(UroToday.com) The 2025 ESMO annual meeting featured a prostate cancer session and a presentation by Neal Shore, MD, FACS, discussing a post hoc analysis of EMBARK assessing baseline features and metastasis-free survival by prior definitive treatment in patients with high‑risk biochemically recurrent prostate cancer. The phase 3 EMBARK trial showed significant improvements in metastasis-free survival with enzalutamide + leuprolide and enzalutamide monotherapy versus leuprolide alone in patients with high‑risk biochemical recurrence.1
The results from EMBARK led to the approval of enzalutamide, with ADT and as monotherapy, for the treatment of non-metastatic castration sensitive prostate cancer with biochemical recurrence at high risk for metastasis. As biochemical recurrence following radical prostatectomy versus radiotherapy may be associated with different risk profiles, understanding whether efficacy varies based on prior treatment could help to inform personalized treatment decision-making. This post hoc analysis explores baseline features and metastasis-free survival stratified by prior definitive treatment: radical prostatectomy only, radiotherapy only, or radical prostatectomy + radiotherapy.
EMBARK included patients with high‑risk biochemically recurrent (defined as a PSA doubling time of ≤9 months), who were randomized 1:1:1 to receive enzalutamide + leuprolide, leuprolide alone, or enzalutamide monotherapy. Post hoc subgroup analyses descriptively compared baseline features and metastasis-free survival in mutually exclusive prior treatment subgroups (radical prostatectomy, radiotherapy, or radical prostatectomy + radiotherapy).
Across all three treatment groups (enzalutamide combination, enzalutamide monotherapy, or leuprolide alone), most patients had prior radical prostatectomy + radiotherapy:

Baseline features were broadly similar across prior treatment groups. There was a greater percentage of Asian patients in the radical prostatectomy-only subgroup than in the radiotherapy-only or radical prostatectomy + radiotherapy subgroups, and radical prostatectomy-only patients were disproportionately represented among those with PSA doubling time <= 3 months. Patients who received prior radiotherapy only were slightly older and had higher PSAs than patients who received radical prostatectomy or radical prostatectomy + radiotherapy.
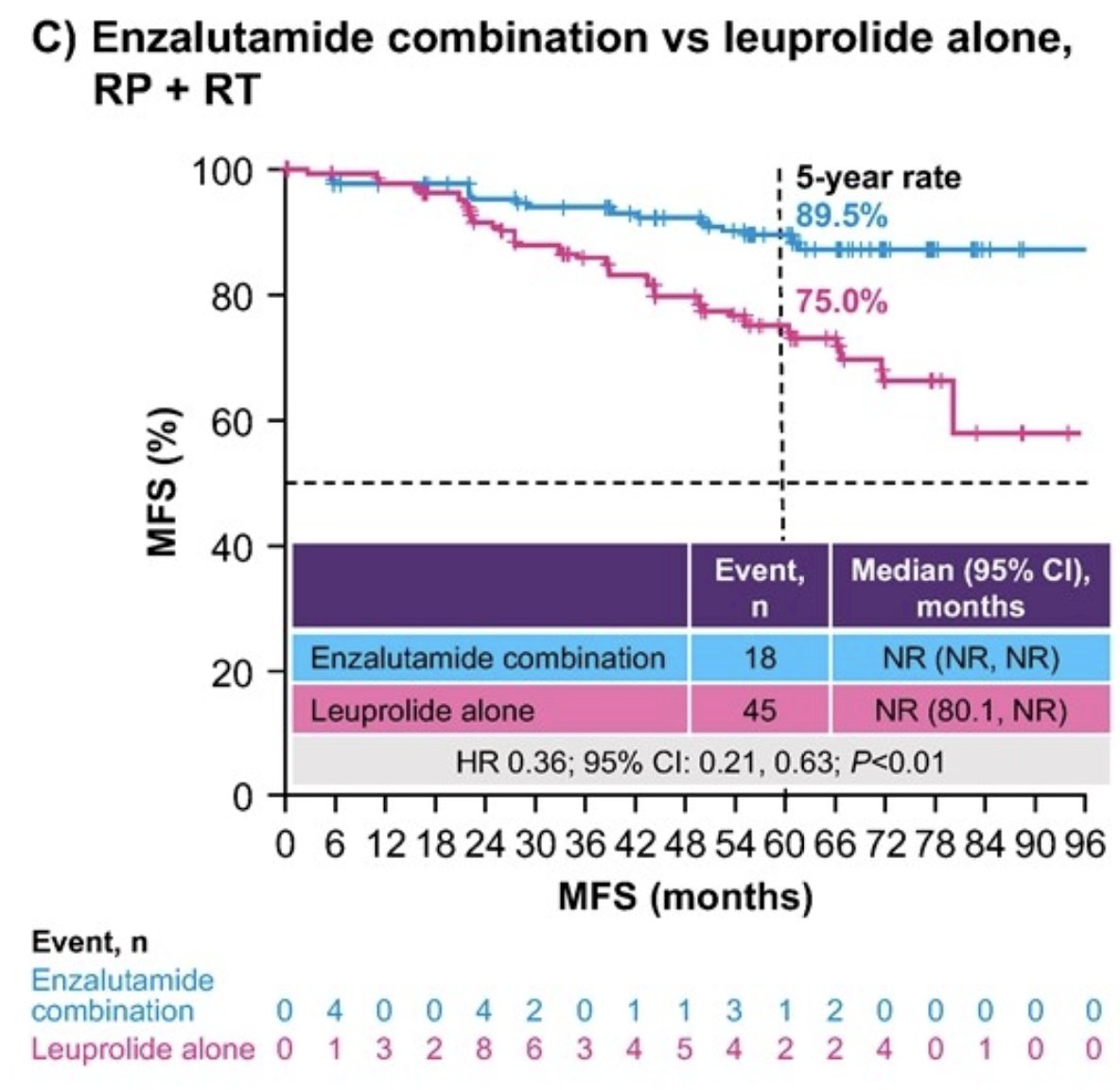
Enzalutamide + leuprolide showed improved metastasis free survival versus leuprolide alone across all prior treatments: radical prostatectomy (HR 0.37, 95% CI 0.16–0.87, p < 0.02), radiotherapy (HR 0.57, 95% CI 0.32–1.00, p < 0.05), and radical prostatectomy + radiotherapy (HR 0.36, 95% CI 0.21–0.63, p < 0.01):

 \
\
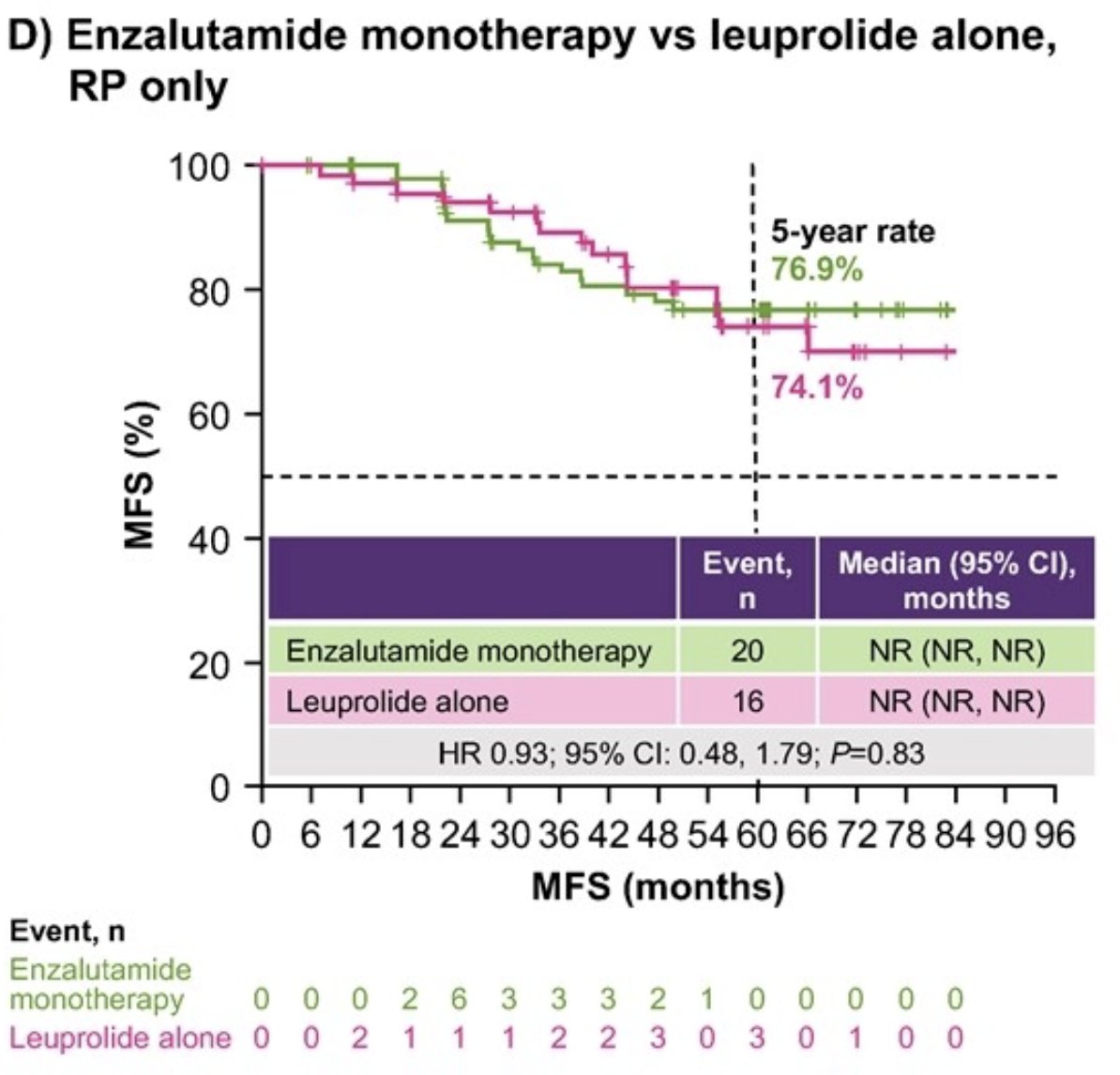
No difference in metastasis-free survival was found between enzalutamide monotherapy and leuprolide alone in the radical prostatectomy only subgroup, though the number of events was small in both arms (HR 0.93, 95% CI 0.48–1.79, p = 0.83):
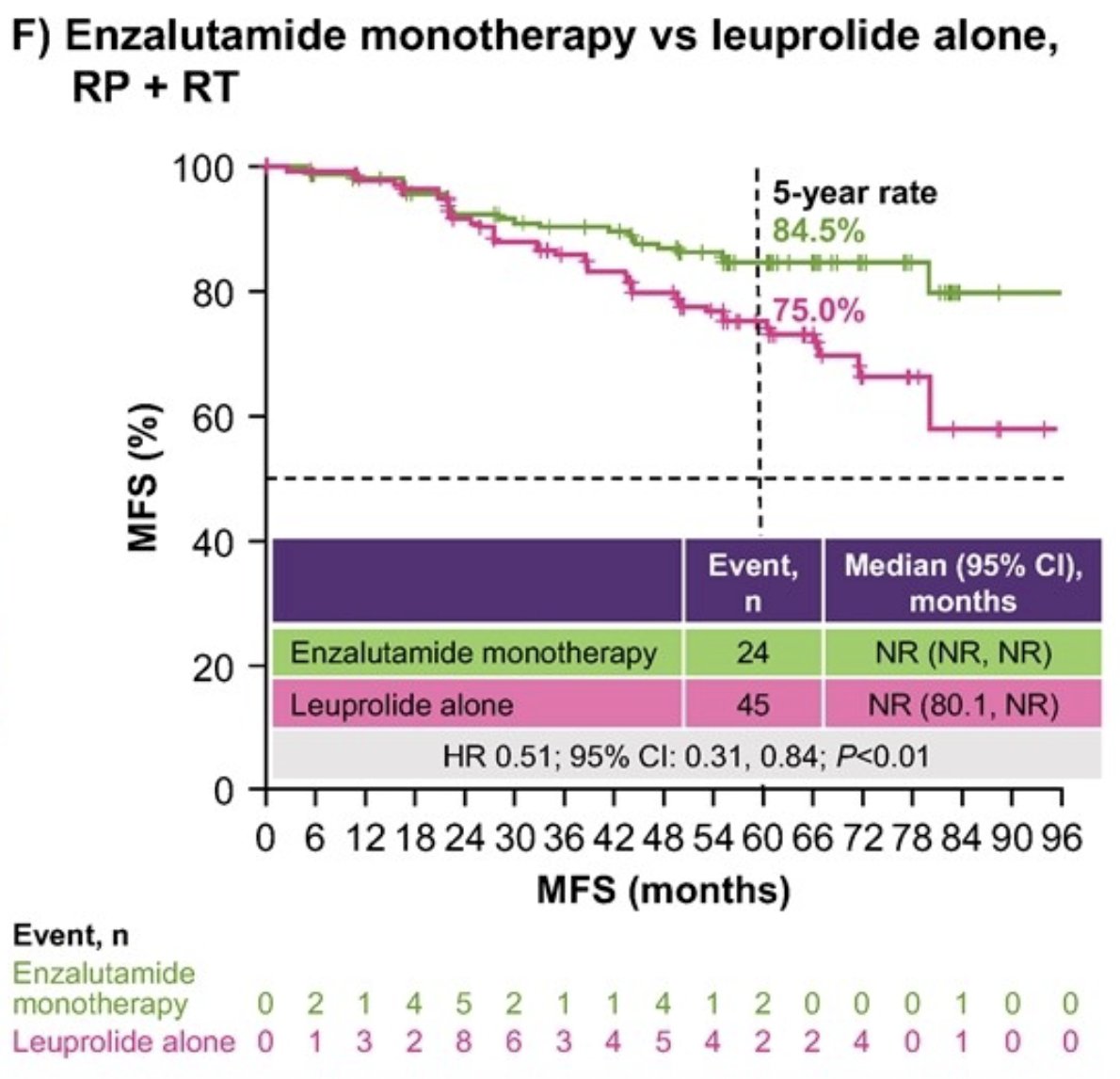
Enzalutamide monotherapy showed improved metastasis-free survival versus leuprolide alone in the radical prostatectomy + radiotherapy subgroup (HR 0.51, 95% CI 0.31–0.84, p < 0.01) and numerically improved metastasis-free survival in the radiotherapy subgroup (HR 0.65, 95% CI 0.37–1.15, p = 0.13):

Importantly, there were no significant interactions between the combo arm and prior treatment (P-interaction = 0.52) or the mono arm and prior treatment (P-interaction = 0.40).
Dr. Shore concluded his presentation discussing a post hoc analysis of EMBARK assessing baseline features and metastasis-free survival by prior definitive treatment in patients with high‑risk biochemically recurrent prostate cancer, with the following take-home points:
- Data from this post hoc analysis align with the primary results from EMBARK
- Enzalutamide plus leuprolide showed improved metastasis-free survival versus leuprolide alone across all prior treatments
- Enzalutamide monotherapy showed improved metastasis-free survival versus leuprolide alone in the radical prostatectomy + radiotherapy subgroup, numerically improved metastasis-free survival in the radiotherapy-only subgroup, and no difference in the radical prostatectomy-only subgroup, but the absolute number of events was small
- Despite differences in hazard ratios across subgroups, the lack of interaction between the randomization arm and prior treatment group suggests that both enzalutamide combination and enzalutamide monotherapy improve metastasis-free survival versus leuprolide alone, regardless of prior definitive treatment, in patients with high-risk biochemical recurrent prostate cancer
Presented by: Neal Shore, MD, FACS, Director, CPI (Certified Principal Investigator by the Association of Clinical Research Professionals), Medical Director for the Carolina Urologic Research Center, AUC Urology Specialists, Myrtle Beach, South Carolina
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
Reference: