(UroToday.com) The 2025 ESMO annual meeting featured a prostate cancer session and a presentation by Dr. Alicia Morgans discussing the prevalence and severity of hot flashes and their association with PSA response in the initial treatment phase of LIBERTAS, a phase 3 study in metastatic hormone-sensitive prostate cancer (mHSPC).
Apalutamide with continuous ADT showed rapid and deep PSA decline in patients with mHSPC; 38% and 23% of patients treated with apalutamide + ADT achieved a PSA decline of >0.02 to 0.2 ng/mL, and <=0.02 ng/mL by 3 months, respectively, in the TITAN study.1 Hot flashes, an ADT-related side effect, pose a high burden for patients, negatively impacting their quality of life. LIBERTAS, an ongoing ADT de-escalation study, is evaluating apalutamide + intermittent ADT versus apalutamide + continuous ADT in mHSPC patients with deep PSA response after initial treatment (apalutamide + continuous ADT). At the 2025 ESMO annual meeting, Dr. Morgans and colleagues reported PSA and hot flash data for the initial 6-month treatment phase.
LIBERTAS, a prospective, open-label, randomized study, enrolled patients with mHSPC. Patients had metastasis by conventional imaging and/or regional lymph node metastases by next-generation imaging, ≤3 months of ADT pre-enrolment, and ECOG performance status 0 or 1 (2 or 3 if only related to stable physical disabilities). Patients received 6 months of apalutamide (240 mg/d) + continuous ADT, and patients with confirmed PSA <0.2 ng/mL were randomized 1:1 to apalutamide + intermittent ADT or apalutamide + continuous ADT in the main treatment phase:
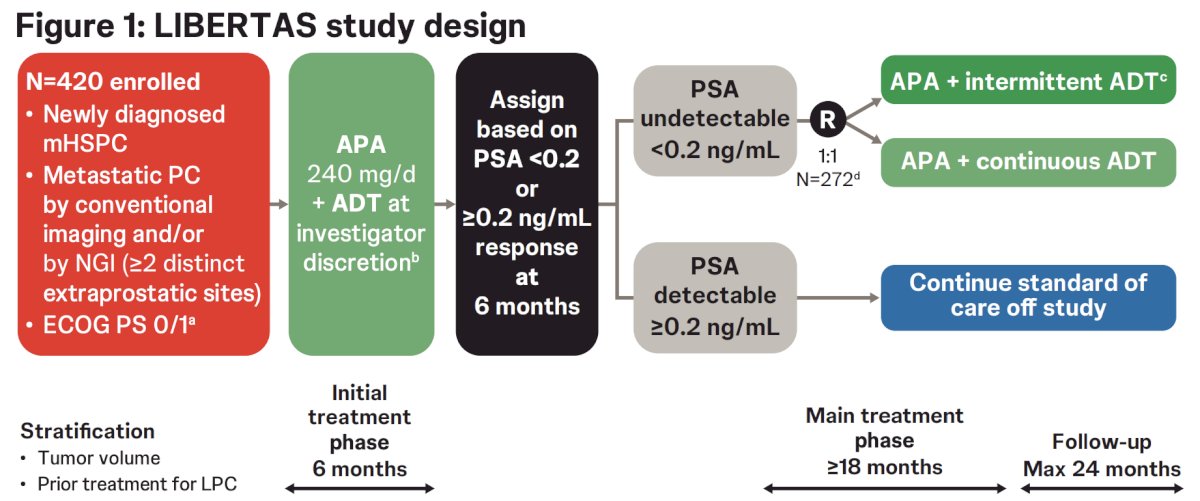
A hot flash diary was collected per protocol across all sites/visits and was completed for 7+ days consecutively prior to cycle 1 day 1 (baseline), cycle 4 day 1 (3 months), and cycle 7 day 1 (6 months) during the initial treatment phase. The primary endpoints are radiographic progression-free survival and hot flash burden reduction after 18 months of apalutamide + intermittent ADT.
