(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to the session Mini Oral session 2: GU tumours, renal & urothelial. Dr. Lothar Bergmann presented 2600MO - Relevance of the CPS score and tumor nephrectomy in the SUNNIFORECAST trial comparing ipilimumab/nivolumab versus standard of care in non-clear cell renal cell cancer.
Dr. Bergmann opened his presentation by emphasizing that non-clear cell renal cell carcinomas (nccRCC) constitute a rare and heterogeneous group comprising more than 20 histologically and molecularly defined entities. He noted that clinical data in this setting remain limited, with a lack of large randomized trials contributing to ongoing uncertainty regarding optimal treatment recommendations. Currently, tyrosine kinase inhibitor (TKI) therapy, with or without immune checkpoint inhibitors (ICIs), is considered the standard of care for advanced nccRCC.
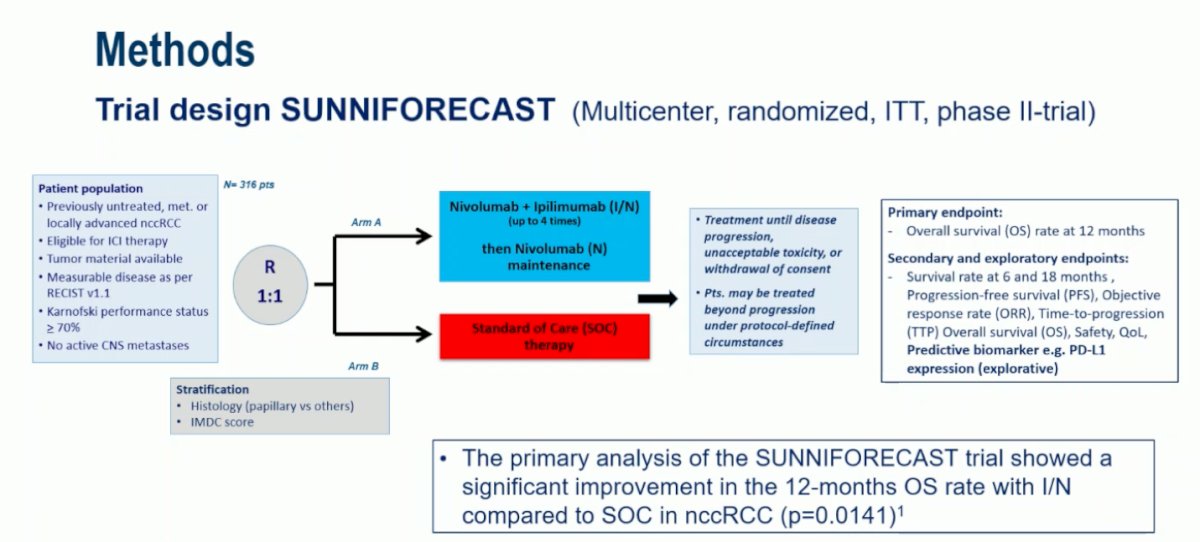
The SUNNIFORECAST trial (EudraCT 2016-000706-12; NCT03075423) was designed as a prospective, multicenter, randomized phase 2 study comparing ipilimumab/nivolumab (I/N) with standard of care (SOC) in treatment-naïve patients. The study design is shown below. Dr. Bergmann further highlighted that the clinical relevance of PD-L1 expression in RCC remains debated and is not routinely assessed, and that there are limited data evaluating the impact of nephrectomy status on the efficacy of I/N versus SOC in this population.
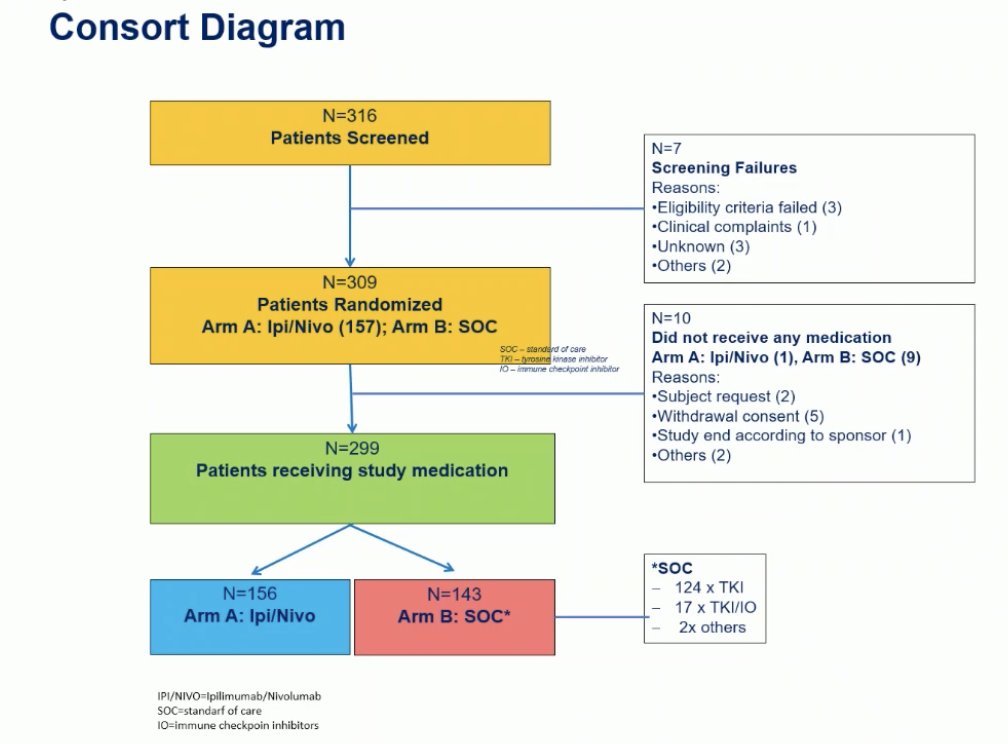
The SUNNIFORECAST trial enrolled more than 316 patients, of whom 309 were randomized to receive either ipilimumab/nivolumab (Ipi/Nivo n=157) or standard of care (SOC, n=152). After accounting for screening failures and withdrawals, a total of 299 patients received study medication: 156 in the Ipi/Nivo arm and 143 in the SOC arm. Among those in the SOC group, 124 received a tyrosine kinase inhibitor (TKI), 17 received a TKI in combination with an immune checkpoint inhibitor (IO), and 2 received other therapies.
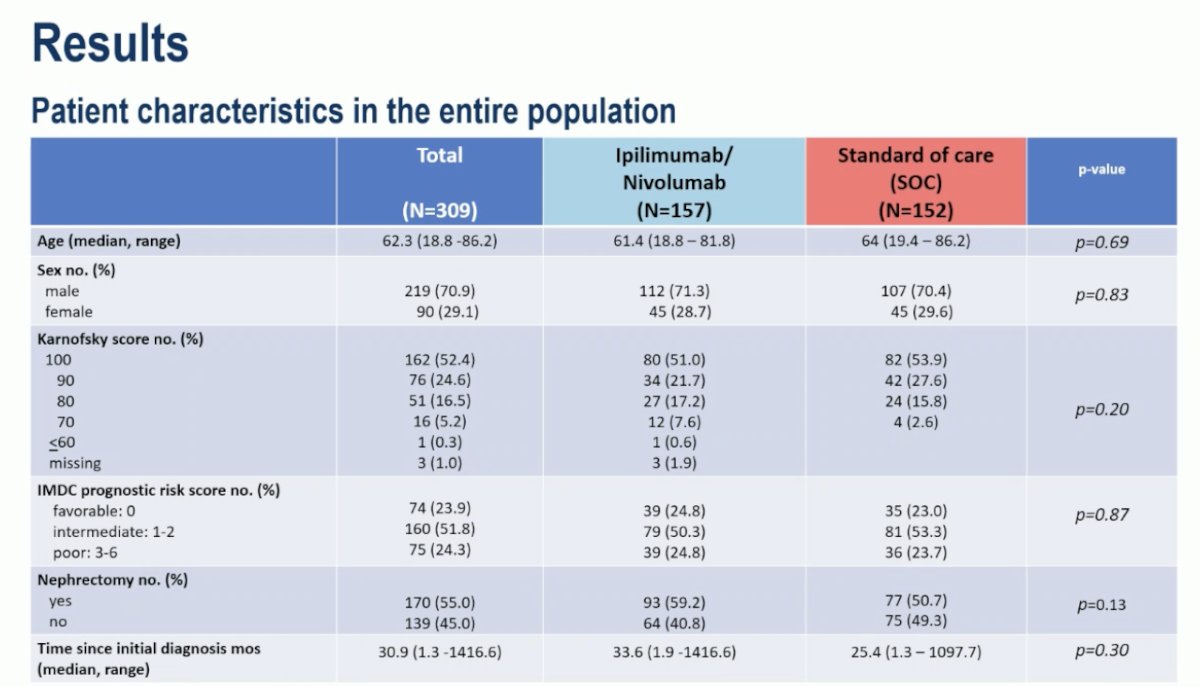
Patient characteristics were well balanced between the ipilimumab/nivolumab and standard of care arms. The median age was approximately 62 years, and most patients were male (around 71%). Baseline Karnofsky performance scores and IMDC prognostic risk categories were evenly distributed across both groups, as was the proportion of patients who had undergone prior nephrectomy (59.2% in the Ipi/Nivo arm vs 50.7% in the SOC arm). Similarly, histological subtypes were comparable between treatment arms, ensuring a well-matched study population for efficacy and safety analyses.
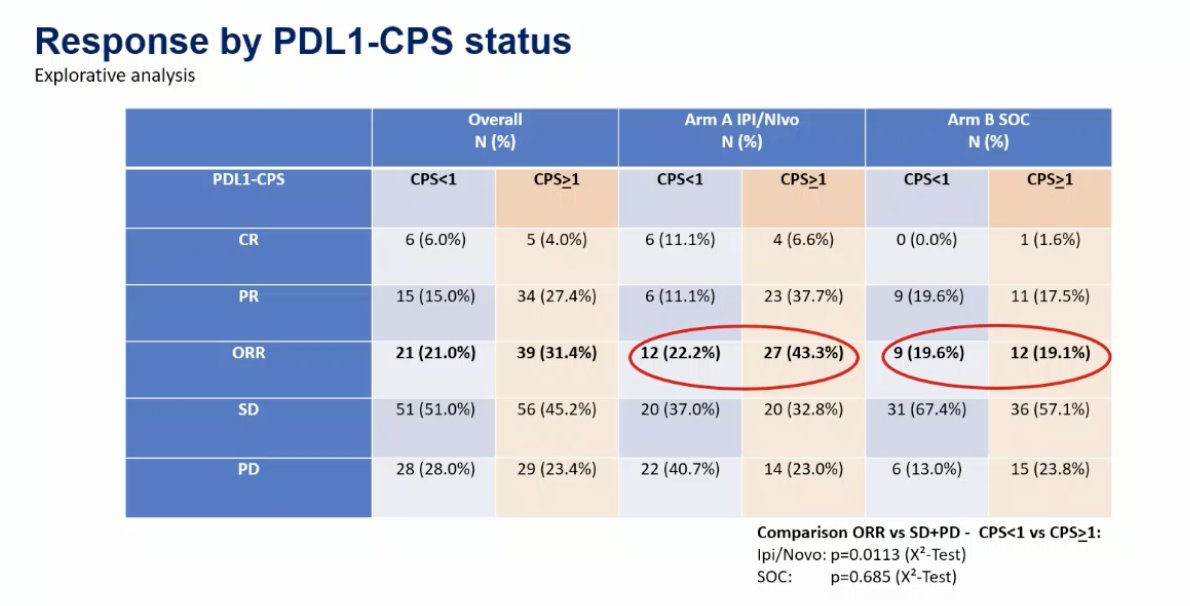
In the exploratory analysis evaluating response by PD-L1 combined positive score (CPS) status, no significant difference was observed in the SOC arm between patients with CPS <1 and those with CPS ≥1 (ORR 19.6% vs 19.1%, p=0.685). However, in the ipilimumab/nivolumab arm, patients with CPS ≥1 demonstrated a numerically higher objective response rate compared to those with CPS <1 (43.3% vs 22.2%, p=0.0113) as illustrated in the table below, suggesting potential predictive relevance of PD-L1 expression for response to immunotherapy in this cohort.
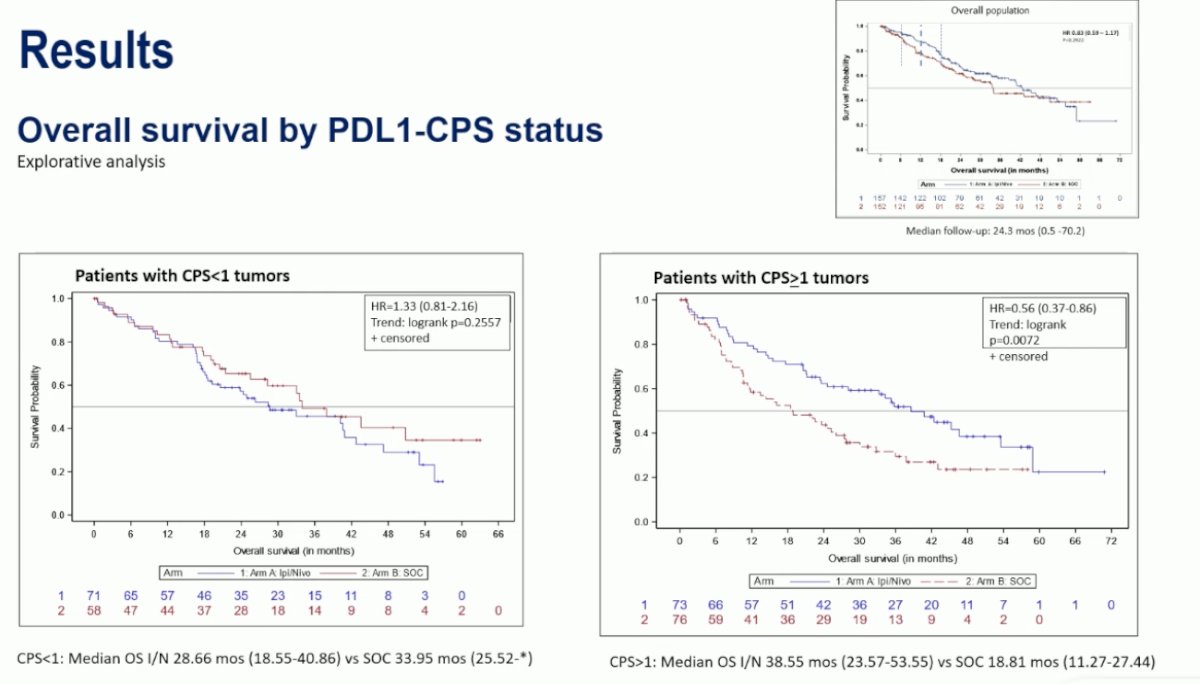
In the exploratory analysis of overall survival by PD-L1 CPS, patients with CPS ≥1 tumors showed a significant survival benefit with immunotherapy. Median OS was 38.6 months with ipilimumab/nivolumab compared to 18.8 months with standard of care (HR 0.56, 95% CI 0.37–0.86; p=0.0072).
Conversely, for patients with CPS <1 tumors, there was no significant difference between the two arms (median OS 28.7 vs 33.9 months; HR 1.33, 95% CI 0.81–2.16; p=0.26). These findings suggest that PD-L1 expression may serve as a potential predictive biomarker for response to immunotherapy in non–clear cell RCC.
Moreover, no significant difference was observed between treatment arms among patients who had undergone nephrectomy (median OS 38.6 months with ipilimumab/nivolumab vs 34 months with SOC; HR 1.03, 95% CI 0.67–1.56; p=0.90). However, among patients without nephrectomy, those treated with immunotherapy showed a trend toward improved survival compared to SOC (median OS 26.3 vs 16.5 months; HR 0.68, 95% CI 0.45–1.02; p=0.06). The decision to perform nephrectomy was largely influenced by IMDC risk, with poor-risk patients typically not recommended for cytoreductive nephrectomy, consistent with current clinical practice.

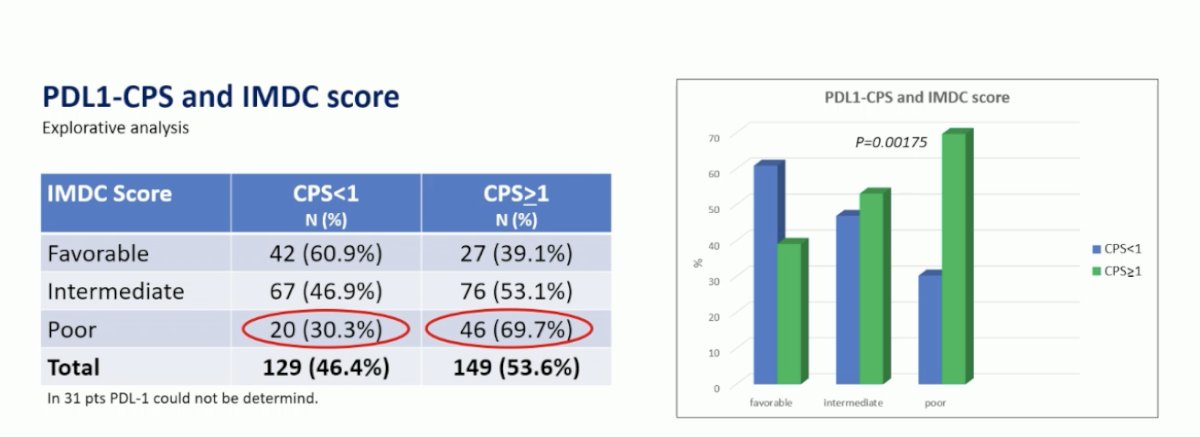
Lastly, Dr. Bergmann noted that a higher proportion of patients with poor IMDC risk were found among those with CPS ≥1 tumors (69.7% vs 30.3% for CPS <1, p=0.00175). He suggested that this imbalance could partly explain some of the differences observed in treatment outcomes, as PD-L1 positivity in this cohort was associated with a higher proportion of poor-risk disease.
Dr. Bergmann concluded his presentation with the following key take-home messages from this exploratory analysis of the SUNNIFORECAST trial:
- The primary endpoint of 12-month OS showed a significant benefit for ipilimumab + nivolumab versus SOC (78.3% vs 68.3%; p = 0.026).
- Median OS was 33.2 months vs 25.2 months (p = 0.163; HR 0.81 [0.61–1.099]).
- In patients with CPS ≥ 1, the 12-month OS rate was 83.5% with I/N versus 57.6% with SOC (p = 0.008).
- There was no significant difference in 12-month OS among patients with CPS < 1.
- Patients who underwent nephrectomy had longer and comparable survival across arms, while those without nephrectomy appeared to derive greater benefit from I/N versus SOC.
- PD-L1 expression increased with higher IMDC scores, as shown in exploratory analyses.
Presented by: Lothar Bergmann, MD, Department of Hematology and Oncology, University Hospital Frankfurt, Goethe University Frankfurt am Main, Frankfurt, Germany
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025