(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress, held in Berlin, Germany, between October 17th and 21st was host to the session Radioligand therapeutics. Dr. Jeremie Calais discussed what is next after clinical trials testing PSMA & lutetium-177?
Lu-177–PSMA therapy works by delivering targeted radiation to prostate cancer cells that overexpress PSMA. A radiolabeled ligand binds selectively to PSMA on the tumor surface, allowing the radioisotope Lutetium-177 to emit beta particles that damage cancer cell DNA over several days, with a half-life of 6.6 days. Companion imaging agents such as Gallium-68 or Fluorine-18 PSMA PET scans are used for precise patient selection and real-time monitoring, ensuring accurate targeting and minimal background activity in non-tumor tissues.

Dr. Calais highlighted the evolution of Lu177-PSMA-617 as a landmark in prostate cancer theranostics. The VISION trial, which evaluated LuPSMA versus standard of care in post-chemotherapy mCRPC, demonstrated significant improvements in overall survival and radiographic progression-free survival, leading to FDA approval in 2022. Subsequent studies, such as PSMAfore in pre-chemotherapy mCRPC and PSMAaddition in metastatic hormone-sensitive prostate cancer (mHSPC), have further expanded the therapeutic potential of Lu177-PSMA. These results confirm the role of PSMA-targeted radioligand therapy across the disease continuum, representing a major success in precision oncology and a model for future theranostic development.1-2

Dr. Calais emphasized that the success of Lu177-PSMA-617 in the VISION and PSMAfore trials has paved the way for a new generation of radioligand therapy (RLT) studies across the prostate cancer disease spectrum. Multiple ongoing trials, such as PSMAaddition, SPLASH, ECLIPSE, ARROW, and LUNAR, are now exploring earlier treatment settings, including mHSPC, oligometastatic, and biochemical recurrence states. These studies aim to optimize combinations with ARPIs, PARP inhibitors, and chemotherapy, refine sequencing strategies, and test novel radionuclides and ligands. The expanding PSMA RLT landscape underscores a shift toward precision-guided, biology-driven treatment intensification and is brilliantly summarized in the figure below.

However, despite the success of Lu177-PSMA, there remains substantial room for improvement, as a subset of patients experience limited or no PSA response. Resistance to PSMA-based radioligand therapy may arise from heterogeneous PSMA expression, PSMA-negative disease, tumor microenvironment effects, or failure to deliver an adequate radiation dose to micrometastatic lesions. Strategies to overcome resistance include optimizing patient selection through PSMA PET, ctDNA, and molecular profiling; exploring earlier disease stages; refining sequencing relative to ARPIs or chemotherapy; and personalizing dosing via dosimetry. Combination strategies such as pairing RLT with ARPIs, PARP inhibitors, immunotherapy, or alpha emitters, which are under active investigation and illustrated below.

Dr. Calais continued by discussing ongoing combination strategies aimed at enhancing the efficacy of Lu177-PSMA therapy. He highlighted the ENZA-p trial, which showed a significant overall survival benefit when combining Lu177-PSMA-617 with enzalutamide compared to enzalutamide alone (HR 0.55, 95% CI 0.36–0.84; p=0.0053). (3,4) Approaches combining Lu177-PSMA with AR pathway inhibitors (ARPI) seek to enhance PSMA target expression, as short-term androgen blockade can increase PSMA density and improve radioligand uptake, a concept being explored in trials such as ENZA-p, PSMAcare, and PSMAndARPI.
Another area of active investigation involves dual targeting strategies, including alpha–beta emitter combinations like AcTFirst, designed to overcome heterogeneous PSMA expression and improve tumor control. Finally, combinations with immune checkpoint inhibitors such as pembrolizumab or ipilimumab/nivolumab (PRINCE, EVOLUTION, NEPI) aim to prime or ignite an immune response, leveraging Lu177-PSMA–induced immunogenic cell death to enhance T-cell activity and potentially extend the durability of response. A summary of combination trials is shown in the tables below.

Moreover, Dr. Calais walked the audience through the rapidly expanding landscape of PSMA-targeted radioligand therapies beyond Lu177-PSMA-617. He showcased novel compounds and radionuclides currently in development, including next-generation beta emitters (such as 177Lu-PSMA-R2 and 177Lu-DOTA-TLX591) and alpha emitters (like 225Ac-PSMA-617, 225Ac-PSMA-R2, and 225Ac-PSMA-I&T). These agents vary in their physical properties, tissue penetration, and carrier platforms from antibodies and bispecifics to peptides and nanoparticles, each designed to optimize tumor targeting and minimize off-target toxicity.

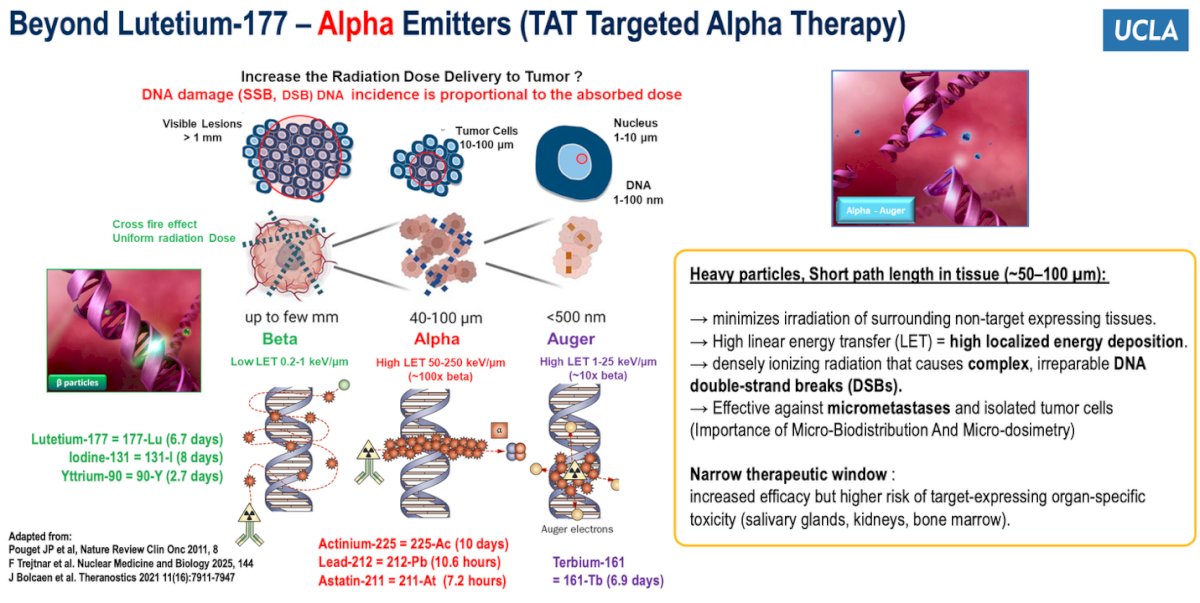
Beyond Lutetium-177, Dr. Calais then reviewed the physical properties of therapeutic radioisotopes used in PSMA-targeted radioligand therapy. Lutetium-177 primarily emits beta particles, which deliver a lower energy deposition distributed across multiple cells, creating a crossfire effect. In contrast, alpha emitters and Auger electrons have a much higher linear energy transfer, 10 to 100 times greater than beta particles, delivering concentrated radiation over a few nanometers, at the level of the cell nucleus. This localized, high-energy deposition induces complex and irreparable DNA double-strand breaks, enhancing the potential to eradicate micrometastatic disease. Preclinical studies have demonstrated that while Lu177-PSMA monotherapy struggles to effectively target microscopic disease, actinium-based alpha emitters or Lu177 combined with AcPSMA achieve more complete tumor control. Importantly, Dr. Calais emphasized that micro-biodistribution and micro-dosimetry are critical determinants of efficacy, particularly for microscopic disease, while also noting the narrower therapeutic window and potential for organ-specific toxicity associated with alpha emitters.
Dr. Calais then delved into the role of actinium-225 (Ac-225) as a next-generation alpha-emitting radionuclide and reviewed the growing number of clinical trials evaluating its use in prostate cancer. Multiple studies, including TATCIST, AlphaBREAK, and PSMACTION, are investigating Ac225-PSMA constructs such as PSMA-617, PSMA-R2, and PSMA-I&T—across various disease settings from heavily pretreated mCRPC to earlier disease states. In advanced mCRPC, early results from retrospective and phase 1/2 experiences have been remarkable, with PSA50 responses reported in up to 57% of patients, median overall survival around 15 months, and median PFS close to 8 months. However, xerostomia remains the main dose-limiting toxicity, observed in approximately 68% of patients. Dr. Calais emphasized that ongoing multicenter trials—including the phase 3 PAnTHA and PSMACTION studies will be critical to defining optimal dosing, sequencing, and combinations to harness the potent cytotoxic potential of Ac-225 while minimizing off-target effects.

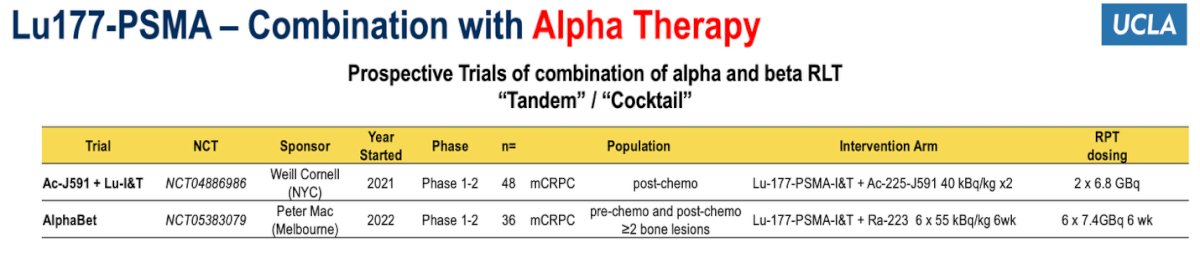
Dr. Calais also discussed emerging “tandem” or “cocktail” approaches combining beta- and alpha-emitting PSMA-targeted radioligand therapies. These strategies aim to balance the broader tissue penetration of beta particles with the highly localized, potent cytotoxicity of alpha emissions. Two key ongoing studies include the Ac-J591 + Lu-I&T trial (Weill Cornell, NCT04886986) in post-chemotherapy mCRPC, and the AlphaBet trial (Peter MacCallum, NCT05383079) testing Lu177-PSMA-I&T with Ra-223 in patients with ≥2 bone lesions, both pre- and post-chemotherapy.
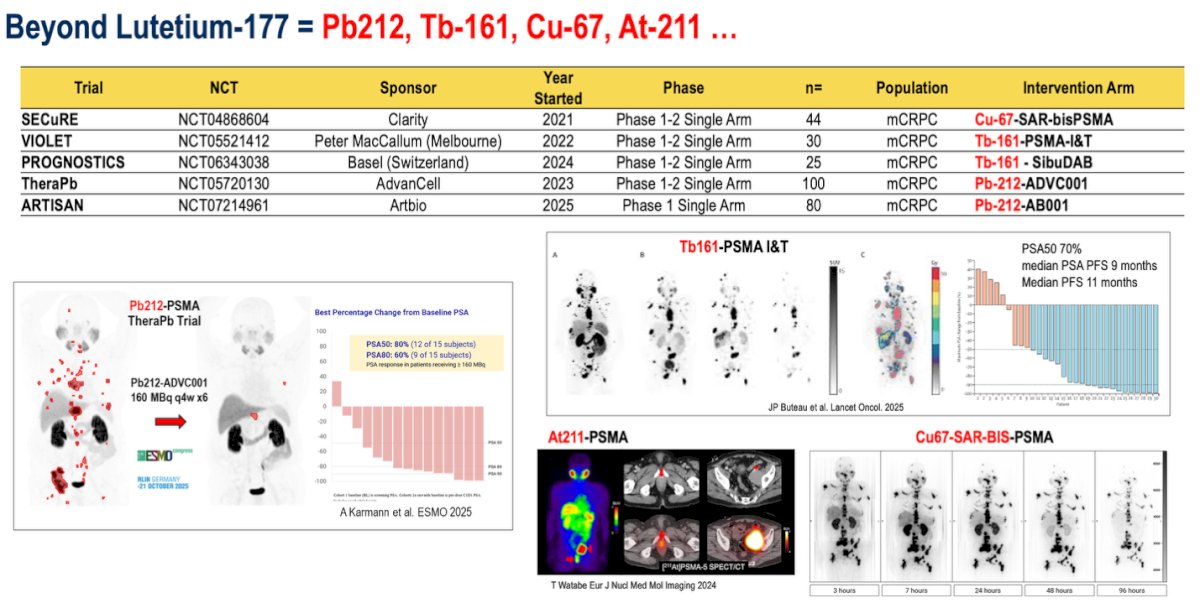
Furthermore, Dr. Calais highlighted that research in targeted radionuclide therapy is rapidly expanding beyond lutetium-177, with several novel isotopes such as lead-212, terbium-161, copper-67, and astatine-211 currently under investigation. These next-generation agents differ in emission properties, potentially improving tumor dose delivery and overcoming resistance seen with beta emitters. Early trials, including SECuRE (Cu67-SAR-bisPSMA), VIOLET and PROGNOSTICS (Tb161-based agents), and TheraPb and ARTISAN (Pb212 constructs), are testing these compounds in mCRPC as illustrated below. Preliminary findings are promising, with the Pb212-PSMA TheraPb study reporting PSA50 responses in 70% of patients and a median PFS of 9–11 months.
Beyond PSMA, Dr. Calais discussed efforts to move beyond small-molecule PSMA ligands like PSMA-617 by exploring antibody-based approaches, notably J591, which offers distinct pharmacokinetic and targeting properties. Unlike PSMA-617 (1 kDa), the J591 antibody is much larger (150 kDa), leading to prolonged blood circulation and potentially higher tumor retention and radiation dose delivery. Several ongoing trials are investigating these agents, including the ProstACT Select, ProstACT TARGET, and ProstACT Global studies by Telix, and the CONVERGE-01 trial by Convergent Therapeutics. Early data with Lu177- and Ac225-labeled J591 have shown encouraging PSA declines and durable disease control in heavily pretreated mCRPC populations.

Furthermore, Dr. Calais highlighted that the theranostic field in prostate cancer is expanding rapidly beyond PSMA, with several novel molecular targets under active investigation. These include ACP3, STEAP1, CD46, HK2, GRPR, and DLL3, all of which show potential for imaging and therapeutic applications in mCRPC. Early-phase clinical data have demonstrated encouraging tumor uptake and target specificity, suggesting that these agents could serve as complementary or alternative strategies, particularly for PSMA-negative or heterogeneous disease. Emerging targets such as KLK3 and TROP2 further broaden the horizon, underscoring the ongoing evolution of precision radiotheranostics in prostate cancer.

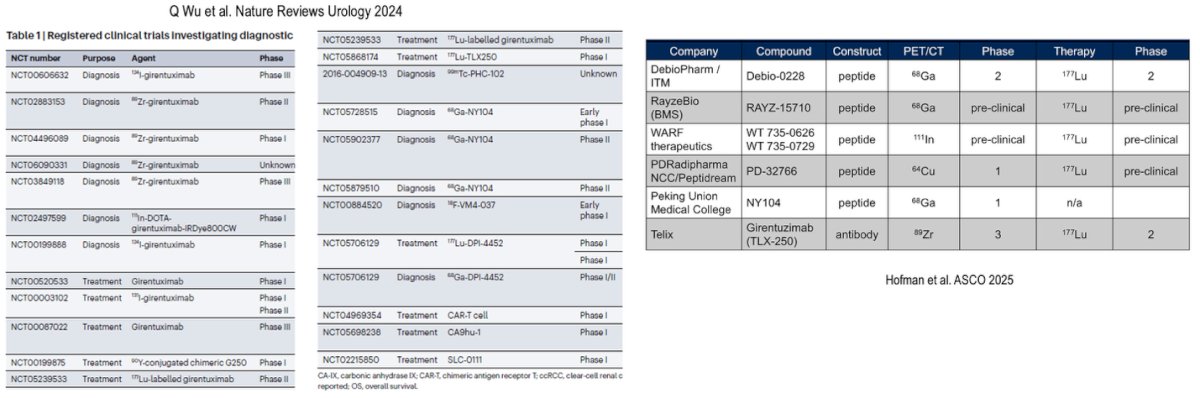
Theranostic advances extend beyond PSMA and SSTR, spotlighting Carbonic Anhydrase IX (CAIX) as a novel and promising target, particularly in clear cell renal cell carcinoma (ccRCC). He showcased data with 68Ga-DPI-4452 PET imaging, which demonstrates strong uptake in both primary and metastatic ccRCC lesions, often with SUVmax values exceeding 20 and even reaching over 100. Early therapeutic experience using ^77Lu-DPI-4452 across three cycles (10, 44, and 66 mCi) has shown meaningful radiotracer retention and on-treatment response compared to baseline scans. These findings underscore the expanding role of molecularly targeted radionuclide therapies across genitourinary malignancies, marking CAIX as an exciting next frontier in radiotheranostics.

Dr. Calais highlighted the rapidly expanding landscape of CAIX-targeted radiotheranostics, with multiple ongoing trials evaluating novel peptide and antibody-based agents across diagnostic and therapeutic settings, as shown below.
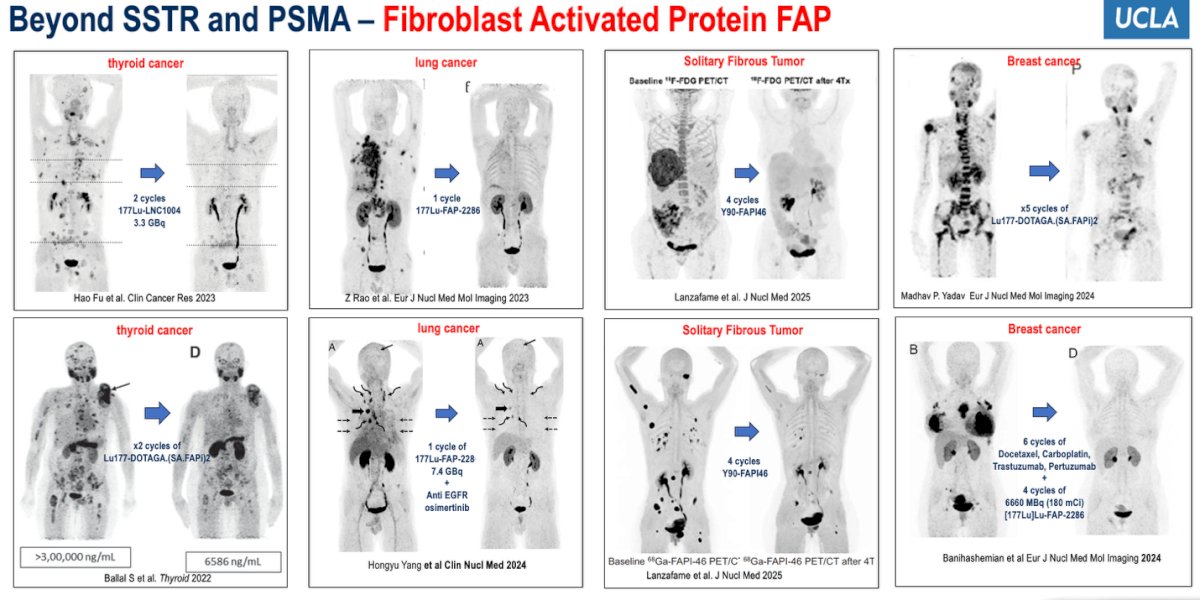
Dr. Calais then discussed the emerging role of Fibroblast Activated Protein (FAP) as a theranostic target, presenting compelling clinical imaging and treatment data across various malignancies, including thyroid, lung, solitary fibrous tumors, and breast cancer, where FAP-targeted radioligand therapy has shown promising responses after multiple treatment cycles.
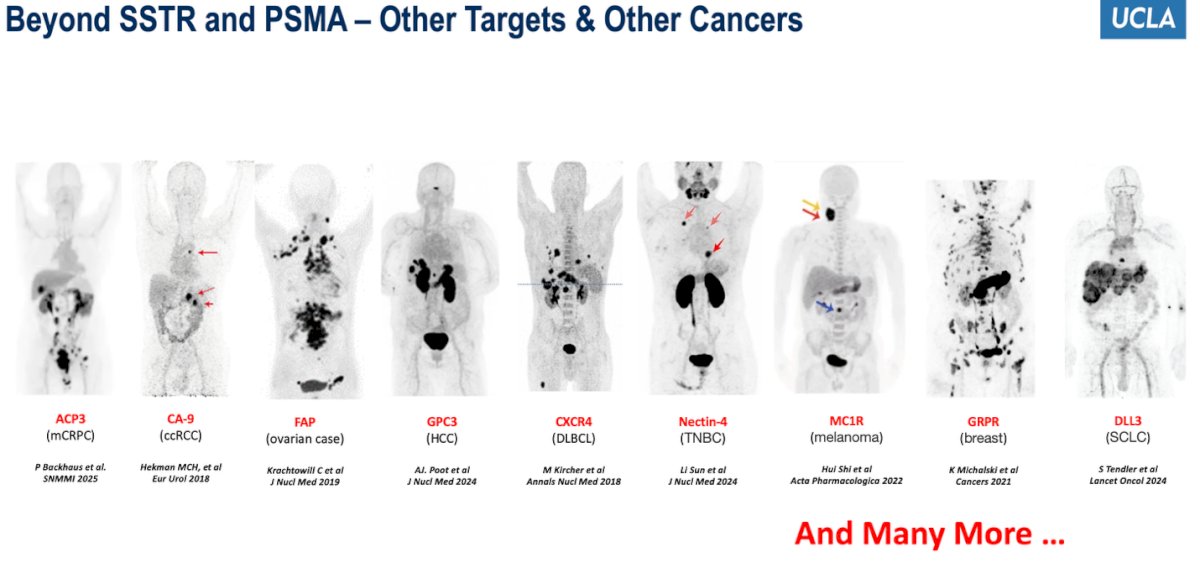
Dr. Calais emphasized that there are now numerous theranostic targets being investigated beyond SSTR and PSMA, including ACP3 in prostate cancer, CAIX in renal cell carcinoma, FAP in ovarian and other solid tumors, GPC3 in hepatocellular carcinoma, CXCR4 in lymphoma, Nectin-4 in triple-negative breast cancer, MC1R in melanoma, GRPR in breast cancer, and DLL3 in small-cell lung cancer, illustrating how the field is rapidly evolving to encompass a wide range of malignancies.
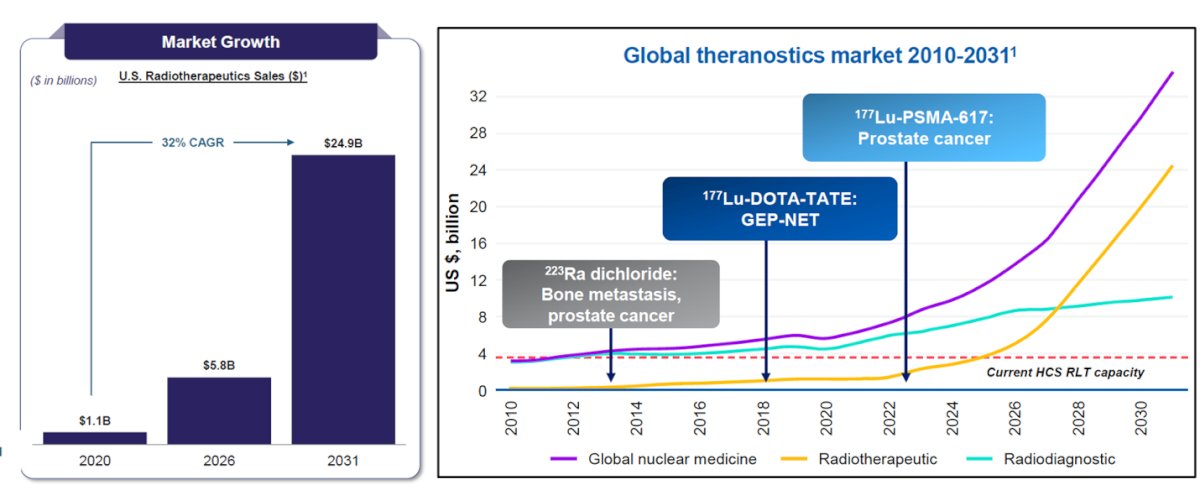
Lastly, Dr. Calais highlighted the explosive growth of the radiotheranostics field, noting that over 250 clinical trials are currently underway across more than 20 cancer types, with over 60 active assets in development. He illustrated the expanding biopharma investment landscape and projected market growth from $1.1 billion in 2020 to nearly $25 billion by 2031 driven by innovation in radioisotopes, targeting molecules, and next-generation agents beyond 177Lu-PSMA-617.
Dr. Calais concluded his presentation by emphasizing the success of the VISION trial, describing it as the legacy model for theranostics in metastatic castration-resistant prostate cancer (mCRPC).1 He outlined that the effectiveness of Lu-177–PSMA therapy stems from its ability to target an antigen highly overexpressed by most prostate cancer cells, the use of radiopharmaceuticals with minimal background activity, and the integration of companion imaging agents for precise patient selection and real-time monitoring. This paradigm has paved the way for expanding radioligand therapy into earlier disease settings, exploring new radionuclides and ligands, and extending theranostics beyond prostate cancer to new targets and tumor types.
Presented by: Jeremie Calais, MD, MSc, PhD, Certified Principal Investigator, ACRIP, Associate Professor, Department of Molecular and Medical Pharmacology, Director, Theranostics Program, Director, Clinical Research Program, Ahmanson Translational Theranostics Division, David Geffen School of Medicine, University of California, Los Angeles (UCLA), Los Angeles, CA
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.
Reference:
- Sartor O, de Bono J, Chi KN, Fizazi K, Herrmann K, Rahbar K, Tagawa ST, Nordquist LT, Vaishampayan N, El-Haddad G, Park CH, Beer TM, Armour A, Pérez-Contreras WJ, DeSilvio M, Kpamegan E, Gericke G, Messmann RA, Morris MJ, Krause BJ; VISION Investigators. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103. doi: 10.1056/NEJMoa2107322. Epub 2021 Jun 23. PMID: 34161051; PMCID: PMC8446332.
- Morris MJ, Castellano D, Herrmann K, de Bono JS, Shore ND, Chi KN, Crosby M, Piulats JM, Fléchon A, Wei XX, Mahammedi H, Roubaud G, Študentová H, Nagarajah J, Mellado B, Montesa-Pino Á, Kpamegan E, Ghebremariam S, Kreisl TN, Wilke C, Lehnhoff K, Sartor O, Fizazi K; PSMAfore Investigators. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naive patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): a phase 3, randomised, controlled trial. Lancet. 2024 Sep 28;404(10459):1227-1239. doi: 10.1016/S0140-6736(24)01653-2. Epub 2024 Sep 15. Erratum in: Lancet. 2025 Dec 21;404(10471):2542. doi: 10.1016/S0140-6736(24)02716-8. PMID: 39293462; PMCID: PMC12121614.
- Emmett L, Subramaniam S, Crumbaker M, Nguyen A, Joshua AM, Weickhardt A, Lee ST, Ng S, Francis RJ, Goh JC, Pattison DA, Tan TH, Kirkwood ID, Gedye C, Rutherford NK, Sandhu S, Kumar AR, Pook D, Ramdave S, Nadebaum DP, Voskoboynik M, Redfern AD, Macdonald W, Krieger L, Schembri G, Chua W, Lin P, Horvath L, Bastick P, Butler P, Zhang AY, Yip S, Thomas H, Langford A, Hofman MS, McJannett M, Martin AJ, Stockler MR, Davis ID; ENZA-p Trial Investigators and the Australian and New Zealand Urogenital and Prostate Cancer Trials Group. [177Lu]Lu-PSMA-617 plus enzalutamide in patients with metastatic castration-resistant prostate cancer (ENZA-p): an open-label, multicentre, randomised, phase 2 trial. Lancet Oncol. 2024 May;25(5):563-571. doi: 10.1016/S1470-2045(24)00135-9. Epub 2024 Apr 12. PMID: 38621400.
- Emmett L, Subramaniam S, Crumbaker M, Joshua AM, Sandhu S, Nguyen A, Weickhardt A, Lee ST, Ng S, Francis RJ, Goh JC, Pattison DA, Tan TH, Kirkwood ID, Gedye C, Rutherford NK, Kumar ASR, Pook D, Ramdave S, Nadebaum DP, Voskoboynik M, Redfern AD, Macdonald W, Krieger L, Schembri G, Chua W, Lin P, Horvath L, Bastick P, Butler P, Zhang AY, McJannett M, Thomas H, Langford A, Hofman MS, Martin AJ, Davis ID, Stockler MR; ENZA-p Trial Investigators; Australian and New Zealand Urogenital and Prostate Cancer Trials Group. Overall survival and quality of life with [177Lu]Lu-PSMA-617 plus enzalutamide versus enzalutamide alone in metastatic castration-resistant prostate cancer (ENZA-p): secondary outcomes from a multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2025 Mar;26(3):291-299. doi: 10.1016/S1470-2045(25)00009-9. Epub 2025 Feb 13. PMID: 39956124.