(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between October 17th and 21st was host to the Poster presentation session. Dr. J. Connor Wells presented the poster Durability of Complete Response (CR) to First Line (1L) in metastatic renal cell carcinoma (mRCC) in the Real World.
Dr. Wells began by highlighting that patients with metastatic RCC (mRCC) who achieve a complete response (CR) to immuno-oncology (IO)–based combinations often have an excellent prognosis and may experience durable remissions. However, real-world evidence on the durability of these CRs, long-term survival, and the need for subsequent lines of therapy remains limited.
To address this, the investigators leveraged data from the IMDC, identifying patients with mRCC treated with first-line (1L) therapy between 2015 and 2022 who achieved a documented CR. These patients were stratified by treatment type—IO plus VEGF-targeted therapy (IO VE), dual IO therapy (Ipilimumab + Nivolumab; IO IO), or VEGF monotherapy. Analyses focused on time to next treatment (TTNT), overall survival (OS), and patterns of subsequent therapy use across these treatment groups.
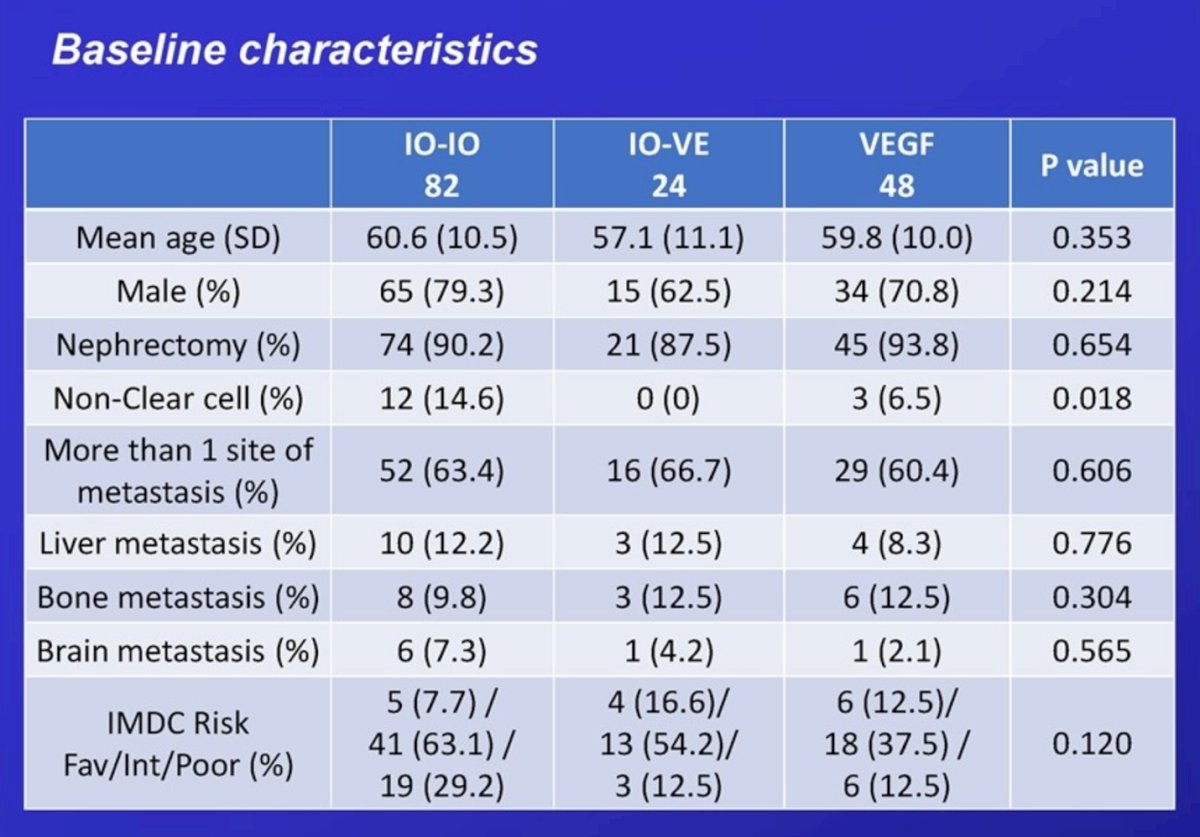
Baseline characteristics are summarized in the table. Notably, the mean age across treatment groups ranged from 57 to 61 years, with a predominance of male patients (~75–80%) and high rates of prior nephrectomy (>85%). The majority had clear cell histology, although 14.6% of patients in the IO–IO cohort had non–clear cell disease. Most patients presented with multiple sites of metastasis (~60–67%), while liver, bone, and brain metastases were less common (each <15%). IMDC risk distribution was similar across groups.
In terms of subsequent therapy, 13.4% of patients in the IO–IO cohort initiated a second-line regimen, with nearly two-thirds (63.6%) receiving an IO rechallenge. In contrast, 20.8% of patients in the IO–VE group started second-line therapy, and only one-fifth underwent IO retreatment.
With a median follow-up of 46.7 months, complete responses were documented in 3.1% of the overall IMDC population—most frequently among patients treated with IO–IO (6.3%), followed by IO–VE (3.9%) and VEGF monotherapy (1.5%).
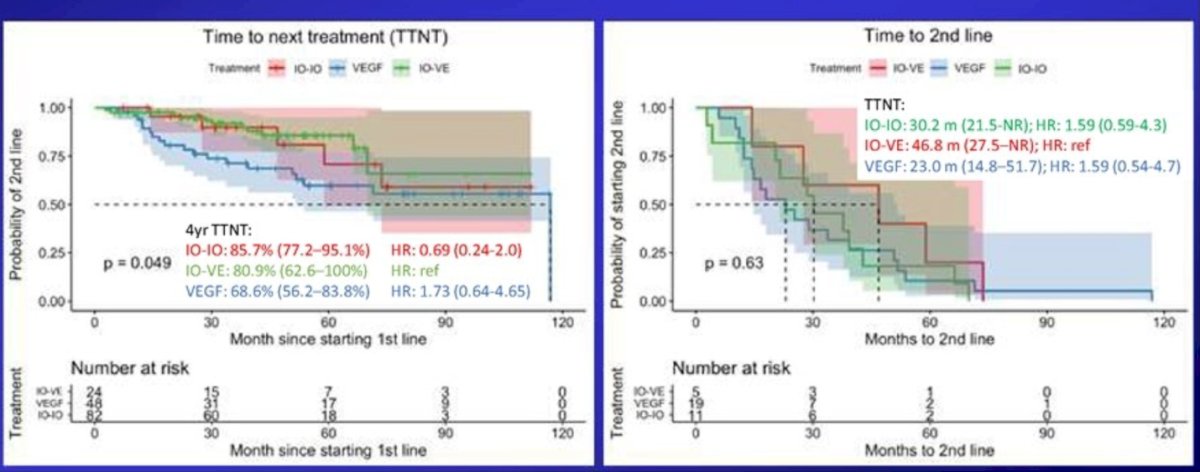
Regarding TTNT, patients treated with IO–IO achieved the most durable responses, with a 4-year TTNT rate of 85.7% compared to 80.9% for IO–VE and 68.6% for VEGF monotherapy (p=0.049). The median time to second-line therapy was longest for IO–VE (46.8 months) versus 30.2 months for IO–IO and 23.0 months for VEGF-based therapy, though these differences were not statistically significant.
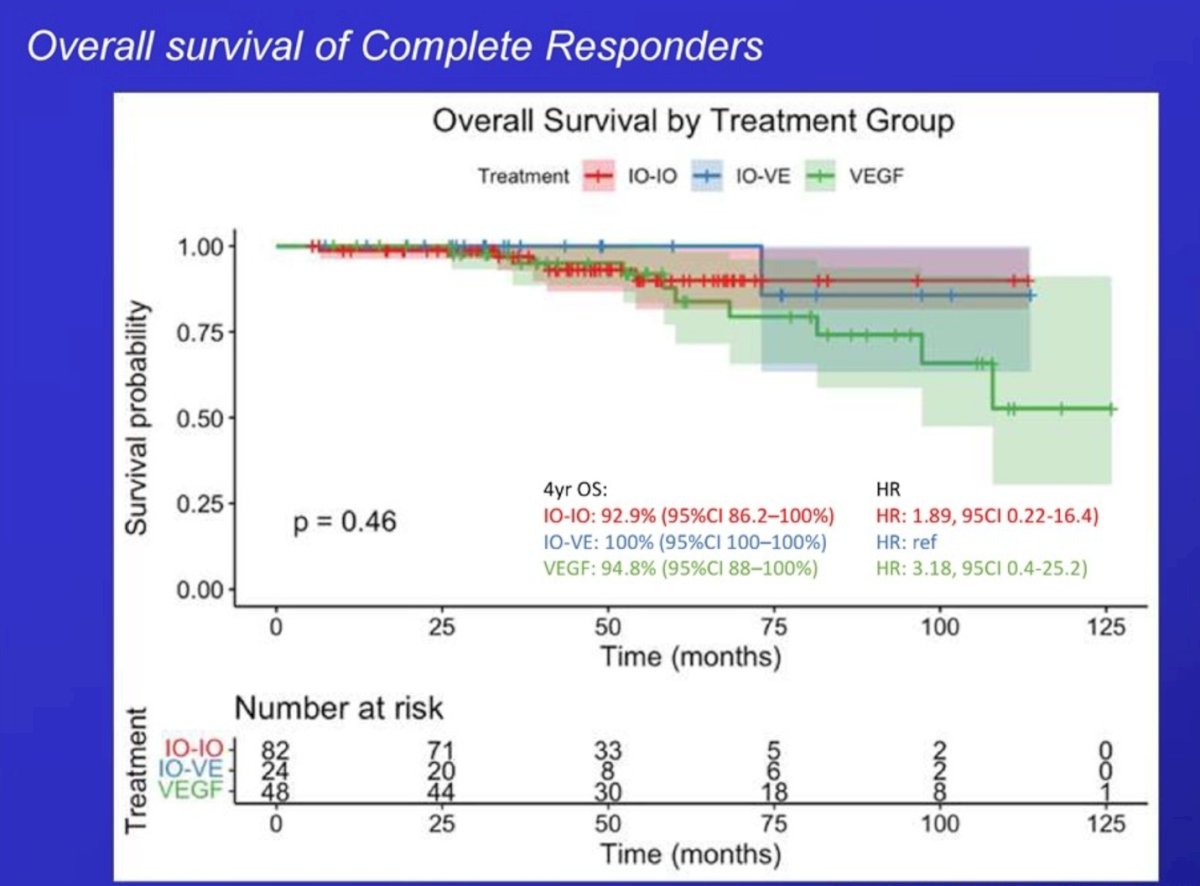
Lastly, overall survival among complete responders was excellent across all treatment groups. The 4-year OS rate was 92.9% for patients treated with IO–IO, 100% for those treated with IO–VE, and 94.8% for the VEGF monotherapy group (p=0.46). There were no statistically significant differences between groups, underscoring that patients achieving CR with any first-line regimen particularly IO-based combinations experienced durable survival outcomes.
Dr. Wells concluded by emphasizing the following key points:
- Achieving a complete response (CR) confers an excellent prognosis but does not equate to cure.
- Relapses may still occur among patients treated with Ipilimumab/Nivolumab or IO–VEGF combinations.
- Importantly, retreatment with immunotherapy may be effective for patients who experience disease progression after an initial CR.
Presented by: J. Connor Wells MD, Medical Oncologist at Arthur J.E. Comprehensive Cancer Centre, Alberta, Canada.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.