(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between October 17th and 21st was host to the session Mini oral session: GU tumours, prostate, penile and testis. Dr. Marc-Oliver Grimm presented the LBA92 - 3-Weekly Docetaxel 75 mg/m2 vs 2-Weekly Docetaxel 50 mg/m2 in Combination with Darolutamide + ADT in Patients with mHSPC – Results from the Randomised Phase 3 ARASAFE Trial.
Dr. Oliver-Grimm opened his presentation by emphasizing that triple therapy combining androgen deprivation therapy (ADT), darolutamide, and docetaxel (75 mg/m² every 3 weeks for six cycles, as evaluated in the ARASENS trial, NCT02799602) is an approved treatment option for men with metastatic hormone-sensitive prostate cancer (mHSPC).1 However, he noted that toxicity, particularly neutropenic complications, can limit the widespread use of docetaxel-based regimens when compared with ADT plus an androgen receptor pathway inhibitor (ARPI) alone.
He highlighted that in the metastatic castration-resistant prostate cancer (mCRPC) setting, a modified docetaxel dosing schedule of 50 mg/m² every two weeks in a four-week cycle has previously shown improved time to treatment failure and reduced rates of grade 3–4 adverse events, including neutropenia, leukopenia, and febrile neutropenia. Based on these findings, the investigators hypothesized that triple therapy with darolutamide, ADT, and biweekly docetaxel could achieve similar efficacy while reducing the incidence of severe (grade 3–5) adverse events compared with the standard 75 mg/m² every 3 weeks regimen in patients with mHSPC.
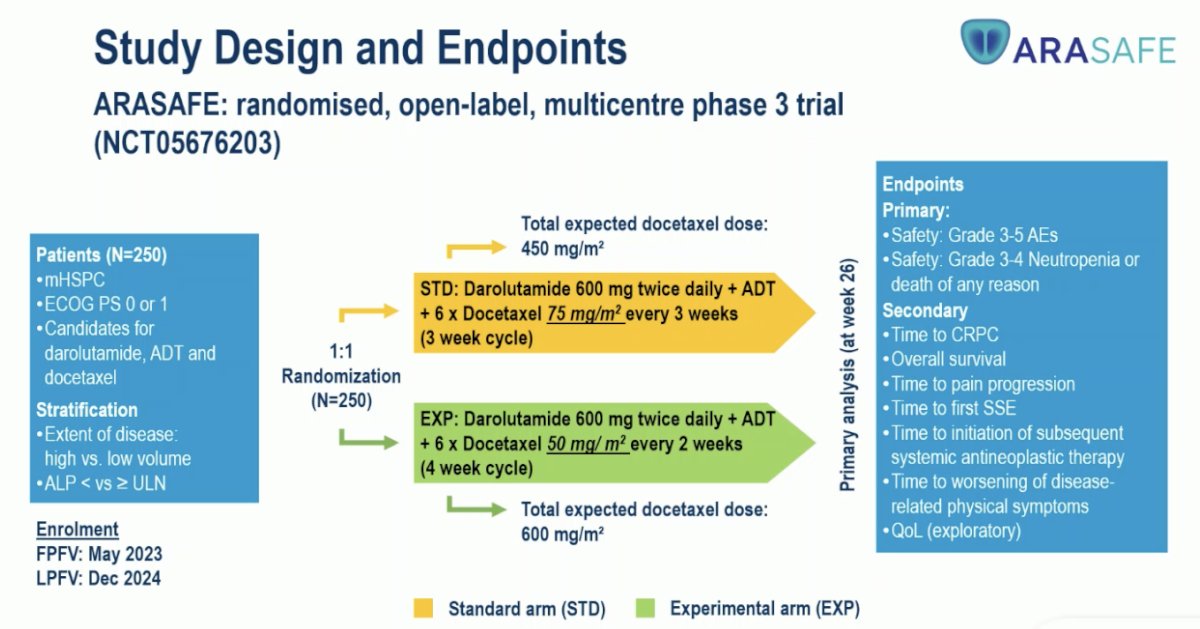
Between May 2023 and December 2024, the ARASAFE phase 3 trial (NCT05676203) randomized 250 patients with mHSPC in a 1:1 ratio to receive darolutamide 600 mg twice daily with ADT plus docetaxel administered either at 75 mg/m² every 3 weeks for six cycles (standard arm; total expected dose 450 mg/m²) or 50 mg/m² every 2 weeks for six cycles (experimental arm; total expected dose 600 mg/m²). The primary endpoints were the incidence of grade 3–5 adverse events and safety, particularly rates of grade 3–4 neutropenia or sepsis, while secondary endpoints included time to castration resistance, progression, first skeletal event, next systemic therapy, and quality-of-life outcomes. The study design is shown below.
Baseline characteristics were well balanced between treatment arms. The median age was 68 years in the standard arm and 67 years in the experimental arm, with most patients having an ECOG performance status of 0. High-volume disease was observed in approximately 85% of participants, and Gleason score ≥8 was reported in over 80% in both groups. Baseline median PSA levels and ALP stratification were also comparable. In terms of docetaxel exposure, patients in the 75 mg/m² Q3W arm received a mean of 5.6 cycles (cumulative dose 842.8 mg), while those in the 50 mg/m² Q2W arm completed a mean of 10.7 cycles (cumulative dose 1073.5 mg), consistent with the adjusted dosing schedule.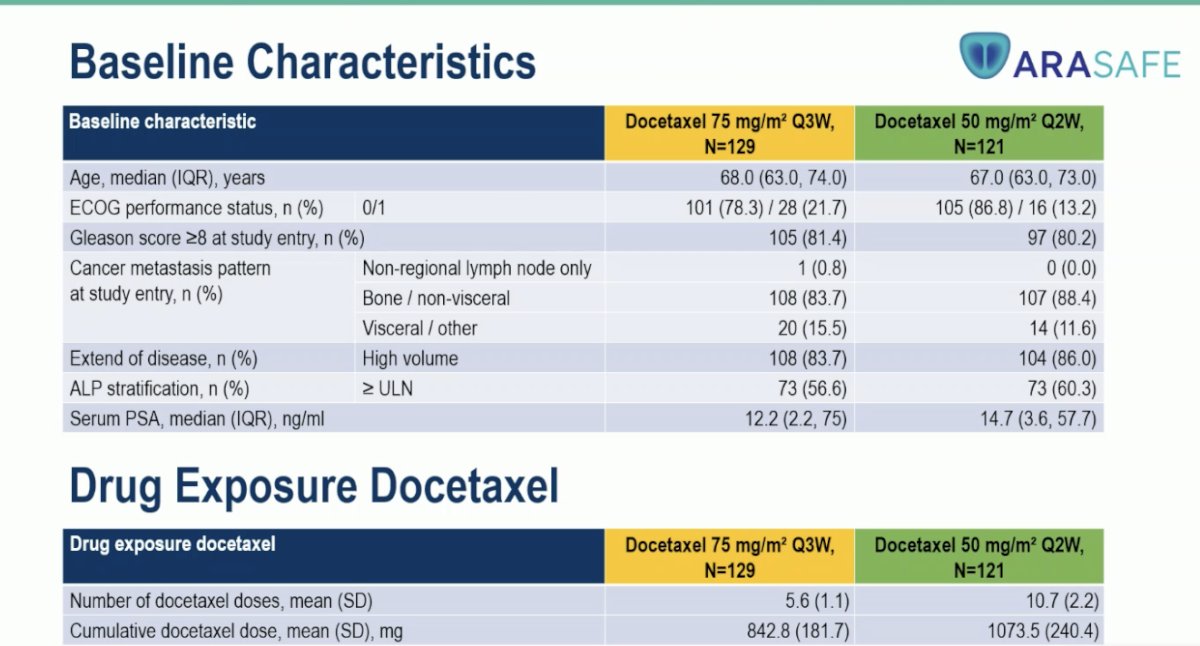
Notably, both treatment schedules included six cycles of docetaxel administered alongside continuous darolutamide (600 mg twice daily) and ADT. The standard arm received docetaxel 75 mg/m² every 3 weeks, while the experimental arm was treated with 50 mg/m² every 2 weeks. Study treatment lasted approximately 22 weeks, followed by an end-of-study visit at week 26 (±1 week) and a subsequent observation period, with additional blood samples collected at predefined intervals for safety assessments.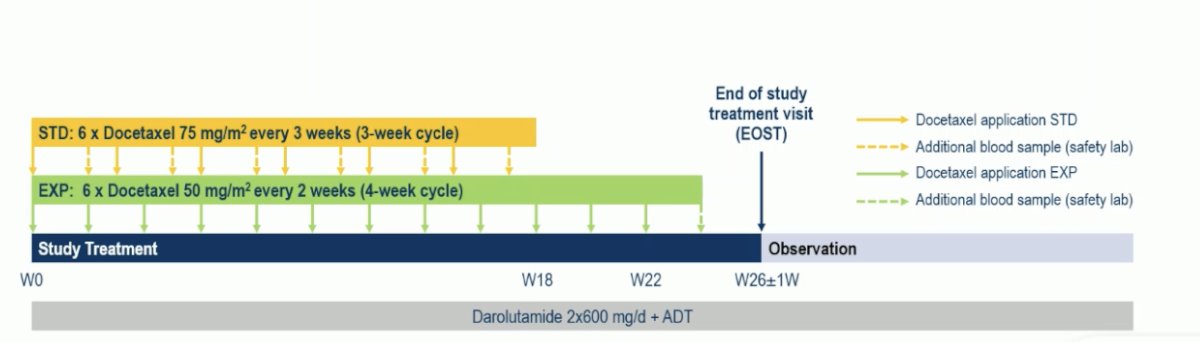
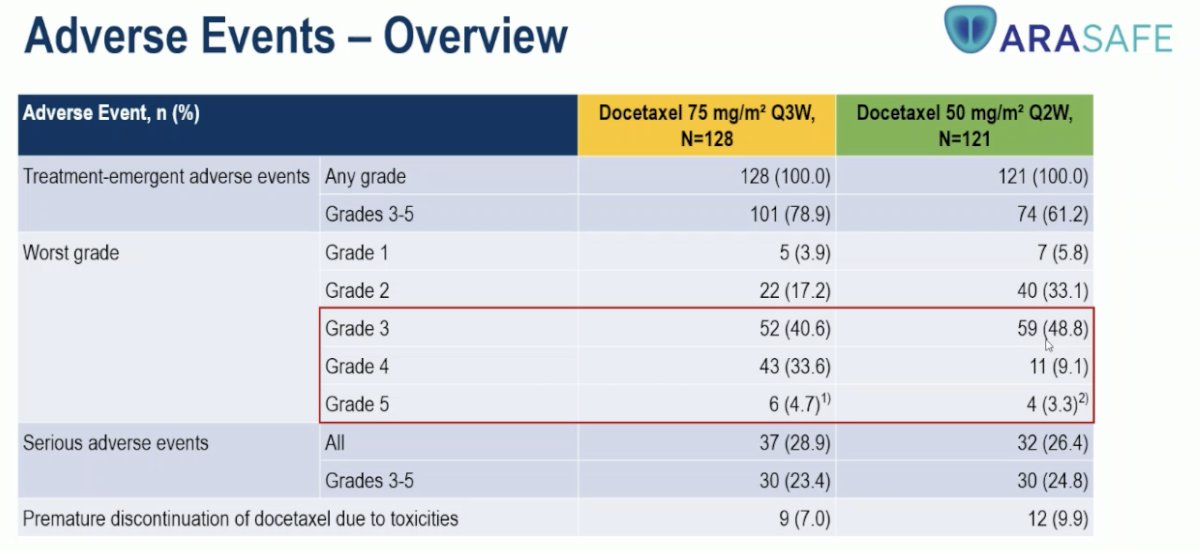
The primary endpoint showed a highly significant difference between treatment arms. Grade 3–5 adverse event rates were lower with the 50 mg/m² Q2W regimen (61.2%) compared to the 75 mg/m² Q3W regimen (78.9%; p=0.0024). Likewise, the incidence of grade 3–4 neutropenia or death was markedly reduced with the Q2W schedule (24.0% vs 64.1%; p<0.00001), highlighting a substantial safety advantage for the biweekly dosing approach.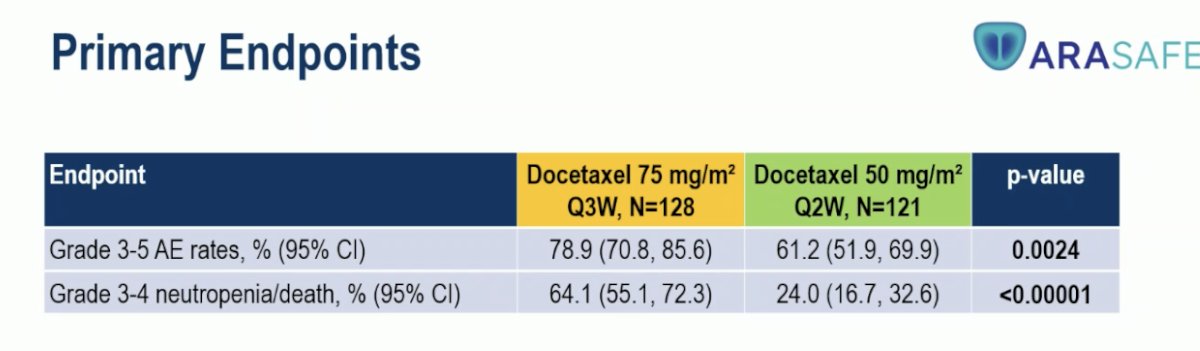
Specifically, grade 4 events were substantially reduced (9.1% vs 33.6%), and grade 5 events were infrequent in both groups (3.3% vs 4.7%). Serious adverse events and discontinuations due to toxicity were comparable between arms, with slightly.
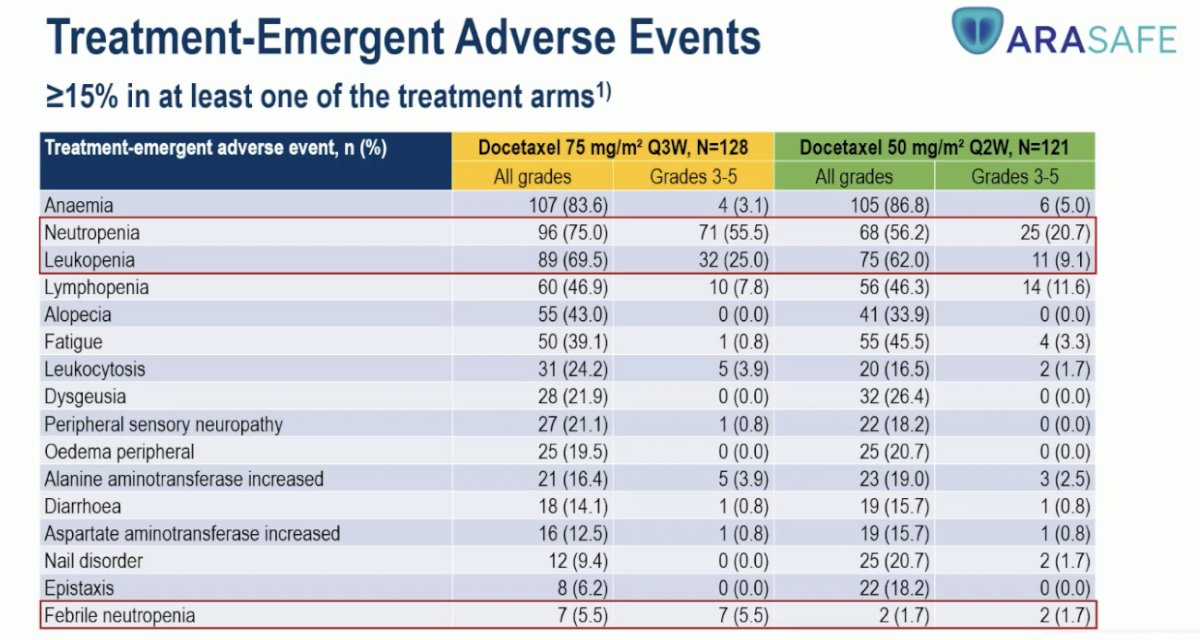
Hematologic toxicities were substantially more frequent with the 75 mg/m² Q3W regimen. Neutropenia occurred in 75% versus 56.2% of patients, leukopenia in 69.5% versus 62.0%, and febrile neutropenia in 5.5% versus 1.7% for the Q2W regimen. In contrast, non-hematologic adverse events such as fatigue, dysgeusia, and alopecia were comparable across both treatment arms, underscoring the improved hematologic safety profile of the lower-dose biweekly schedule.
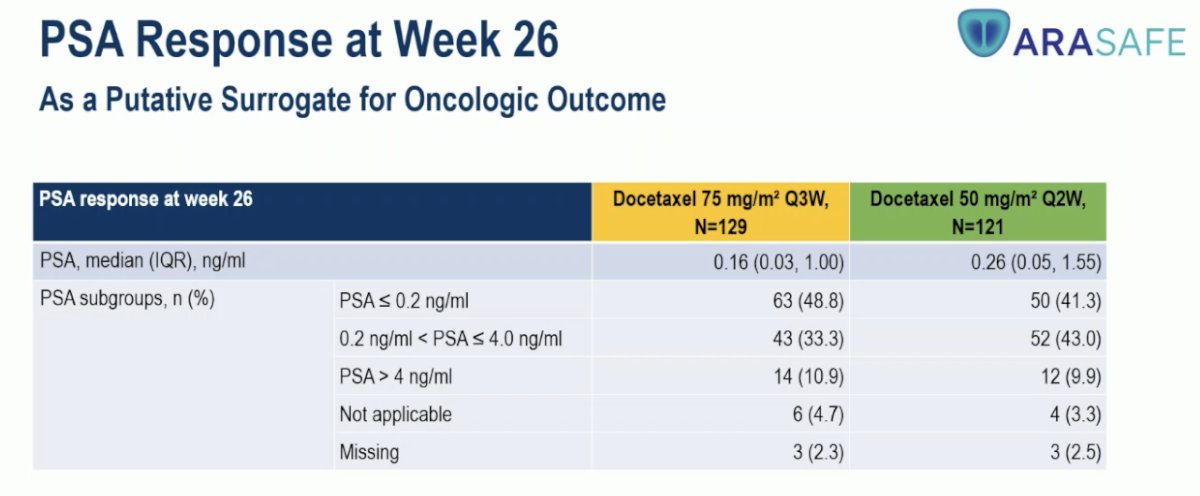
PSA response at week 26 was used as a putative surrogate for oncologic outcomes. Median PSA levels were comparable between arms 0.16 ng/mL in the standard group versus 0.26 ng/mL in the experimental arm. The proportion of patients achieving deep PSA suppression (≤0.2 ng/mL) was slightly higher with standard dosing (48.8%) compared to the biweekly schedule (41.3%), suggesting maintained biochemical efficacy despite lower and more frequent dosing.
Dr. Oliver-Grimm concluded his presentation with the following key points:
- ARASAFE demonstrated a statistically highly significant and clinically meaningful reduction in the incidence of grade 3–5 adverse events and grade 3/4 neutropenia or death in the experimental arm.
- This reduction was achieved despite a higher cumulative docetaxel dose in the experimental arm (mean 1074 mg vs 843 mg).
- The ARASAFE dosing strategy may represent a potential new standard of care for patients with mHSPC.
- Ongoing follow-up will evaluate oncologic outcomes, including time to mCRPC, overall survival, time to pain progression, time to first SSE, initiation of subsequent systemic therapy, and worsening of disease-related symptoms.
- Quality of life analyses will be conducted on an exploratory basis.
Presented by: Marc-Oliver Grimm, MD, Director of the Department of Urology at the University Hospital Jena, Jena, Germany.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.
Reference: