(UroToday.com) The 2025 ESMO annual meeting featured a prostate cancer session and a presentation by Dr. Hoda Abdel-Aty discussing the utilization of the CHAARTED and STAMPEDE2 criteria in the PSMA PET era. PSMA PET-guided treatment outcomes in synchronous metastatic prostate cancer remain limited. The CHAARTED criteria, based on conventional imaging, were previously noted to correlate with survival.1
The STAMPEDE2 definition is derived from the STAMPEDE M1 RT trial and the ESTRO-ASTRO oligometastatic disease definition. Thus, Dr. Abdel-Aty and colleagues explored clinical outcomes following PSMA PET-guided treatment by applying the CHAARTED and STAMPEDE2 disease volume definitions.
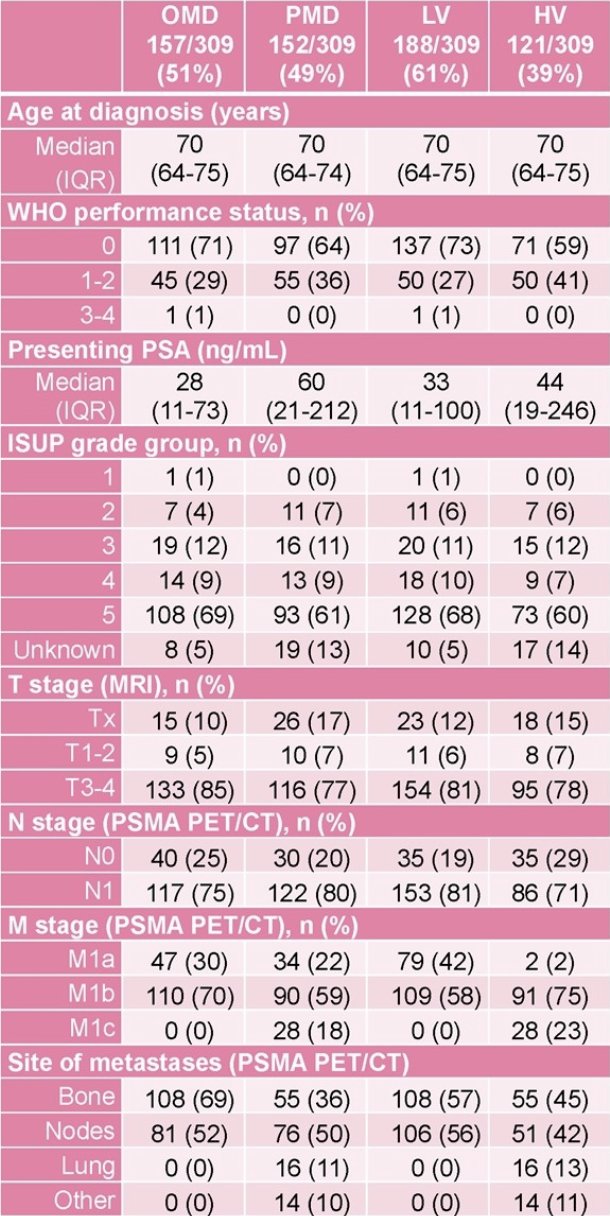
This study retrospectively reviewed 309 patients with synchronous metastatic prostate cancer confirmed on baseline PSMA PET at The Royal Marsden Hospital between December 2015-2022. Disease volume was classified using:
- CHAARTED criteria: low (≤3 bone metastases – low) versus high volume
- STAMPEDE2 criteria: oligometastatic (1-5 bone/non-regional nodes metastases) versus polymetastatic disease
Radiological best response (within 4 months of PSA nadir) and first progression/relapse patterns were analyzed. Progression/relapse was evaluated using PCWG3, RECIST, and PERCIST criteria. The median radiographic progression-free survival and overall survival were estimated using Kaplan-Meier methods, and adjusted Cox regression models were used to compare groups.
The mean age at diagnosis was 70 years, and the median follow-up was 38.5 months (IQR 28-50):
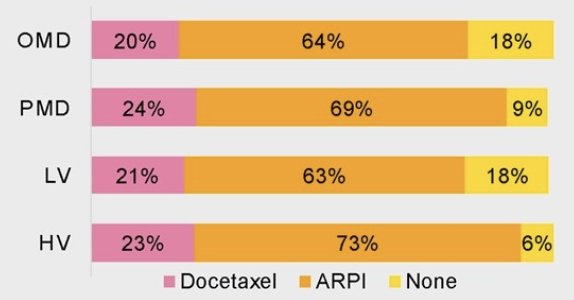
Use of systemic therapy in addition to ADT is highlighted in the following figure, which most commonly includes androgen receptor pathway inhibitors:
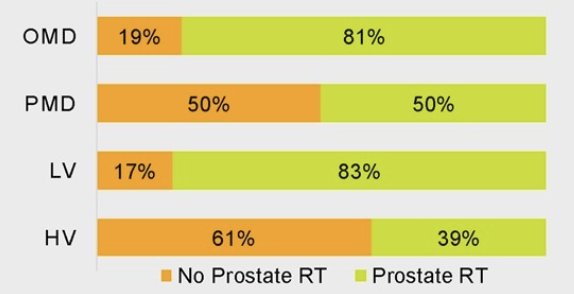
With regards to prostate radiotherapy, 69% of patients received prostate radiotherapy only, 28% received prostate and lymph node radiotherapy, and 16% received radiotherapy to the prostate (+/- pelvic lymph nodes) and metastatic lesions:
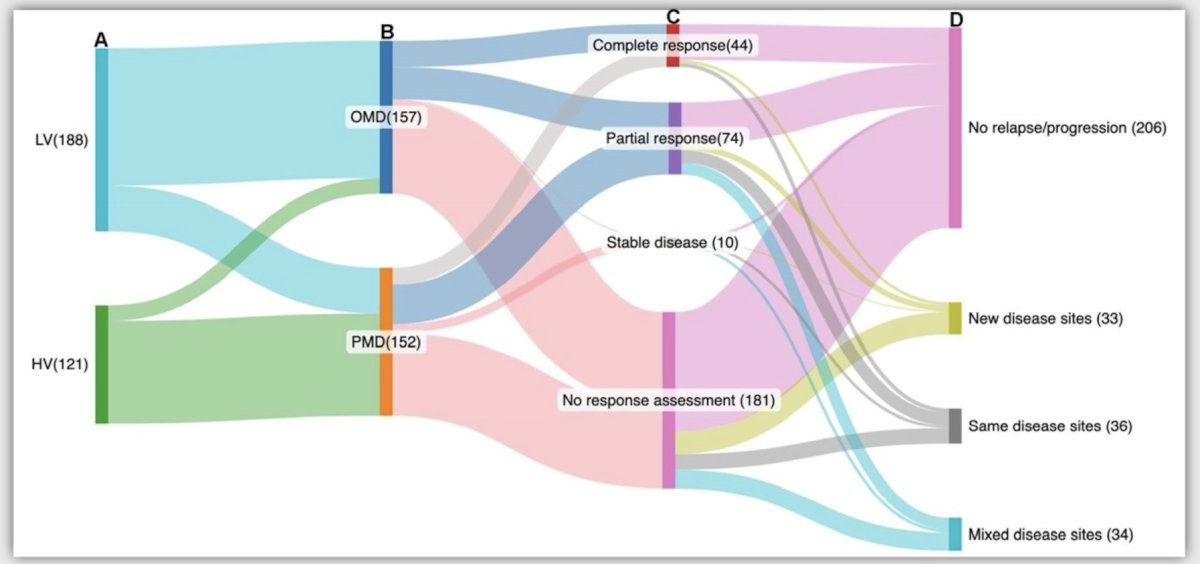
The Sankey plots show reclassification from PSMA PET CHAARTED low volume and high volume to STAMPEDE2-defined oligometastatic disease and polymetastatic disease (A-B), as well as patterns of radiological best response assessment and first relapse/progression (B-D):
Median radiographic progression-free survival was 73 months (95% CI 64-not reached) for oligometastatic disease and 41 months (95% CI 32-47) for polymetastatic disease. Moreover, median radiographic progression-free survival was 71 months (95% CI 63-not reached) for low volume and 36 months (95% CI 27-44) for high volume:

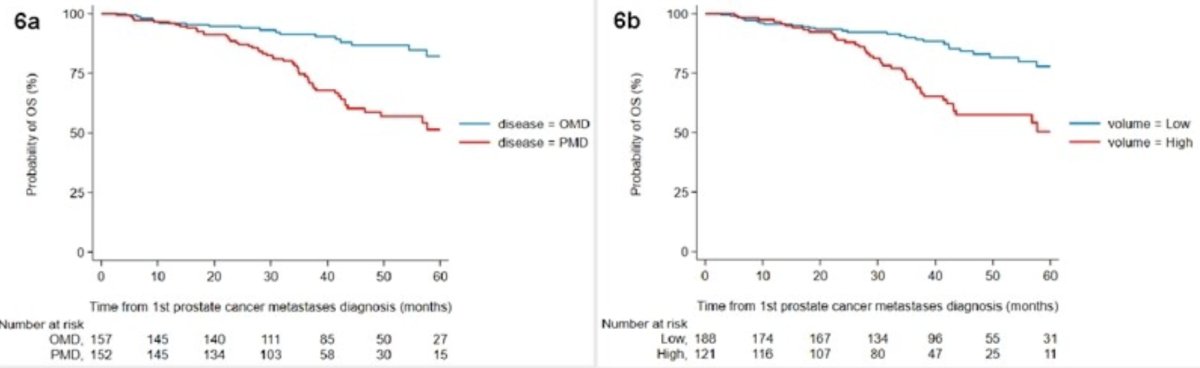
Median overall survival was not reached (95% CI not reached-not reached) for oligometastatic disease and 64 months (95% CI 47-not reached) for polymetastatic disease. Furthermore, median overall survival was not reached (95% CI not reached-not reached) for low volume and 90 months (95% CI 43-not reached) for high volume:
Dr. Abdel-Aty concluded her presentation discussing utilization of the CHAARTED and STAMPEDE2 criteria in the PSMA PET era with the following take-home points:
- This contemporary series demonstrated that radiographic progression-free survival and overall survival were comparable across PSMA PET-defined CHAARTED and STAMPEDE2 groups, demonstrating meaningful risk stratification similar to conventional imaging
- Accordingly, the ongoing STAMPEDE2 trial (NCT06320067) now incorporates PSMA PET for primary disease group classification in both comparison S (stereotactic ablative radiotherapy) and P (177Lu-PSMA-617)
Presented by: Hoda Abdel-Aty, MD, The Royal Marsden, London, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
Reference: