(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to a prostate, penile, and testicular cancers proffered paper session. Dr. Neal Shore presented the overall survival (OS) results from EMBARK, a randomized phase III trial of enzalutamide or placebo plus leuprolide acetate and enzalutamide monotherapy in high-risk biochemically recurrent prostate cancer.
In the phase III EMBARK trial (NCT02319837), both enzalutamide + leuprolide combination therapy (HR: 0.42, p<0.001) and enzalutamide monotherapy (HR: 0.63, p=0.005) significantly improved metastasis-free survival, compared to leuprolide alone, in patients with high-risk biochemically recurrent prostate cancer who were conventional imaging-negative for metastases. Furthermore, both regimens were associated with improved times to PSA progression, first use of new anti-neoplastic therapy, distant metastases, and symptomatic progression.1
Dr. Shore noted that OS was a key, alpha-protected secondary endpoint of EMBARK. At the time of the original analysis and publication, OS data were immature. In this updated report of EMBARK, Dr. Shore presented the final OS, updated secondary endpoints, and long-term safety data for EMBARK patients treated with enzalutamide + leuprolide combination, enzalutamide monotherapy, or leuprolide alone.
The study design is summarized below. In brief, all patients had a PSA ≥1 ng/ml after radical prostatectomy or ≥2 ng/ml above nadir after primary external beam radiotherapy (EBRT), with a PSA doubling time (PSADT) of ≤9 months. Patients had no evidence of metastasis on conventional imaging, and baseline testosterone was ≥150 ng/dL. Hormone therapy ≥9 months prior to enrolment was permitted. Patients underwent stratified randomization to one of three arms:
- Enzalutamide 160 mg (standard dose) + leuprolide acetate (blinded arm)
- Placebo + leuprolide acetate (blinded)
- Enzalutamide monotherapy (unblinded)
PSA was assessed at 36 weeks, and if patients had:
- PSA<0.2 Treatment was suspended at week 37, and PSA monitored with treatment reinitiated if PSA rose again
- PSA>0.2 Treatment was continued

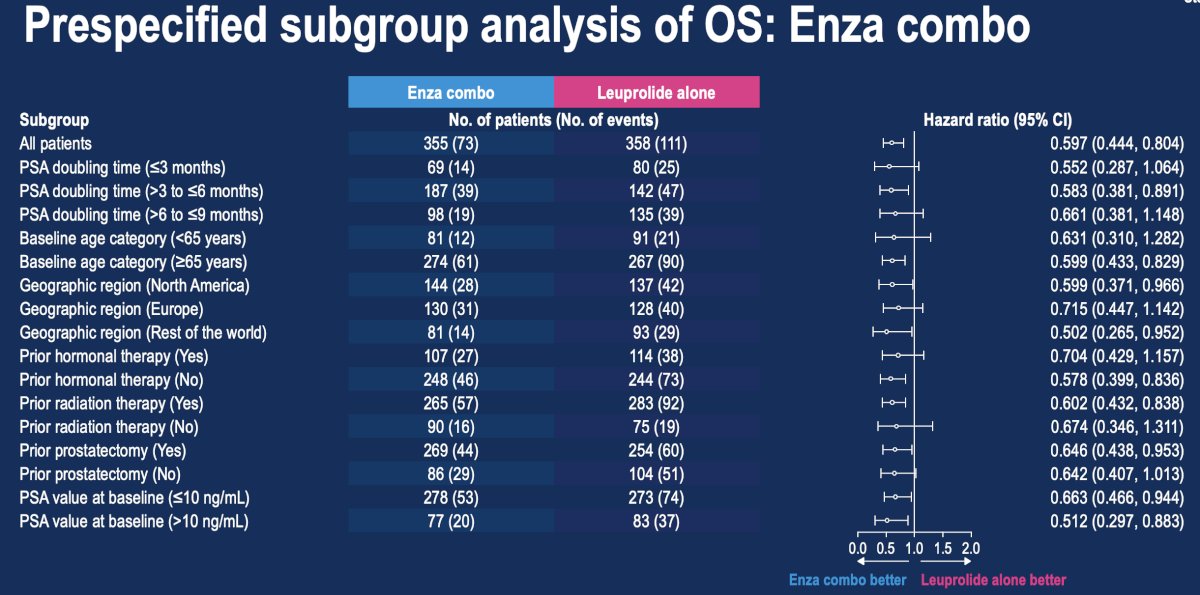
The final OS analysis demonstrated that enzalutamide combination therapy was associated with a 40.3% lower rate of overall deaths, compared with leuprolide alone (8-year OS: 79% versus 69.5%; HR: 0.60, 95% CI: 0.44–0.80, p=0.0006):

A consistent OS benefit was observed across all prespecified subgroups with enzalutamide combination, compared with leuprolide alone.
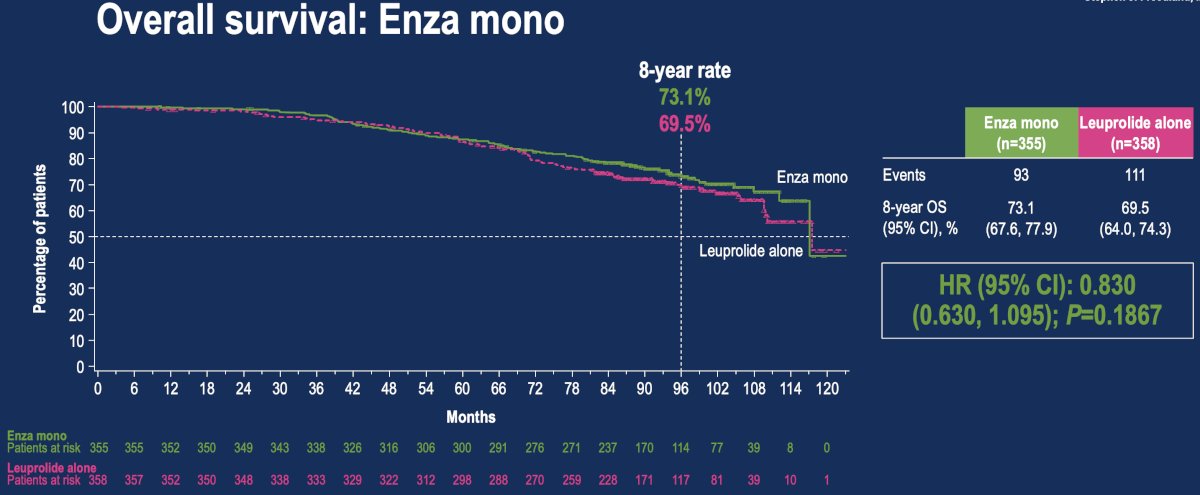
In the comparison of enzalutamide monotherapy to leuprolide alone, the risk of death was 17% lower with enzalutamide monotherapy; however, this did not reach statistical significance (HR: 0.83, 95% CI: 0.63–1.10, p=0.19).
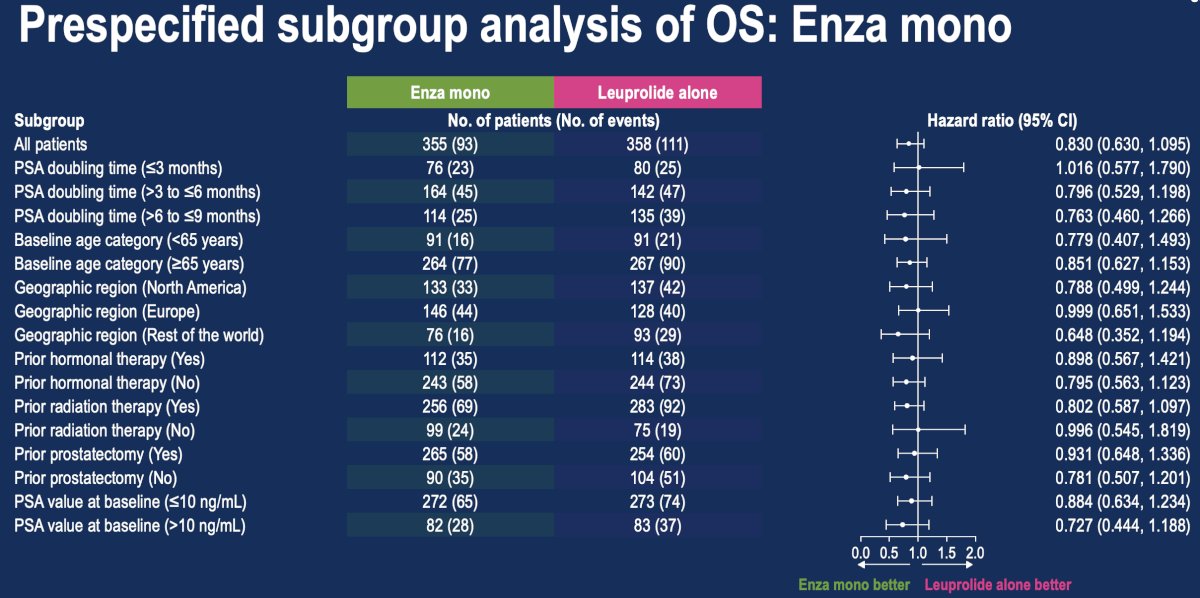
Directionally consistent OS benefits were observed in several prespecified subgroups for enzalutamide monotherapy, compared with leuprolide alone:
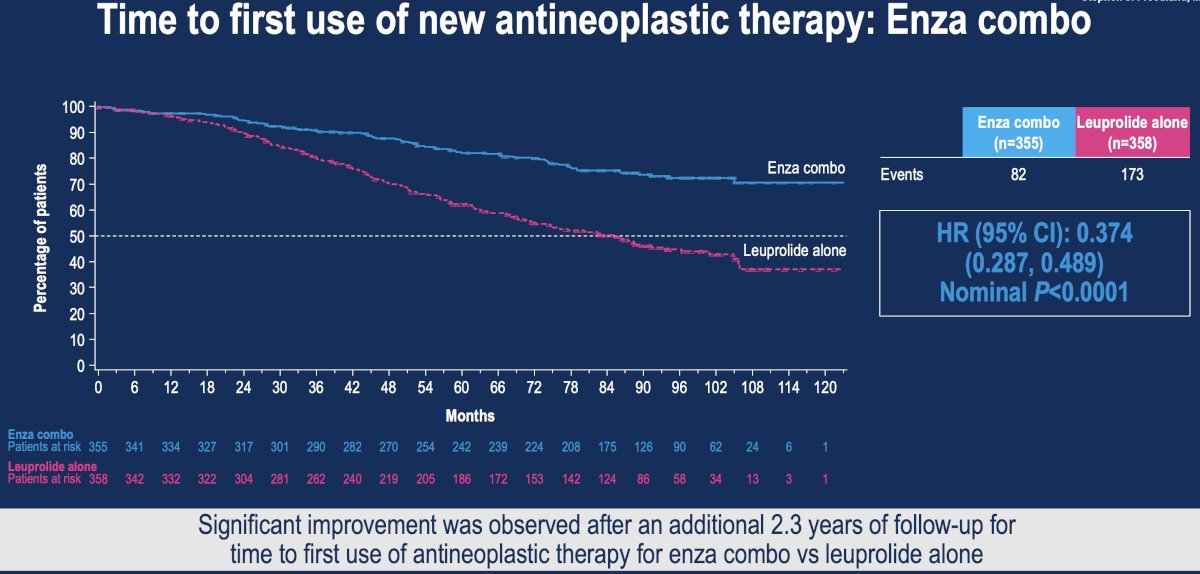
Time to first use of new antineoplastic therapy was significantly prolonged with both enzalutamide combination (HR: 0.37, 95% CI: 0.29–0.49, p<0.0001) and monotherapy (HR: 0.57, 95% CI: 0.45–0.72, p<0.0001):

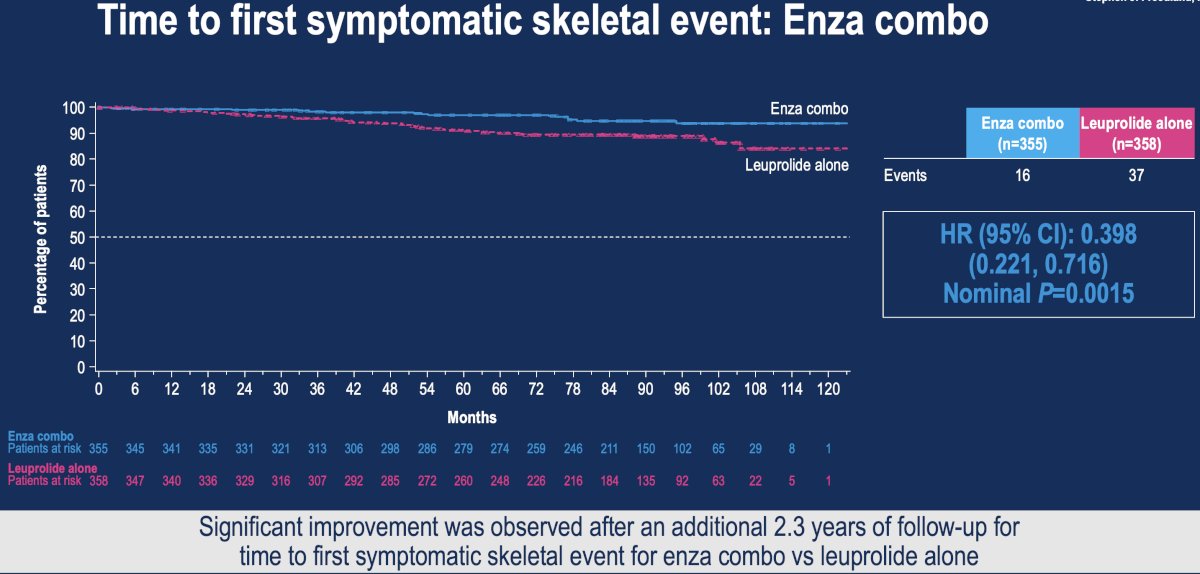
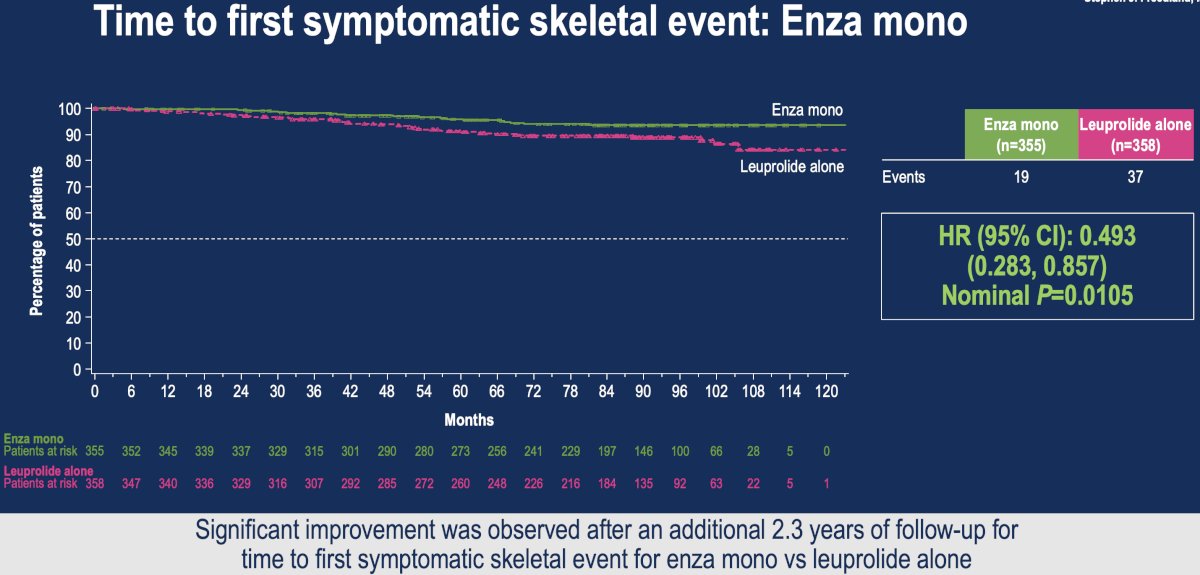
Time to first symptomatic skeletal event was similarly significantly prolonged with both enzalutamide combination (HR: 0.40, 95% CI: 0.22–0.72, p=0.0015) and monotherapy (HR: 0.49, 95% CI: 0.28–0.86, p=0.011):
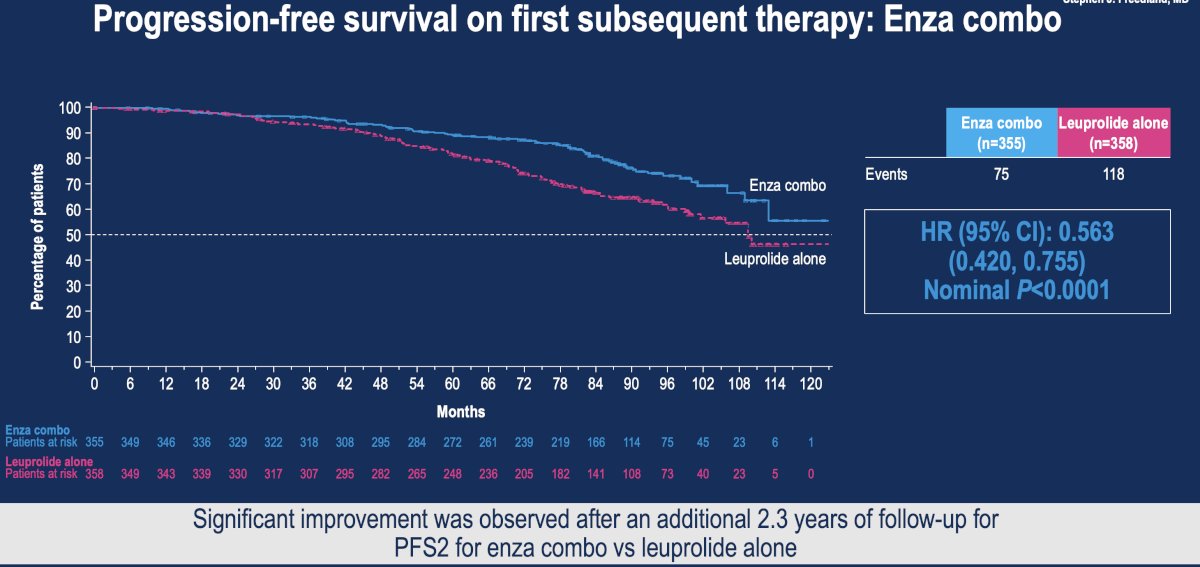
Progression-free survival on first subsequent therapy (i.e., PFS2) was significantly prolonged with both enzalutamide combination (HR: 0.56, 95% CI: 0.42-0.76, p<0.0001) and monotherapy (HR: 0.76, 95% CI: 0.58–1.00, p=0.047):

Safety findings were consistent with the primary analysis:

Dr. Shore concluded as follows:
- Enzalutamide + leuprolide combination reduced the risk of death by more than 40% versus leuprolide alone in patients with high-risk, biochemically recurrent prostate cancer
- Enzalutamide monotherapy led to a numerically lower risk of death versus leuprolide alone, although the difference did not reach statistical significance
- Significant improvements in time to first use of new antineoplastic therapy, time to symptomatic skeletal events, and PFS2 further highlight the benefit of both enzalutamide combination and monotherapy
- No new safety signals were observed in the long-term safety analysis
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Related Content: EMBARK Trial Reports Overall Survival Benefit for Enzalutamide with ADT in High-Risk Non-Metastatic Prostate Cancer - Stephen Freedland
Improved Survival with Enzalutamide in Biochemically Recurrent Prostate Cancer.
References: