(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to a prostate, penile, and testicular cancers proffered paper session. Dr. Elena Castro discussed CAPItello-281, a phase III trial of capivasertib + abiraterone versus placebo + abiraterone in PTEN-deficient patients with de novo metastatic hormone-sensitive prostate cancer (mHSPC), presented earlier by Dr. Karim Fizazi.
Currently, treatment decisions for mHSPC patients are driven by the timing of metastases (de novo versus recurrent) and volume of disease (CHAARTED high vs low volume):

However, this approach does not incorporate biologic/genetic risk factors that are both predictive and prognostic in nature. For example, tumors with SPOP mutations appear to be more susceptible to hormone therapy intensification, whereas those with BRCA, homologous recombination repair (HRR), and PTEN mutations are less likely to respond to hormone therapy intensification regimens.

Notably, it appears that the prevalence of these mutations (i.e., HRR and PTEN/PI3K/AKT) is similar across high- and low-volume mHSPC – as such, simple reliance on disease volume to guide targeted therapy is inaccurate in this setting.

As such, moving towards a biomarker-directed treatment approach is the future in this disease space:

CAPItello-281 is a global, multicenter, randomized, double-blind, phase III trial that included patients meeting the following eligibility criteria:
- De novo mHSPC
- PTEN deficiency: ≤10% of cells expressing PTEN by immunohistochemistry (IHC)
- Of 6,200 patients submitting tumor tissue, 97% had a valid IHC results, and 25% were PTEN deficient
Eligible participants (n=1,012) were randomized 1:1 to:
- Capivasertib (400 mg BID, 4 days on & 3 days off) + abiraterone acetate (1,000 mg daily) + prednisone (5 mg daily) + ADT
- Placebo + abiraterone acetate + prednisone + ADT

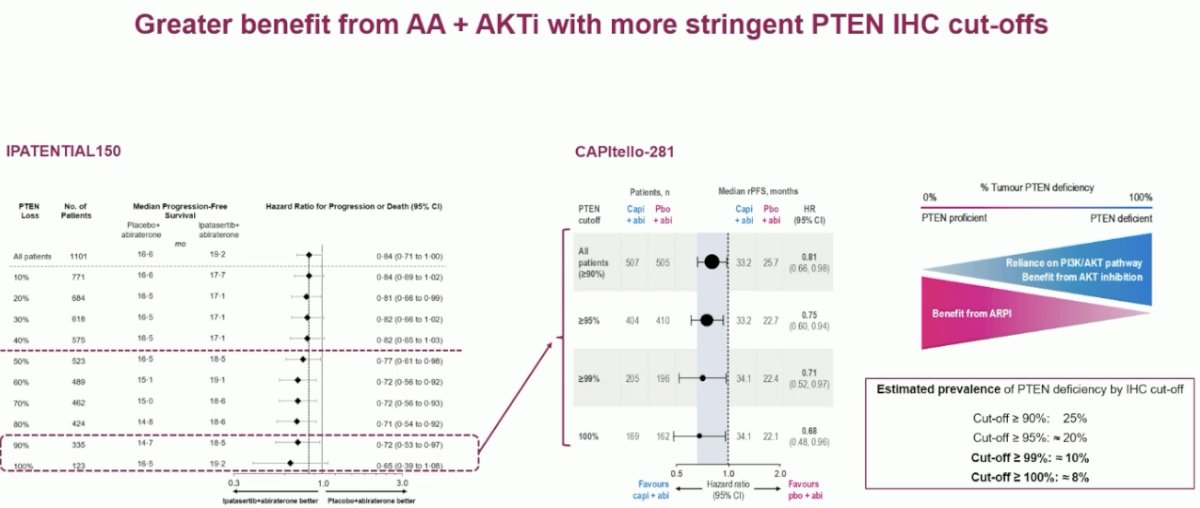
The study met its primary endpoint with capivasertib prolonging rPFS by 7.5 months (median: 33.2 vs 25.7 months; HR: 0.81, 95% CI: 0.66-0.98, p=0.034). However, the median OS of 33.2 months in the capivasertib arm, and especially 25.7 months in the placebo arm, underline the poor prognoses of PTEN-deficient mHSPC. Furthermore, Dr. Castro noted that the magnitude of effect with a HR of 0.81 is lower than what has been observed in other intensification trials.

A number of patients in both treatment arms experienced clinical/radiographic progression prior to experiencing PSA progression, which is a hallmark of PTEN deficient tumors. This emphasizes the importance of routine imaging of such patients in clinical practice and to avoid overreliance on PSA kinetics alone in such patients.

Analysis of OS (data maturity: 26%) demonstrated a weak trends towards a survival benefit (HR: 0.90, 95% CI: 0.71–1.15, p=0.4):

Dr. Castro remarked that the results of this trial mirror those of IPATential150, which was the first phase III trial to evaluate an AKT inhibitor. This trial included 1,101 previously untreated, asymptomatic or minimally symptomatic mCRPC patients with progressive disease. Patients were randomized 1:1 to receive ipatasertib + abiraterone/prednisolone or placebo + abiraterone/prednisolone. In contrast to CAPItello-281, which defined PTEN deficiency by ≥90% loss on IHC, PTEN deficiency was defined by an IHC cut-off of 50% in IPATential150.
Similar to CAPItello-281, the addition of ipatasertib to abiraterone in the IPATential150 trial led to an rPFS benefit (18.5 vs 16.5 months; HR: 0.77, 95% CI: 0.61–0.98), but there was ultimately no overall survival benefit.1

Both trials have demonstrated that the patients most likely to benefit from intensification with an AKT inhibitor are those with complete or near complete PTEN deficiency. However, only 8–10% of advanced prostate cancer patients have ≥99% PTEN loss by IHC, which severely limits the application of these results to real-world practice.
Does it matter if we assess PTEN loss by IHC or next generation sequencing (NGS)? PTEN gene deletion is the primary cause of PTEN deficiency in prostate cancer and usually results in protein loss by IHC. Other causes of PTEN protein loss are less frequent. There is an 86% concordance between IHC and NGS findings.

In the IPATential150 trial, defining PTEN deficiency by NGS was associated with a greater benefit from ipatasertib. Would a similar trend have been observed in the CAPItello-281 trial had NGS been used instead of IHC?

Another issue with the use of PTEN loss as a predictive biomarker is the heterogeneity of IHC PTEN expression in the primary tumor leading to patient misclassification.

With regards to adverse events, the incidence of grade ≥3 adverse events was increased with capivasertib (67% vs 40.4%). Adverse events leading to treatment discontinuation were observed in 18% of capivasertib-treated patients. The most common adverse events in the capivasertib arm were diarrhea (52%), hyperglycemia (38%), and rash (35%). Abiraterone-specific adverse events (i.e., hypertension, hypokalemia) were similar between both arms.

Dr. Castro concluded with the following key take home messages:
- CAPltello-281 confirms the poor prognosis of PTEN deficient mHSPC patients treated with an ARPI and suggests a distinct progression pattern
- Alternative treatment and follow-up strategies are needed for these patients
- Capivasertib in combination with abiraterone is a potential treatment for patients with PTEN deficient mHSPC
- CAPltello-281 met its primary endpoint of rPFS, but the magnitude of the benefit presented may not yet justify a change in practice today
- A robust predictive biomarker is needed
- Further assessment of PTEN IHC ≥99% loss is needed
- Investigation of other biomarkers is also needed with NGS likely to be implemented in clinical practice for HRR assessment
- Adequate tissue sampling is essential for biomarker driven therapy decisions
Presented by: Elena Castro, MD, MS, PhD, Professor, Medical Oncology, Hospital Universitario, Madrid, Spain
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
PTEN Loss in mHSPC: Why It Changes How We Monitor and Treat Patients - Daniel George, Neal Shore, David Morris, & Neeraj Agarwal
PTEN Loss and the Future of Precision Treatment in mHSPC - Karim Fizazi & Noel Clarke