(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress, held in Berlin, German,y was host to a trials-in-progress prostate cancer poster session. Dr. Fred Saad presented the ongoing PSMACare trial, a phase II trial of [177Lu]Lu-PSMA-617 +/- an androgen receptor pathway inhibitor (ARPI) in patients with PSMA-positive non-metastatic castration-resistant prostate cancer (nmCRPC).
The PSMA-targeted radioligand therapy 177Lu-PSMA-617 prolongs radiographic progression-free survival (rPFS) with a manageable safety profile in patients with PSMA-positive metastatic castration-resistant prostate cancer (mCRPC) in post-taxane (VISION) and taxane-naive (PSMAfore) settings.1,2
Approximately 97% of patients with non-metastatic CRPC (nmCRPC) by conventional imaging have PSMA-positive disease.3 Androgen deprivation therapy (ADT) and second-generation androgen receptor pathway inhibitors (ARPIs) remain the standard of care for patients with nmCRPC.4 However, nearly 60% of patients with nmCRPC progress and develop metastatic disease within 5 years.5
177Lu-PSMA-617 may act synergistically with ARPIs and ADT to delay metastatic progression.6 The PSMACare trial (NCT05849298) evaluates the efficacy and safety of 177Lu-PSMA-617 with and without ARPIs in patients with PSMA-positive CRPC and no evidence of metastases by conventional imaging (CT/MRI and bone scan).
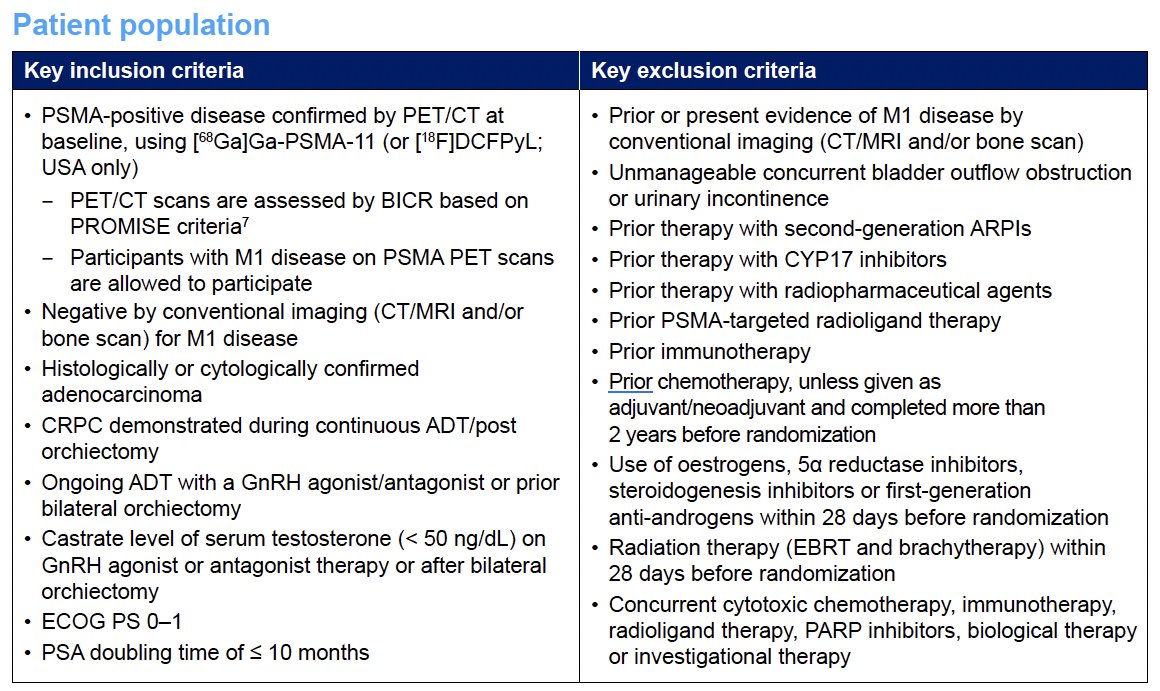
PSMACare is an ongoing international, prospective, open-label, multicentre, randomized, non-comparative phase II trial. The inclusion and exclusion criteria are summarized in the table below. The key criteria are as follows:
- Inclusion
- PSMA-positive disease confirmed by PET/CT at baseline, using [68Ga]Ga-PSMA-11 (or [18F]DCFPyL; USA only)
- PET/CT scans are assessed by BICR based on PROMISE criteria7
- Participants with M1 disease on PSMA PET scans are allowed to participate
- Negative conventional imaging for M1 disease
- PSA doubling time ≤10 months
- PSMA-positive disease confirmed by PET/CT at baseline, using [68Ga]Ga-PSMA-11 (or [18F]DCFPyL; USA only)
- Exclusion
- Prior or current evidence of M1 disease by conventional imaging
- Prior therapy with an ARPI or CYP17 inhibitor
- Prior therapy with a radiopharmaceutical
- Prior immunotherapy
- Prior chemotherapy, unless given as adjuvant/neoadjuvant and completed >2 years before randomization
Approximately 120 patients will be randomized 1:1 to receive 177Lu-PSMA-617 (7.4 GBq ± 10% every 6 weeks, up to 6 cycles) or 177Lu-PSMA-617 + ARPI (apalutamide, darolutamide or enzalutamide; Figure 1). Randomization will be stratified by PSMA-positive distant metastasis on PSMA PET/CT as assessed by BICR. Ongoing treatment with ADT is mandatory in both arms, and best supportive care is permitted in both arms.
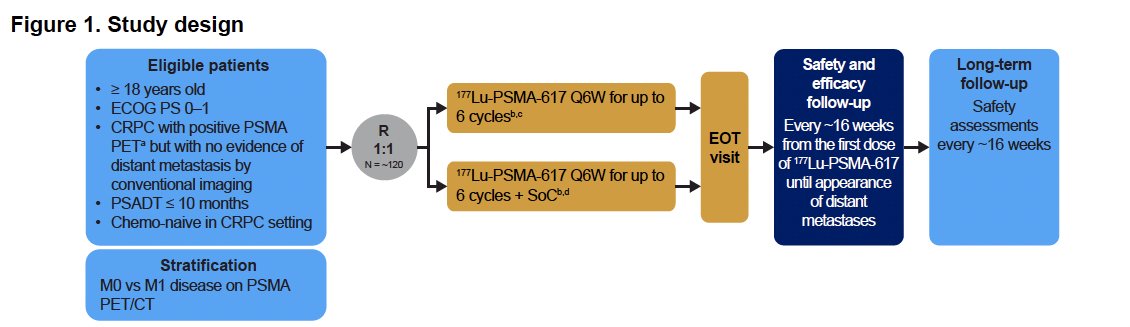
Patients randomized to 177Lu-PSMA-617 plus ARPI may continue to receive ARPI beyond 36 weeks (i.e. after 177Lu-PSMA-617 is completed) at the investigator’s discretion. Patients may also continue to receive ARPI following discontinuation of 177Lu-PSMA-617 for any reason.
Efficacy follow-up assessments will occur every 16 weeks from date of the first administration of 177Lu-PSMA-617, continuing until appearance of distant metastases. Safety follow-up visits will be aligned with the efficacy follow-up visits and will continue until the global end of study. The study duration will be approximately 60 months. At the end of the study, participants will be eligible to join a long-term safety follow-up study.
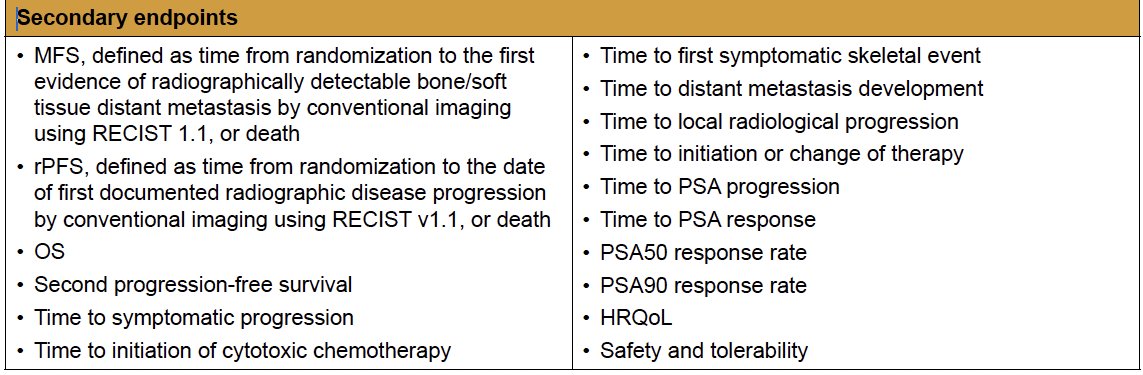
The primary study endpoint is the PSA response rate, defined as the proportion of participants who have a post-baseline PSA nadir value of ≤ 0.2 ng/mL confirmed by a second PSA measurement ≥ 4 weeks later. The secondary endpoints are as follows:
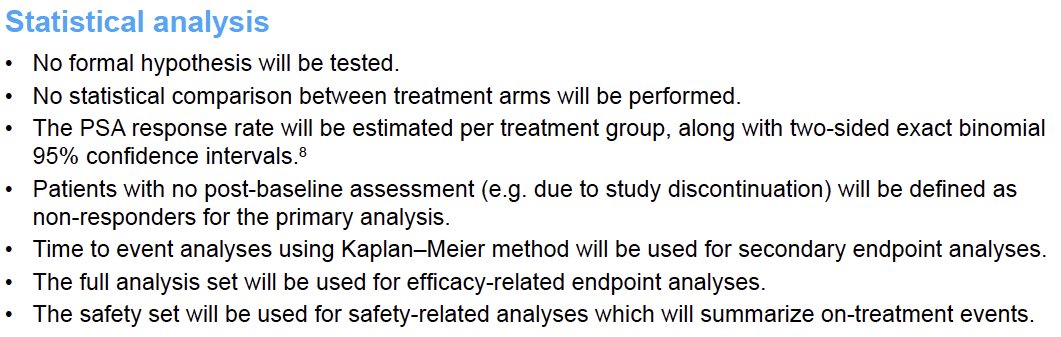
The statistical plan is as follows:
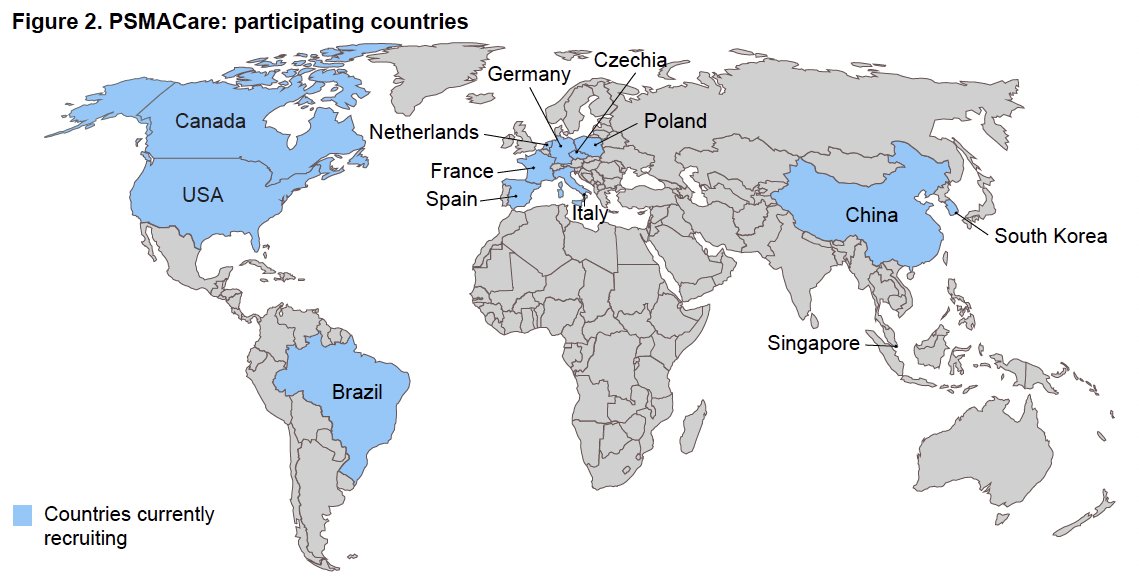
A protocol amendment is currently undergoing health authority evaluation. This amendment is designed to introduce more flexible inclusion/exclusion criteria in order to expand the eligible patient population, leveraging new clinical evidence and enhancing study feasibility. As of August 2025, patient enrolment has commenced in 13/13 countries (Figure 2).
Presented by: Fred Saad, MD, FRCSC, University of Montreal Hospital Center, Montreal, Canada
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025 '
Related content: PSMACare Trial: Phase 2 Study Evaluating Lutetium-Based RLT in Non-Metastatic CRPC - Fred Saad
References:
- Sartor O, de Bono J, Chi KN, et al. Lutetium-177–PSMA-617 for metastatic castration-resistant prostate cancer. N Engl J Med. 2021; 385:1091–1103.
- Morris MJ, Hirmand M, Chi KN, et al. PSMAfore: a randomized, phase 3 trial of [177Lu]Lu-PSMA-617 versus a change in androgen receptor pathway inhibitor in taxane-naïve metastatic castration-resistant prostate cancer. Lancet. 2024; 404:1227–1239.
- Fendler WP, Calais J, Eiber M, et al. Assessment of 68Ga-PSMA-11 PET accuracy in localizing recurrent prostate cancer: a prospective single-arm clinical trial. JAMA Oncol. 2019;5: 856–863.
- Cornford P, van den Bergh RCN, Briers E, et al. EAU–EANM–ESTRO–ESUR–ISUP–SIOG Guidelines on Prostate Cancer – Limited Update March 2025. Netherlands: European Association of Urology; 2025. Available at: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-EANM-ESTRO-ESUR-ISUP-SIOG-Guidelines-on-Prostate-Cancer-2025_updated.pdf. Accessed October 13, 2025.
- Moreira DM, Jayachandran J, Presti JC Jr, et al. Validation of a nomogram to predict pathological stage of clinically localized prostate cancer. Urology. 2016; 96:171–176.
- Kinikoglu O, Gultekin MH, Sahin S, et al. Prognostic value of baseline neutrophil-to-lymphocyte ratio in patients with metastatic hormone-sensitive prostate cancer receiving androgen deprivation therapy. J Clin Med. 2024; 13:4585.
- Eiber M, Herrmann K, Calais J, et al. Prostate cancer molecular imaging standardized evaluation (PROMISE): proposed miTNM classification for PSMA-ligand PET/CT. J Nucl Med. 2018; 59:469–478.
- Clopper CJ, Pearson ES. The use of confidence or fiducial limits illustrated in the case of the binomial. Biometrika. 1934; 26:404–413.