Similar to PROpel, this was a biomarker unselected cohort of ‘all comers’. The primary endpoint was radiographic progression free survival, assessed via blinded independent central review, and overall survival was a key secondary endpoint. The following table summarizes the design, HRR analysis, results, and FDA/EMA approval for the 3 trials:
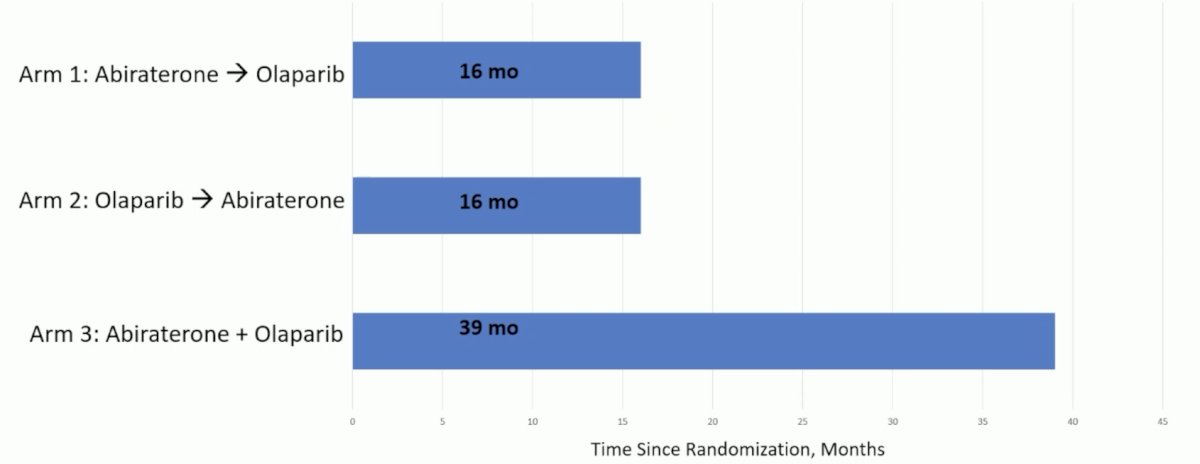
Does sequencing these agents or combining them matter? Dr. Agarwal notes that this was assessed in the BRCAAway trial that randomized mCRPC patients with BRCA1/2 or ATM mutations to abiraterone followed by olaparib versus olaparib followed by abiraterone versus abiraterone + olaparib.7 The median progression free survival from randomization to the end of crossover treatment clearly shows that combination therapy outperformed sequential therapies:
Treatment by specific type of HRR mutation also matters. The table below highlights the gene by gene analysis of radiographic progression free survival in the PROfound and TALAPRO-2 trials, with a clear benefit for PARP inhibitor treatment among patients with BRCA2 mutations, but less efficacy among the rest of the HRR mutations: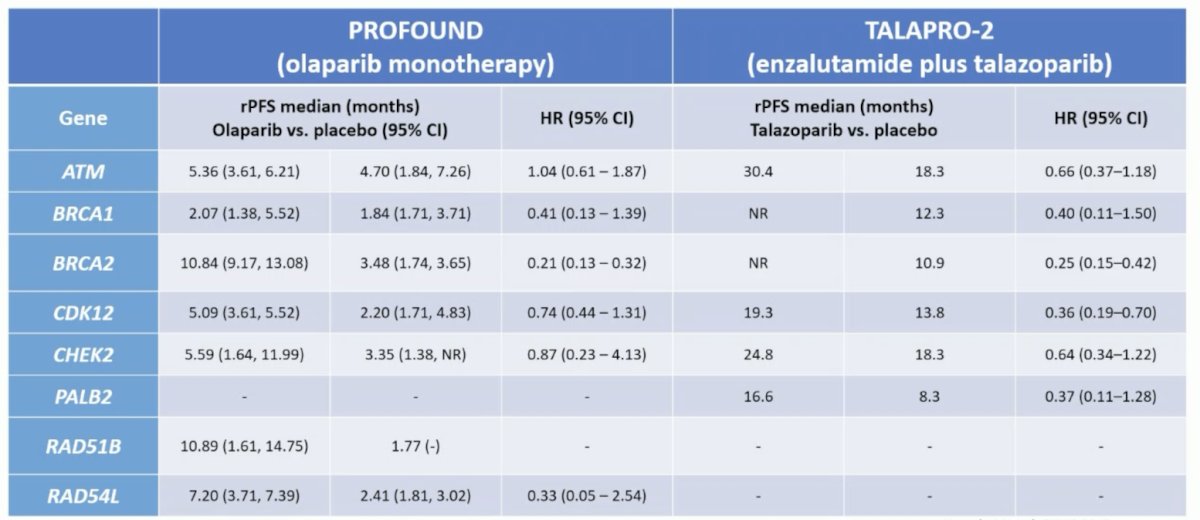
An FDA pooled analysis from 2024 assessed what the impact of PARP inhibitors are for patients with non-BRCA HRR alterations,8 noting that the benefit from PARP inhibitors appeared greatest for patients with BRCA1, BRCA2, CDK12, and PALB2 mutations:
![An FDA pooled analysis from 2024 assessed what the impact of PARP inhibitors are for patients with non-BRCA HRR alterations [8], noting that the benefit from PARP inhibitors appeared greatest for patients with BRCA1, BRCA2, CDK12, and PALB2 mutations:](/images/com-doc-importer/232-esmo-2025/esmo-2025-exploiting-homologous-recombination-alteration-across-the-spectrum-disease-stages/image-6.jpg)
PARP inhibitors and other combinations have also recently been explored, notably olaparib + radium-223 in the COMRADE trial, first presented by Dr. Rana McKay at ASCO 2025:
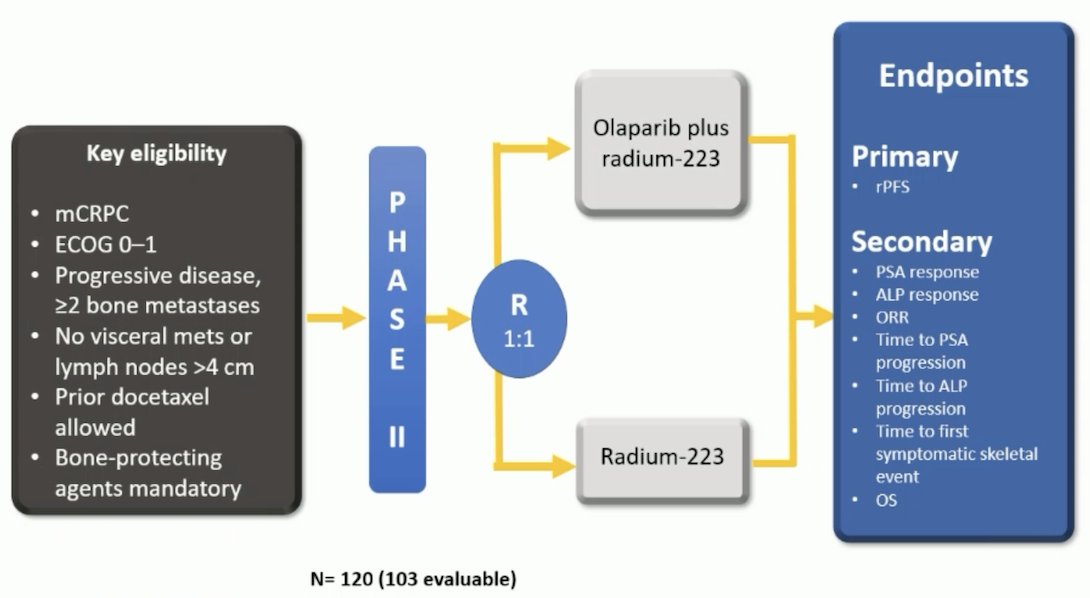
The addition of olaparib to radium-223 significantly prolonged radiographic progression free survival compared to radium-223 alone, with a median of 8.9 months versus 4.7 months, respectively (HR 0.47, 90% CI: 0.34–0.65). Moreover, the combination of olaparib + radium-223 led to a PSA50 response rate of 14.8%, and 39.3% experienced any PSA decline. In comparison, in the radium-223 monotherapy arm, 15.3% of patients achieved a confirmed PSA50 response, and 35.6% had any PSA decline.
The LuPARP phase 1 trial assessed 177Lu-PSMA-617 + increasing doses of olaparib in patients with mCRPC:
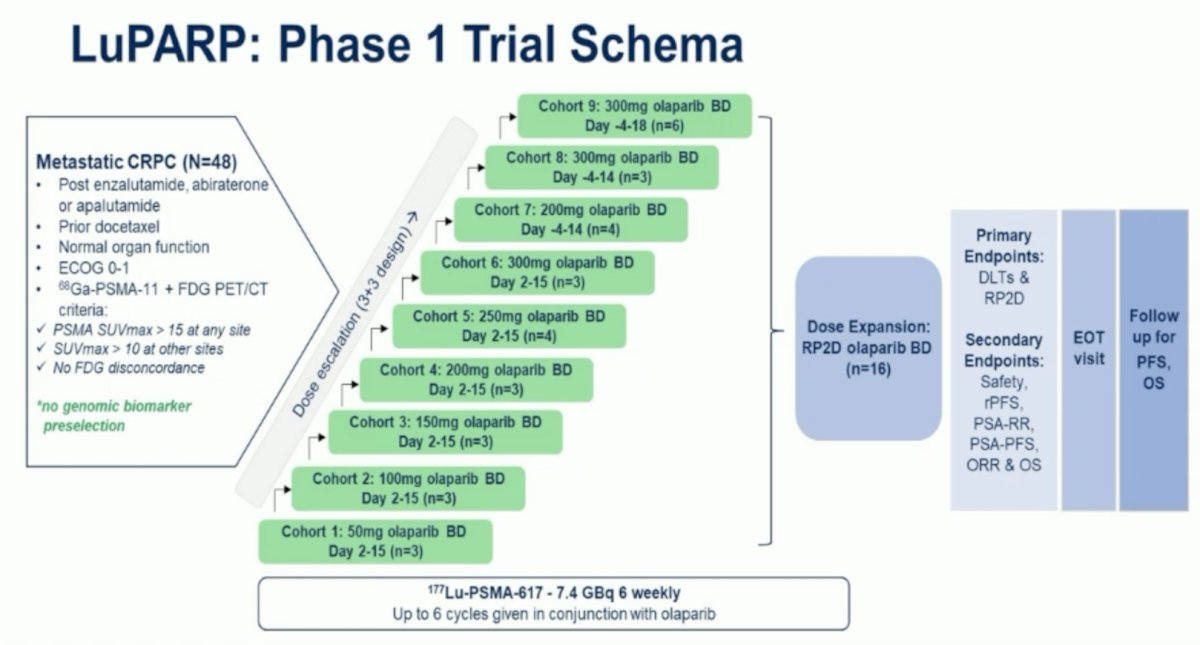
Initial results presented at ASCO 2023 reported a PSA50 response of 66%, PSA90 response of 44%, and an objective response rate of 78%.
Moving to the mHSPC disease space, the AMPLITUDE phase 3 trial assessed niraparib + abiraterone + ADT versus placebo + abiraterone + ADT, with a primary endpoint of rPFS:
Patients had to have at least one HRR mutation in one of the following genes: BRCA1, BRCA2, BRIP1, CDK12, CHEK2, FANCA, PALB2, RAD51B, RAD54L. AMPLITUDE met its primary endpoint, demonstrating that the combination of niraparib + abiraterone significantly reduced the risk of radiographic progression or death by 48% in the BRCA mutated group (HR 0.52, 95% CI, 0.37–0.72) and by 37% in the broader HRR mutated population (HR 0.63, 95% CI, 0.49–0.80). Second, the combination of niraparib + abiraterone also significantly reduced the risk of symptomatic progression by 56% in the BRCA mutated group (HR 0.44, 95% CI, 0.29–0.68) and by 50% in the broader HRR mutated population (HR 0.50, 95% CI, 0.36–0.69). Moreover, the combination was also associated with a 25% reduction in the risk of death in the BRCA mutated group (HR 0.75, 95% CI, 0.51–1.11) and a 21% reduction in the HRR mutated group (HR 0.79, 95% CI, 0.59–1.04), however the overall survival analysis remains immature, as fewer than 50% of the required events have occurred in either group.
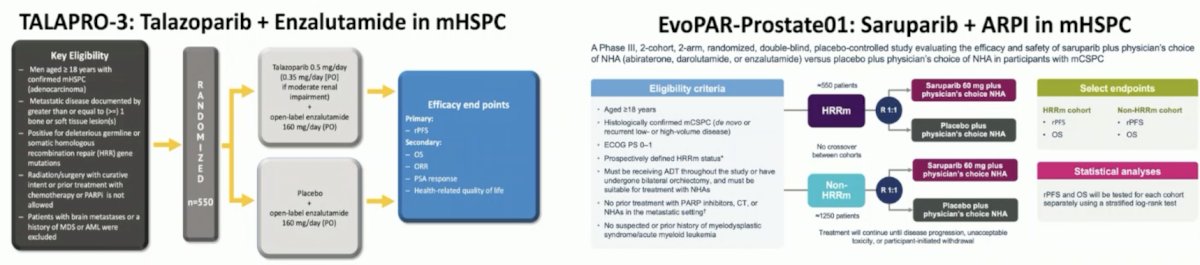
Ongoing PARP inhibitor + androgen receptor pathway inhibitor trials in mHSPC include TALAPRO-3 (talazoparib + enzalutamide) and EvoPAR-Prostate01 (saruparib + androgen receptor pathway inhibitor):
Prior to concluding his presentation, Dr. Agarwal also highlighted two trials even earlier in the prostate cancer landscape. In 2024, Marshall et al. [9] assessed olaparib without androgen deprivation for high-risk biochemically recurrence prostate cancer following prostatectomy among 51 patients. Overall, 13 patients (26%) had a PSA50 response, all within the HRR-positive group (13 of 27 participants [48%]). Additionally, all 11 participants with BRCA2 alterations experienced a PSA50 response:
![Prior to concluding his presentation, Dr. Agarwal also highlighted two trials even earlier in the prostate cancer landscape. In 2024, Marshall et al. [9] assessed olaparib without androgen deprivation for high-risk biochemically recurrence prostate cancer following prostatectomy among 51 patients. Overall, 13 patients (26%) had a PSA50 response, all within the HRR-positive group (13 of 27 participants [48%]). Additionally, all 11 participants with BRCA2 alterations experienced a PSA50 response:](/images/com-doc-importer/232-esmo-2025/esmo-2025-exploiting-homologous-recombination-alteration-across-the-spectrum-disease-stages/image-11.jpg)
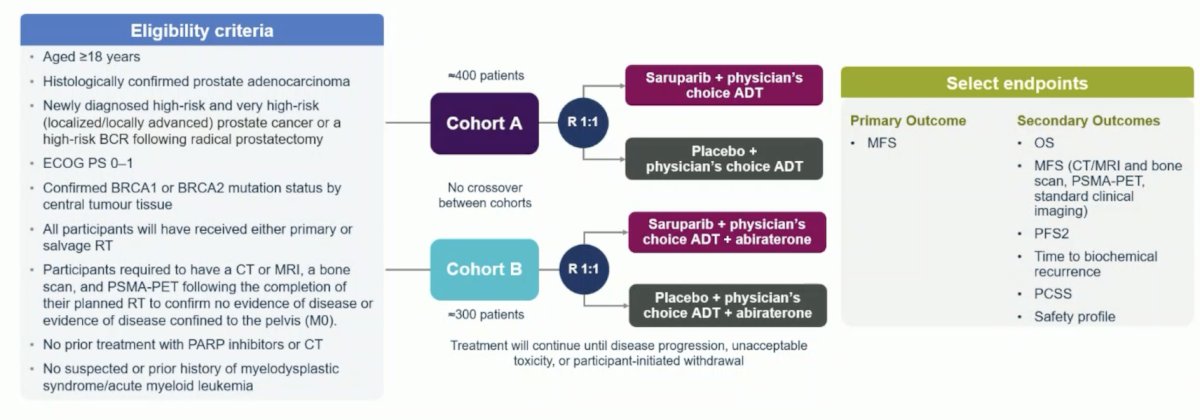
Second, the EvoPAR-PRO2 trial is an ongoing trial assess saruparib + androgen receptor pathway inhibitor in the high risk localized setting, with a primary outcome of metastasis free survival:
Dr. Agarwal concluded his presentation discussing exploitation of homologous recombination alterations across the spectrum disease stages with the following take home points:
- ~25–30% of patients with advanced prostate cancer harbor DNA repair pathway gene alterations making them responsive to PARP inhibitor
- With PARP inhibitor monotherapy, patients with mCRPC with BRCA1/2 altered tumors derive the maximum benefit
- With PARP inhibitors + androgen receptor pathway inhibitor combination therapy in mCRPC, the benefit seems to extend beyond BRCA1/2 to other gene subsets such as CDK12, PALB2, and RAD51. Of note, these trials were not sufficiently powered to assess many individual gene subsets
- Upfront combination therapy may be preferred over sequencing in the mCRPC
- PARP inhibitors may be approved in the mHSPC setting in the near future
- Improved utilization of NGS testing is critical to optimize survival outcomes
Presented by: Neeraj Agarwal, MD, FASCO, Professor, Presidential Endowed Chair of Cancer Research, Director GU Program and the Center of Investigational Therapeutics (CIT), Huntsman Cancer Institute, University of Utah, Salt Lake City, UT
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
References:
- Mateo J, Carreira S, Sandhu S, et al. DNA-repair defects and olaparib in metastatic prostate cancer. N Engl J Med. 2015;373”1697-1708.
- de Bono J, Mateo J, Fizazi K, et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med 2020 May 28;382(22):2091-2102.
- Fizazi K, Piulats JM, Reaume MN, et al. Rucaparib or Physician’s Choice in Metastatic Prostate Cancer. N Engl J Med. 2023 Feb 23;388(8):719-732.
- Saad F, Clarke NW, Oya M, et al. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomized, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108.
- Chi KN, Rathkopf D, Smith MR, et al. Niraparib and abiraterone acetate for metastatic castration-resistant prostate cancer. J Clin Oncol. 2023 Jun 20;41(18):3339-3351.
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): A randomized, placebo-controlled, phase 3 trial. Lancet. 2023 Jul 22;402(10398):291-303.
- Hussain M, Kocherginsky M, Agarwal N, et al. Abiraterone, olaparib, or abiraterone + olaparib in first-line metastatic castration-resistant prostate cancer with DNA repair defects (BRCAAway). Clin Cancer Res. 2024 Oct 1;30(19):4318-4328.
- Fallah J, Xu J, Weinstock C, et al. Efficacy of Poly(ADP-ribose) Polymerase Inhibitors by Individual Genes in Homologous Recombination Repair Gene-Mutated Metastatic Castration-Resistant Prostate Cancer: A US Food and Drug Administration Pooled Analysis. J Clin Oncol. 2024 May 10;42(14):1687-1698.
- Marshall CH, Teply BA, Lu J, et al. Olaparib without androgen deprivation for high-risk biochemically recurrence prostate cancer following prostatectomy: A Nonrandomized controlled trial. JAMA Oncol. 2024 Oct 1;10(10):1400-1408.