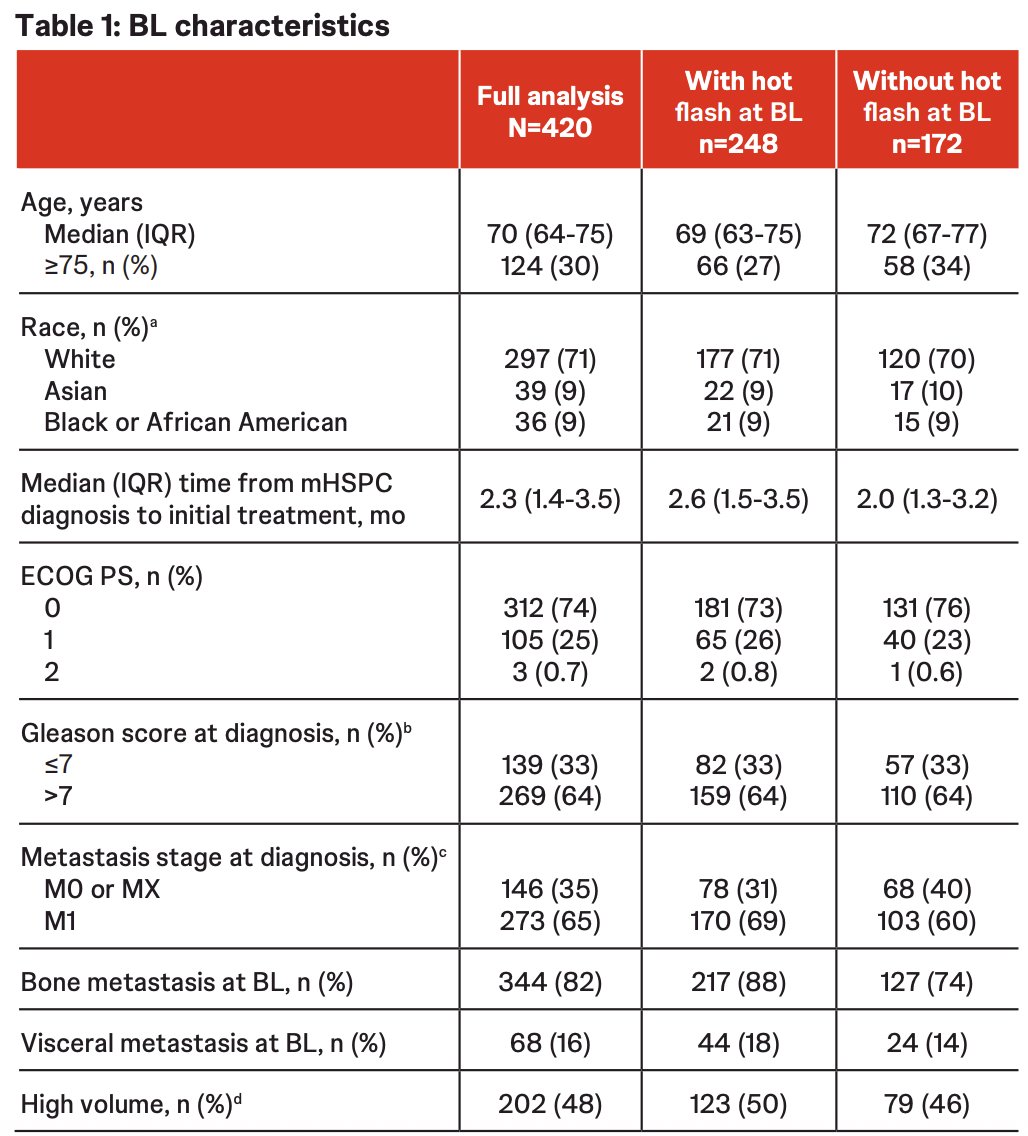
For the initial treatment phase, 420 patients (73 sites, 9 countries) were enrolled in the full analysis set. The baseline median PSA was 7.3 ng/mL, and at baseline, 59% of patients reported hot flashes:
In the full analysis set, pre-study ADT for mHSPC was received by 65% of patients, which was received by more patients with hot flashes at baseline (73%) versus without hot flashes at baseline (54%). The median time from start of pre-study ADT to start of initial study treatment was < 2 months and was similar in patients with and without hot flashes at baseline:
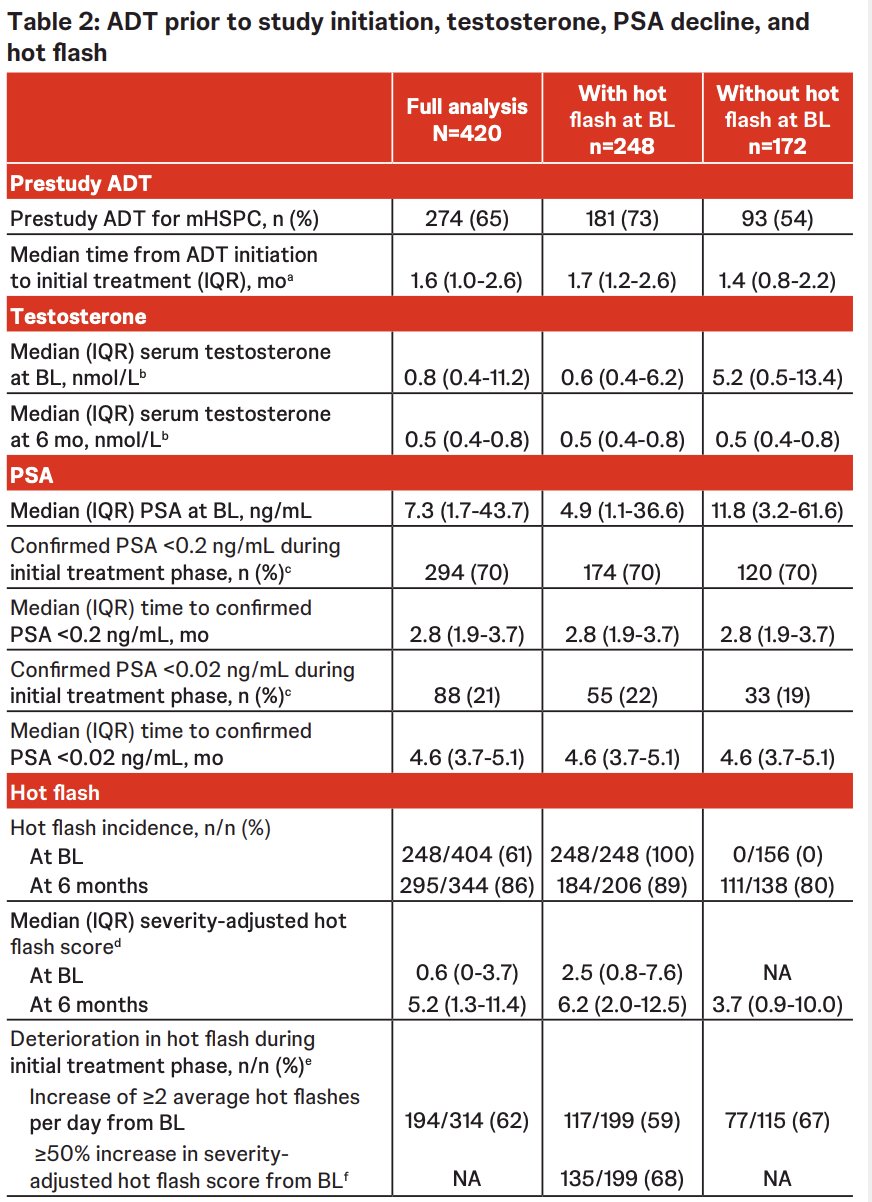
At baseline, median serum testosterone was above castration level in patients without hot flashes at baseline and below in patients with hot flashes at baseline. At 6 months, the median serum testosterone levels were below castration levels regardless of hot flashes at baseline.
More than 2/3 of patients achieved a PSA < 0.2 ng/mL, and the proportion was similar for patients with and without hot flashes at baseline. The median time to achieve PSA <0.2 ng/mL was less than 3 months regardless of hot flashes at baseline. Approximately 1/5 of patients achieved a PSA < 0.02 ng/mL, with a similar proportion for patients with and without hot flashes at baseline.
Hot flash diary was partially or entirely completed by 96%, 93%, and 97% of patients at baseline, 3 months, and 6 months. Hot flash incidence and median severity-adjusted hot flash score increased substantially from baseline to 6 months:
Peak hot flash severity increased from baseline to 6 months: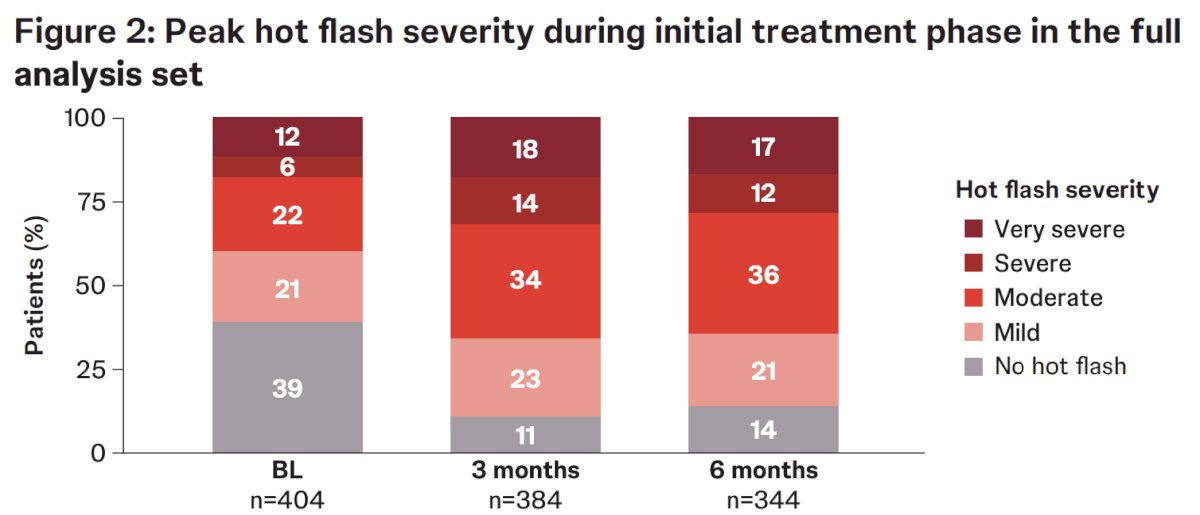
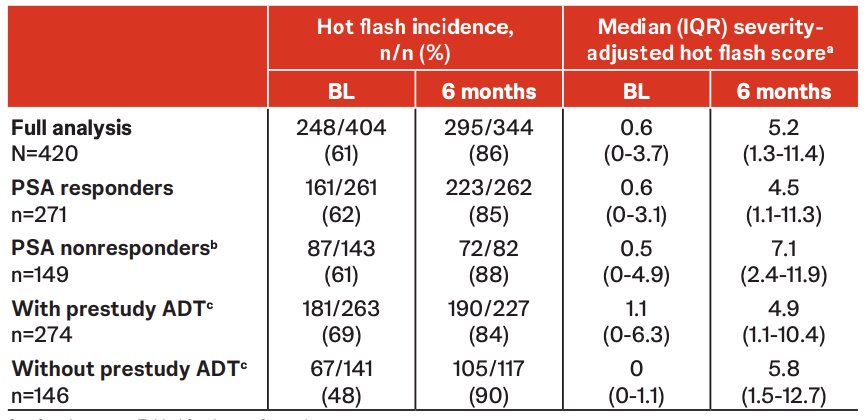
Hot flash incidence and median severity-adjusted hot flash score were similar at baseline and increased from baseline to 6 months, regardless of PSA response. Moreover, the severity-adjusted hot flash score was higher at 6 months in nonresponders versus responders. Patients without pre-study ADT had lower baseline hot flash incidence, peak hot flash severity, and median severity-adjusted hot flash score.
Safety was consistent with prior experience, with the exception of a higher incidence of hot flashes. Hot flash, reported as a treatment-emergent adverse event, occurred in 41% of patients in the full analysis set, of which the majority (84%) were grade 1.
Dr. Morgans concluded her presentation discussing the prevalence and severity of hot flashes and their association with PSA response in the initial treatment phase of LIBERTAS with the following take-home points:
- Patients had a deep and rapid PSA decline with apalutamide + continuous ADT
- Hot flash incidence and overall burden were high and increased from baseline to 6 months during initial treatment with apalutamide + continuous ADT; this increase occurred regardless of PSA response
- Hot flash severity increased more in patients who had not received ADT before the study versus those who did receive pre-study ADT. Further analysis after study unblinding will help to clarify the factors contributing to hot flashes in the main phase of LIBERTAS
- LIBERTAS will explore the de-escalation of ADT in a randomized manner, and the resulting impact on PSA response, clinical outcomes, and quality of life
Presented by: Alicia K. Morgans, MD, MPH, Genitourinary Medical Oncologist, Medical Director of Survivorship Program at Dana-Farber Cancer Institute, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
Reference: