(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress was host to the session Mini Oral session 2: GU tumours, renal & urothelial. Dr. Ignacio Duran titled his discussion of abstracts 2595MO, 2600MO, 2610MO: Bringing any clarity into the non-clear or making things even darker?
Dr. Durán emphasized that non–clear cell RCC (nccRCC) accounts for only about 20–30% of all RCC cases, meaning that the majority of available evidence and clinical experience is derived from clear cell subtypes. These tumors, which include papillary, chromophobe, collecting duct, and other rare histologies, present unique molecular and biological features, often associated with poorer outcomes compared to clear cell RCC. However, as Dr. Durán noted, there remains a lack of robust evidence to guide treatment decisions for this heterogeneous and relatively small patient population seen in daily clinical practice.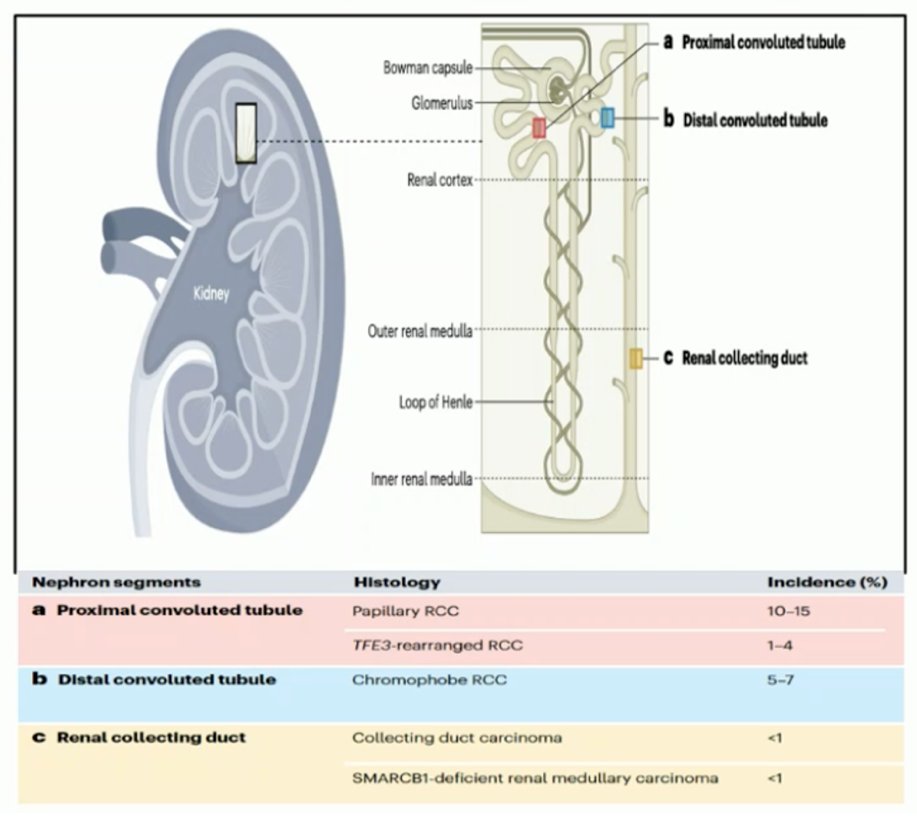
Dr. Durán highlighted that studies focusing on specific non–clear cell RCC populations remain scarce, as most clinical trials still group these heterogeneous subtypes under the generic label of “non-clear cell.” She emphasized that most biomarkers currently lack robust validation, and the role of cytoreductive nephrectomy in this setting remains uncertain. While molecular profiling has advanced, its clinical integration is still limited, underscoring the need for subtype-specific research and translational application to improve outcomes in this rare and diverse group of tumors.
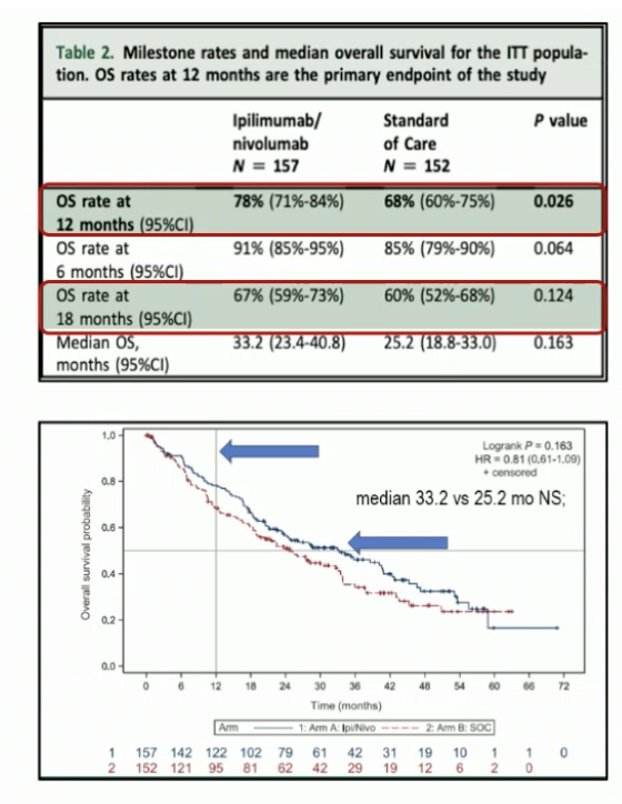
2595MO - Exploratory analysis of chromophobe renal cell carcinoma in the SUNNIFORECAST trial comparing Ipilimumab plus Nivolumab vs standard of care as first-line treatmentDr. Durán emphasized the importance of the SUNNIFORECAST trial as the first prospective study comparing ipilimumab plus nivolumab versus standard of care in nccRCC, demonstrating a 12-month OS benefit (78% vs 68%; p=0.026). He acknowledged the significant effort behind this trial but noted that the observed benefit diminished over time, as reflected in the Kaplan–Meier curves showing a trend favoring Ipi/Nivo (median OS 33.2 vs 25.2 months; HR 0.81) without reaching statistical significance. The study design is shown below.
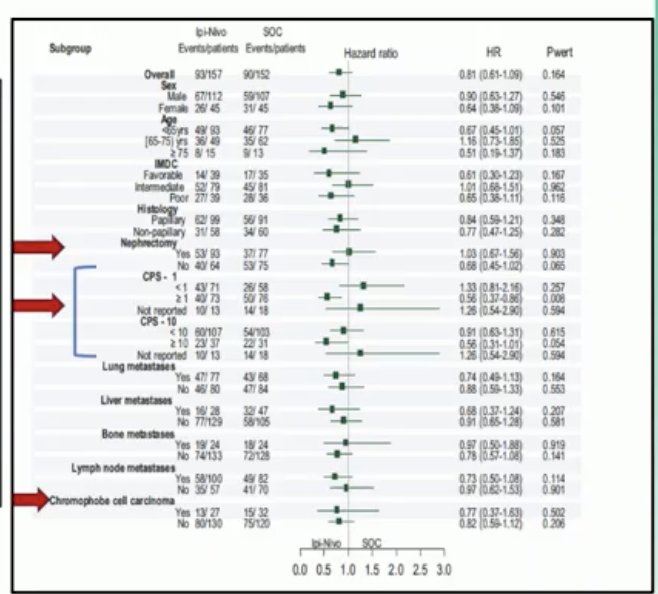
Dr. Durán noted that while the SUNNIFORECAST trial provided important prospective evidence in nccRCC, several critical questions remain unanswered. Among them are the role of PD-L1 expression as a potential predictive biomarker and the impact of prior nephrectomy on treatment outcomes. These are precisely the aspects the authors of the abstracts discussed today sought to explore, aiming to refine patient selection and deepen our understanding of immunotherapy efficacy across subgroups in non–clear cell RCC. Notably, as shown in the forest plot below, in the overall survival analysis, the PD-L1 CPS ≥1 subgroup tumors showed a significant survival benefit with immunotherapy.
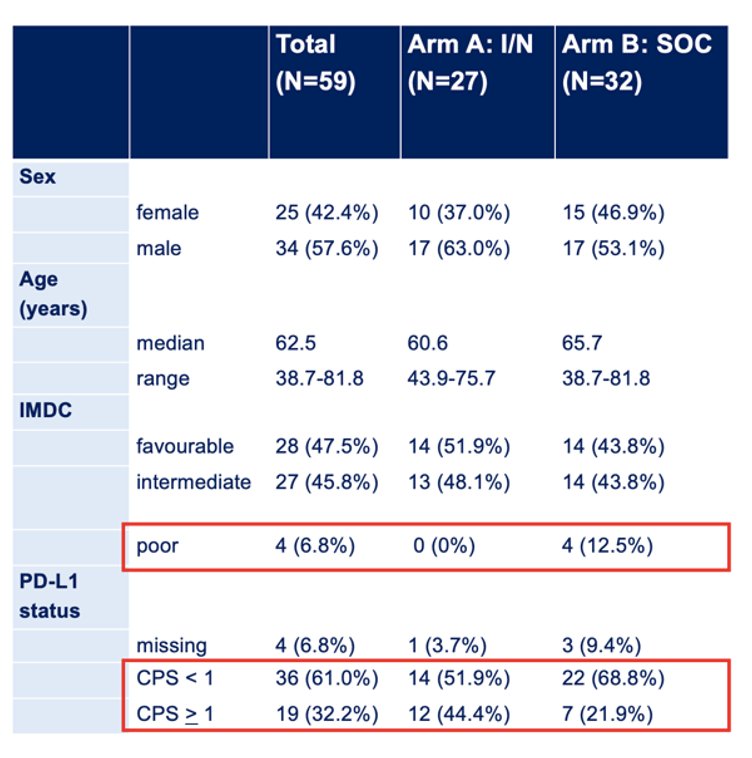
Dr. Durán emphasized the importance of having an expert pathologist involved, noting how crucial it is to identify dedifferentiated features within chromophobe tumors. He questioned where these tumors were classified and how their biology could impact outcomes. This exploratory subgroup analysis, designed to improve decision-making, included only 59 patients and showed imbalances in IMDC risk and PD-L1 status, potentially biasing results toward the Ipi/Nivo arm. Additional pathology analyses, focusing on dedifferentiation, necrosis, and eosinophilic subtypes, aimed to further separate “the good from the bad” tumors, but questions remain on how these were distributed between treatment arms. Although a 12-month OS benefit was observed for chromophobe tumors treated with Ipi/Nivo, the advantage was lost over time, showing no statistical significance, raising concerns about the robustness and predefined nature of this analysis.
 Dr. Durán emphasized that a detailed pathological review was critical in this analysis, as many tumors demonstrated dedifferentiation, necrosis, or eosinophilic features, elements that could significantly influence clinical behavior and treatment response. Among the 56 evaluable chromophobe RCC cases, 33.9% showed dedifferentiation and 28.6% necrosis, highlighting the biological heterogeneity of this subgroup. Eosinophilic tumors accounted for only 8.9% of cases, but their distribution across PD-L1 expression levels (CPS <1 vs ≥1) raises additional questions about their prognostic and predictive implications. This reinforces the need for accurate pathology and molecular stratification to guide therapy in such rare entities.
Dr. Durán emphasized that a detailed pathological review was critical in this analysis, as many tumors demonstrated dedifferentiation, necrosis, or eosinophilic features, elements that could significantly influence clinical behavior and treatment response. Among the 56 evaluable chromophobe RCC cases, 33.9% showed dedifferentiation and 28.6% necrosis, highlighting the biological heterogeneity of this subgroup. Eosinophilic tumors accounted for only 8.9% of cases, but their distribution across PD-L1 expression levels (CPS <1 vs ≥1) raises additional questions about their prognostic and predictive implications. This reinforces the need for accurate pathology and molecular stratification to guide therapy in such rare entities.
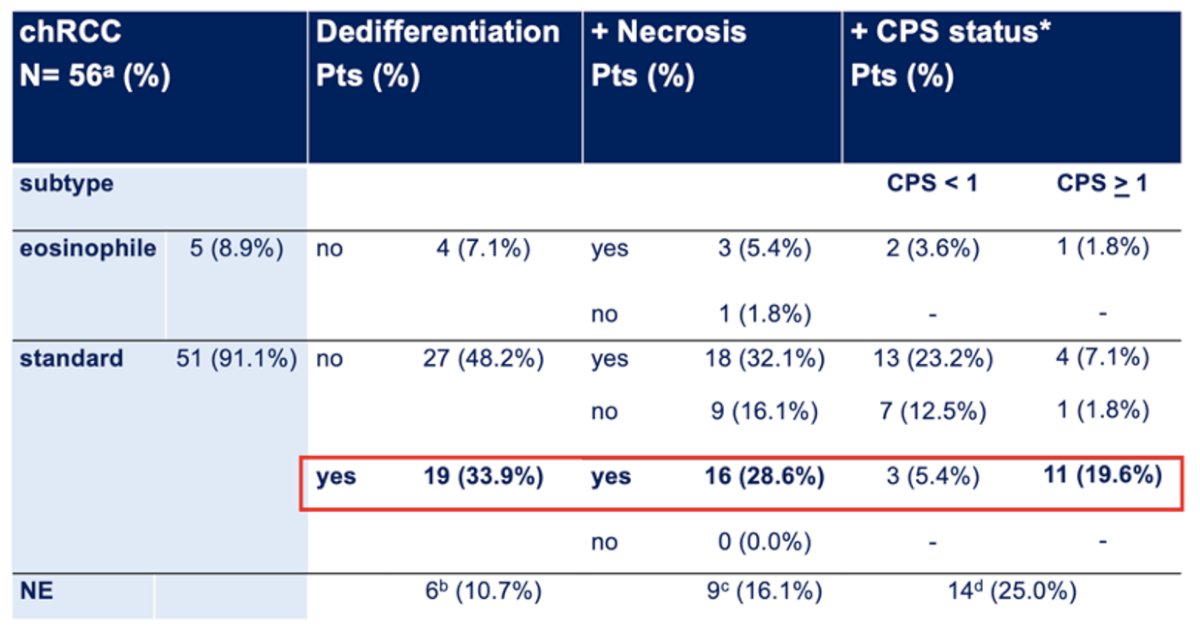
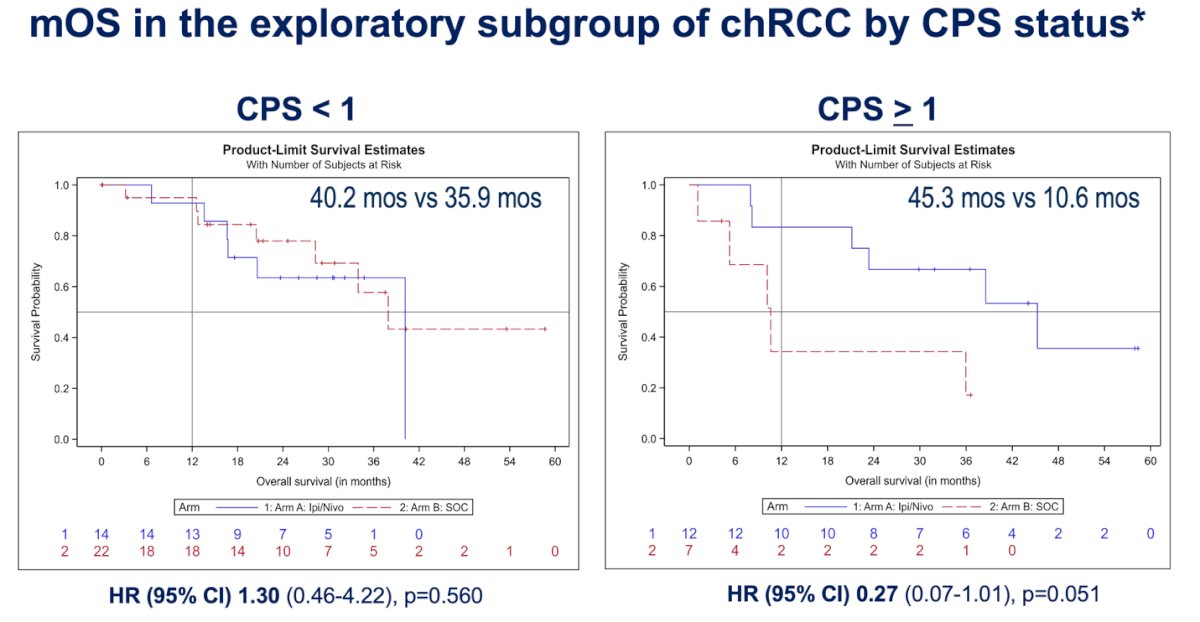
In the SUNNIFORECAST chromophobe RCC subgroup (n=59), CPS stratification suggested a potential signal favoring ipilimumab plus nivolumab when CPS ≥1 (mOS 45.3 vs 10.6 months; HR 0.27, p=0.051), while no benefit was observed in CPS <1 (mOS 40.2 vs 35.9 months; HR 1.30, p=0.56). However, this finding must be interpreted with caution given the small sample size, imbalances in IMDC and PD-L1 distribution, and the fact that the early OS advantage for Ipi/Nivo in chromophobe tumors dissipated over time with no statistical significance.
Additional pathology analyses incorporating dedifferentiation, necrosis, and eosinophilic subtypes aimed to distinguish “the good from the bad,” but their distribution across treatment arms was unclear, raising concern for bias. Ultimately, CPS may play a role in a subset of chromophobe tumors, yet the evidence remains exploratory and underpowered; importantly, PD-L1 testing using the Ventana SP263 assay is not standardized in RCC and should not guide current clinical practice.
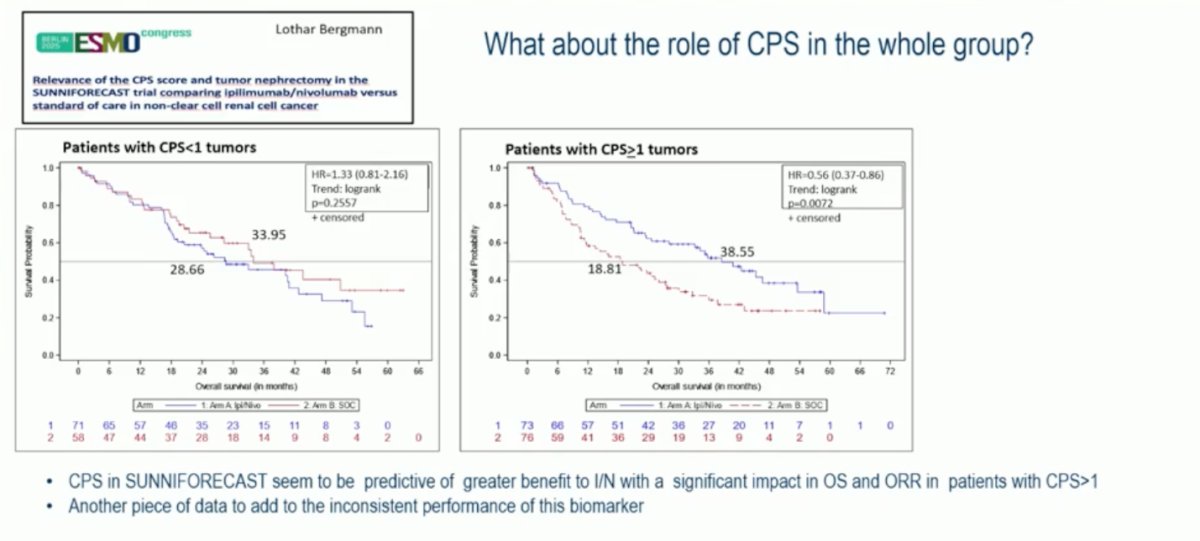
Dr. Duran moved on to discuss the study presented by Dr. Bergmann. Notably, CPS appeared to influence outcomes, with patients whose tumors expressed CPS ≥1 deriving greater benefit from ipilimumab plus nivolumab compared to standard of care (mOS 38.6 vs 18.8 months; HR 0.56, p=0.0072). In contrast, no difference was observed among patients with CPS <1 tumors (mOS 33.9 vs 28.7 months; HR 1.33, p=0.2557). These findings suggest that CPS may serve as a predictive marker of response to dual immune checkpoint blockade; however, given the variability across studies, this adds yet another piece of evidence to the inconsistent and context-dependent performance of CPS as a biomarker in RCC.
Dr. Durán emphasized the need to move toward pragmatic, biomarker-driven studies to refine patient selection and therapeutic strategies in RCC. The ongoing CARE-1 trial, led by Dr. Laurence Albiges, exemplifies this approach, stratifying treatment-naive clear cell mRCC patients by PD-L1 expression and IMDC risk group to directly compare ICI–ICI versus ICI–TKI combinations. Unfortunately, such efforts currently focus only on clear cell RCC, leaving a significant evidence gap for non-clear cell subtypes.

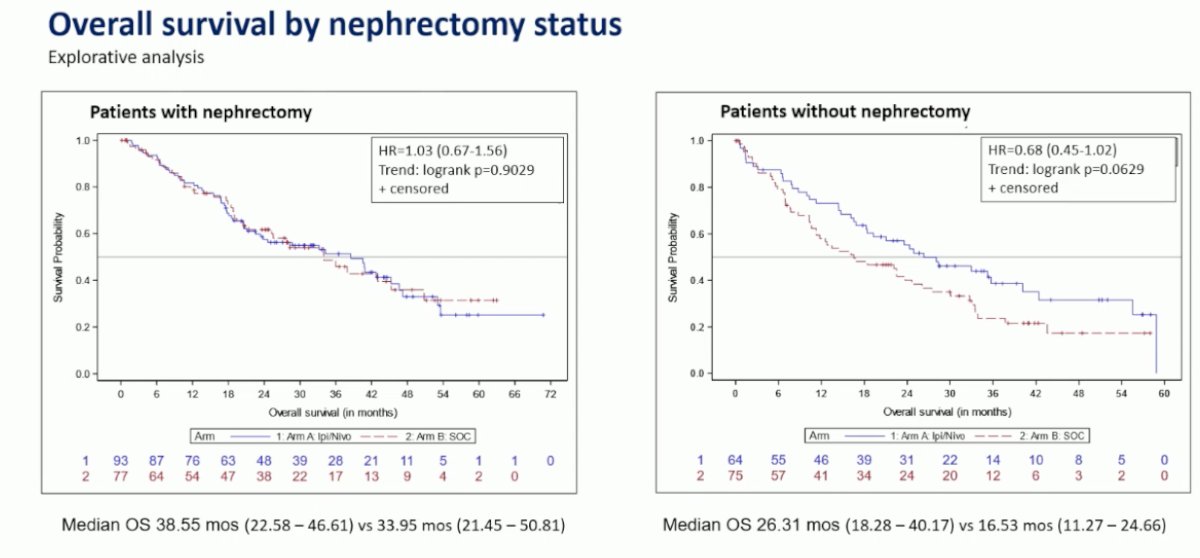
Dr. Durán noted that the exploratory analysis assessing nephrectomy status in SUNNIFORECAST remains purely hypothesis-generating. While a modest trend favoring ipilimumab plus nivolumab was observed in patients without prior nephrectomy (median OS 26.3 vs 16.5 months; HR 0.68, p=0.063), there was no benefit among those who underwent nephrectomy (median OS 38.6 vs 34.0 months; HR 1.03, p=0.90). Given the small sample size and lack of statistical significance, these findings should be interpreted cautiously, underscoring the need for larger prospective trials to clarify the true role of cytoreductive nephrectomy in non-clear cell RCC.
Dr. Durán concluded by noting that the question of nephrectomy in advanced RCC is still “being cooked.” Ongoing trials such as SWOG 1931/PROBE, NORDIC-SUN, and CYTOSHRINK are designed to address the optimal timing and value of cytoreductive surgery in the era of immune checkpoint inhibitors. These studies will help clarify whether nephrectomy should remain part of the therapeutic algorithm or if systemic therapy alone is sufficient for most patients.
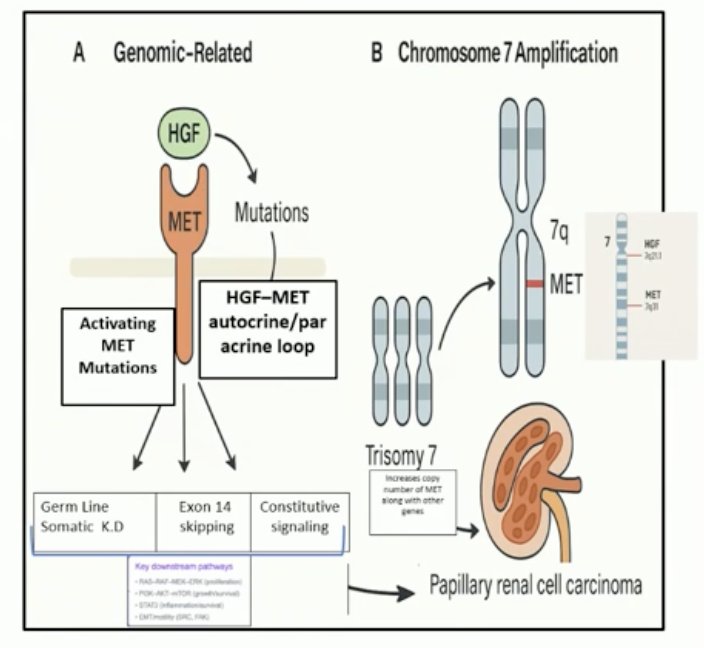
Dr. Durán discussed the abstract presented by Dr. Zugman, which focused on the particular molecular outcomes in papillary RCC. Chromosome 7 amplification was highlighted, noting that both MET and its ligand HGF are located on chromosome 7q31. He emphasized how relevant and frequent these genomic alterations are in real-world practice and the implications they hold for treatment, particularly considering ongoing drug development targeting the HGF–MET axis and the enrichment of MET-positive populations in clinical trials.
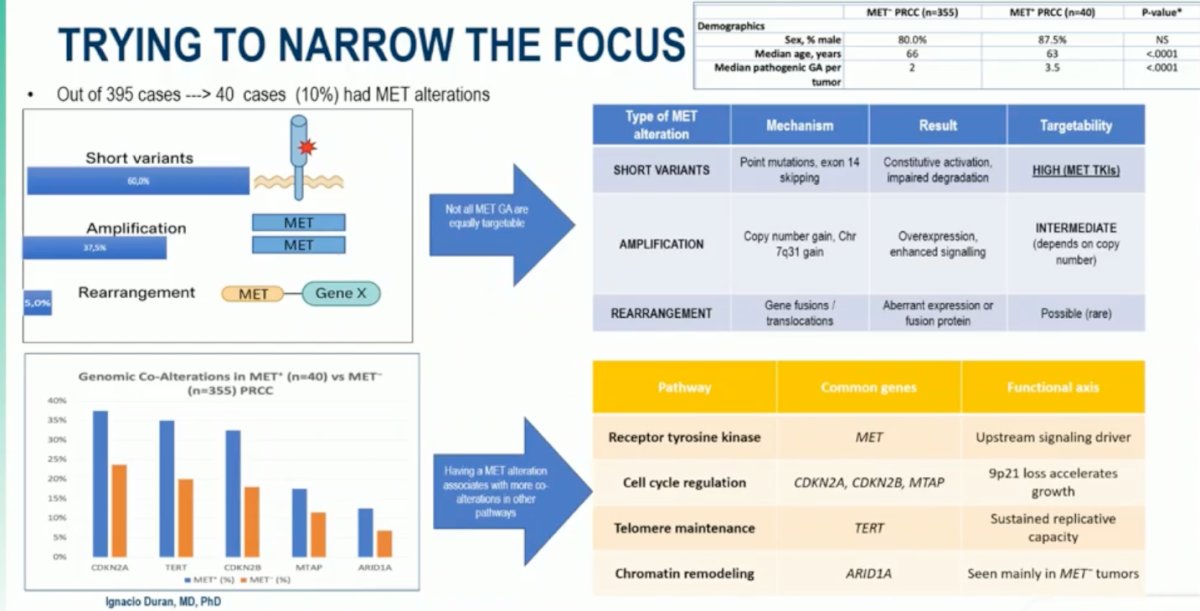
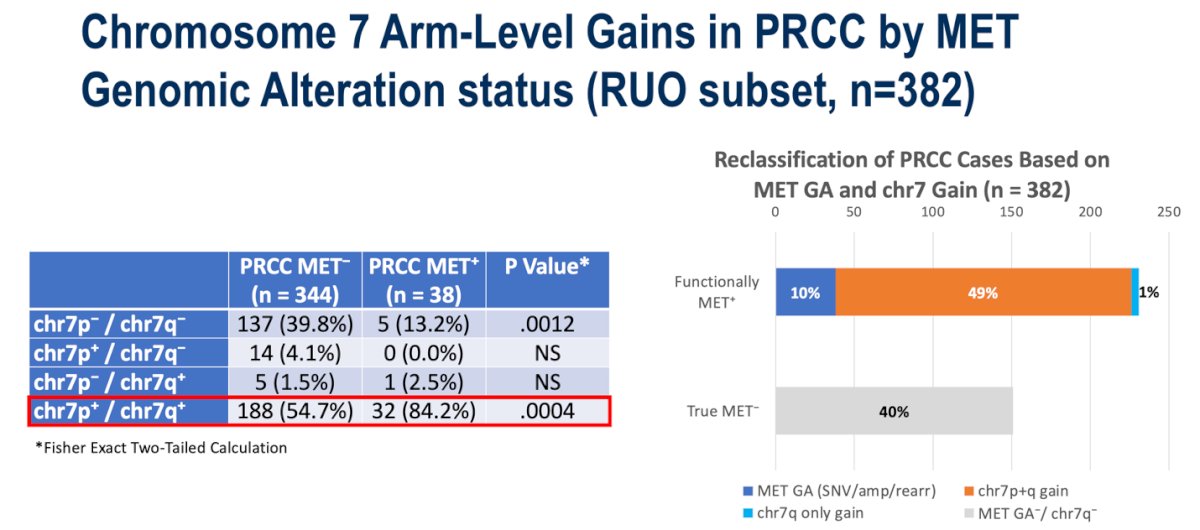
Out of 395 evaluated cases, 40 (10%) harbored MET alterations. Among these, short variants exclusively missense mutations were the most frequent, present in approximately 60% of MET⁺ tumors. MET amplifications accounted for 38% of cases, whereas rearrangements were rare, identified in only 5%. Interestingly, chromosome 7q gain was observed in both MET⁺ and MET⁻ papillary RCC tumors. While more frequent among MET⁺ cases, the key observation was that over half of MET⁻ tumors also demonstrated 7q gain, suggesting that this alteration alone may not fully explain MET pathway activation.
Dr. Durán emphasized that papillary RCCs may be more accurately classified by functional MET pathway activation rather than by raw mutation status. Only about 10% of tumors carry direct MET genomic alterations, while approximately half are functionally MET⁺ due to chromosome 7 gain. The remaining 40% are truly MET⁻, lacking both MET genomic alterations and 7q gain. This functional stratification appears clinically relevant, as prior studies have shown that selecting pRCC patients based on MET pathway activation (rather than just genetic alteration) most likely enriches for those who benefit from MET-targeted therapies, an approach that ongoing trials aim to further validate.
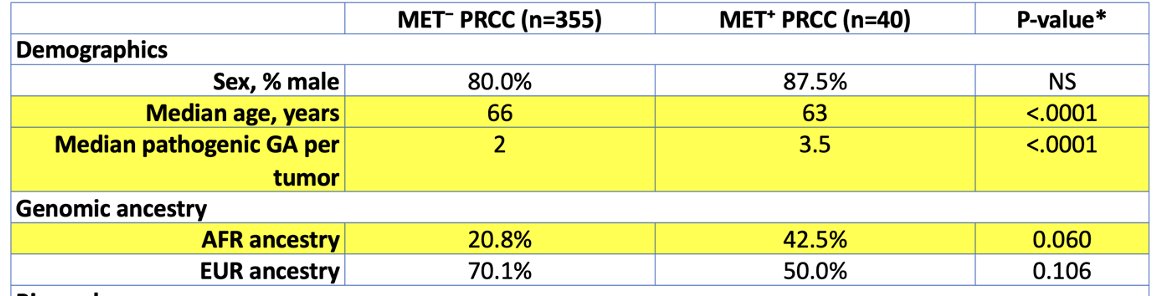
Dr. Durán highlighted the importance of considering genomic ancestry when evaluating MET alterations in papillary RCC. Genomic ancestry, derived from DNA variation, reflects biological lineage and should be distinguished from socially defined race or ethnicity. Data from TCGA pRCC (TCGA-KIRP) indicate an overall MET mutation rate of 13–15%, though the sample was small and predominantly of European ancestry, limiting meaningful ancestry-based comparisons.
A race-stratified analysis from Mount Sinai and MSKCC using TCGA data compared 58 Black and 58 White pRCC patients and found that MET alterations were not more frequent in Black patients; in fact, MET was not even among the limited set of genes showing differential expression or mutation. Similarly, the TCGA Pan-Cancer Ancestry Study, which analyzed over 10,000 tumors across 33 cancer types, identified ancestry-associated differences in renal cancers (such as lower VHL and PBRM1 mutation frequencies in African ancestry) but found no MET-related signal.1
Likewise, the MSK-IMPACT ancestry analysis,2 which included 953 RCC cases, did not report a higher rate of MET alterations in patients of African ancestry, and MET was not among the genes showing ancestry-associated somatic variation. Dr. Durán concluded by underscoring that while inclusion of diverse genomic data is critical to understanding disease biology, treatment strategies in pRCC should be guided by tumor genomics, specifically MET mutation, amplification, or chromosome 7 gain—rather than by race or ethnicity, as these molecular drivers, not ancestry, define true MET-driven disease and inform targeted therapy selection
Dr. Durán concluded his discussion with the following key take-home messages:
- No changes in current clinical practice can be inferred from the data presented today.
- Exploratory analyses should be interpreted with caution and regarded as hypothesis-generating.
- MET remains an appealing molecular target in papillary RCC, but it is not yet ready to guide treatment decisions until results from ongoing studies are available.
- There is a pressing need for specific, prospective studies in nccRCC requiring coordinated global efforts to advance the field.
Presented by: Ignacio Durán, MD, PhD, Hospital Universitario Marqués de Valdecilla; IDIVAL, Santander. Spain
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.
Reference:
- Paulucci DJ, Sfakianos JP, Skanderup AJ, Kan K, Tsao CK, Galsky MD, Hakimi AA, Badani KK. Genomic differences between black and white patients implicate a distinct immune response to papillary renal cell carcinoma. Oncotarget. 2017 Jan 17;8(3):5196-5205. doi: 10.18632/oncotarget.14122. PMID: 28029648; PMCID: PMC5354901.
- Kotecha RR, Knezevic A, Arora K, Bandlamudi C, Kuo F, Carlo MI, Fitzgerald KN, Feldman DR, Shah NJ, Reznik E, Hakimi AA, Carrot-Zhang J, Mandelker D, Berger M, Lee CH, Motzer RJ, Voss MH. Genomic ancestry in kidney cancer: Correlations with clinical and molecular features. Cancer. 2024 Mar 1;130(5):692-701. doi: 10.1002/cncr.35074. Epub 2023 Oct 21. PMID: 37864521; PMCID: PMC11220722.