(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between October 17th and 21st was host to the session Mini Oral session 2: GU tumours, renal & urothelial. Dr. Marit Ahrens presented 2595MO - Exploratory analysis of chromophobe renal cell carcinoma in the SUNNIFORECAST trial comparing Ipilimumab plus Nivolumab vs standard of care as first-line treatment.
Dr. Ahrens opened the presentation by noting that chromophobe renal cell carcinoma (chRCC) accounts for approximately 5% of all RCC cases, making it the second most common subtype among non–clear cell RCCs. These tumors are typically diagnosed at a favorable pathological stage and are associated with a lower risk of progression or metastasis, as well as longer overall survival.1,2 However, treatment outcomes in the metastatic setting remain poor. Previous studies have shown only modest benefit from tyrosine kinase inhibitors (TKIs) and inconsistent results with immune checkpoint inhibitors (ICIs).3-8 Current clinical guidelines therefore recommend treatment strategies analogous to those used for clear cell RCC, often involving TKI ± mTOR inhibition.9 Against this background, the investigators presented an exploratory analysis from the SUNNIFORECAST trial, aimed at refining therapeutic decision-making for patients with chRCC.
The trial design of SUNNIFORECAST is shown below. This multicenter, randomized, investigator-initiated phase II trial enrolled patients with previously untreated metastatic or locally advanced non–clear cell renal cell carcinoma eligible for immune checkpoint inhibitor therapy and measurable disease per RECIST v1.1. Patients were stratified by histology and IMDC risk score and randomized 1:1 to receive nivolumab plus ipilimumab followed by nivolumab maintenance or standard of care. The primary endpoint was overall survival at 12 months, with secondary endpoints including progression-free survival, objective response rate, time-to-progression, safety, and quality of life.
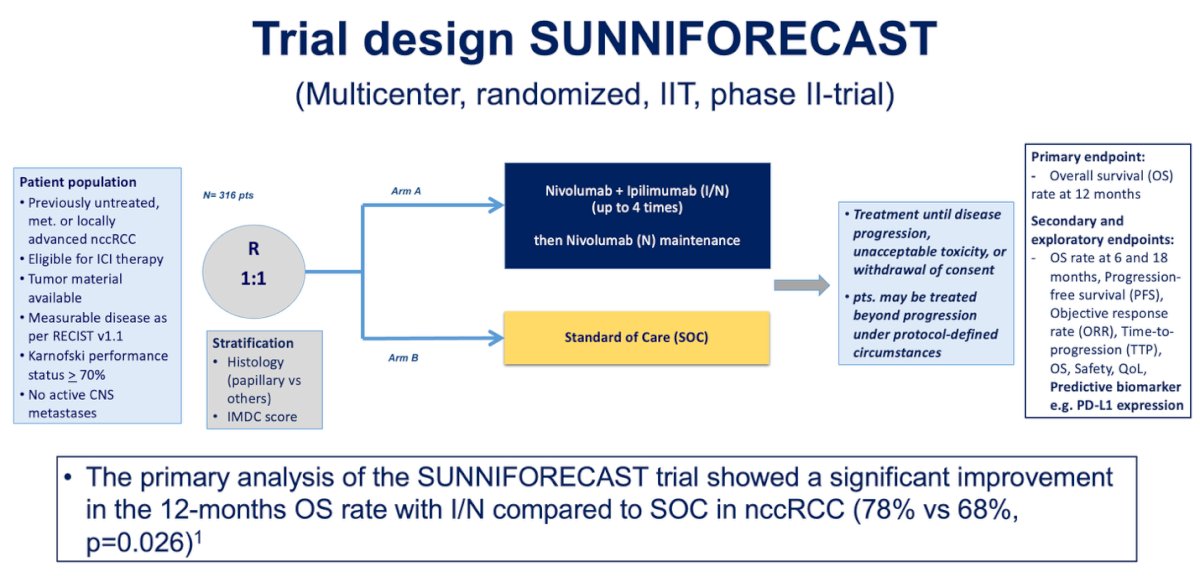
The primary analysis, presented at last year’s ESMO meeting, showed a significant improvement in 12-month overall survival with nivolumab plus ipilimumab compared to standard of care (78% vs 68%, p=0.026
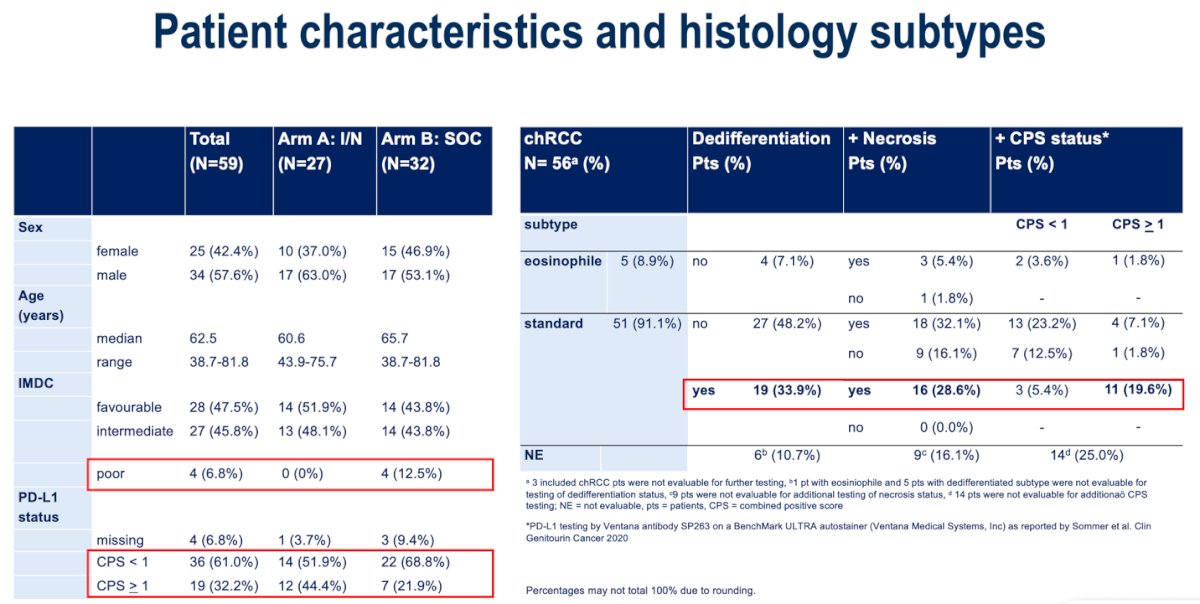
Patient characteristics are summarized below. The majority of participants were male, with a median age of approximately 62 years. Only 6.8% of patients had poor-risk disease by IMDC criteria, and most cases (around 91%) were of the standard chromophobe subtype. Dedifferentiation and necrosis were observed in 33.9% and 28.6% of patients, respectively. Regarding PD-L1 expression, 61% of patients had a combined positive score (CPS) below 1, reflecting a predominantly PD-L1–negative cohort.
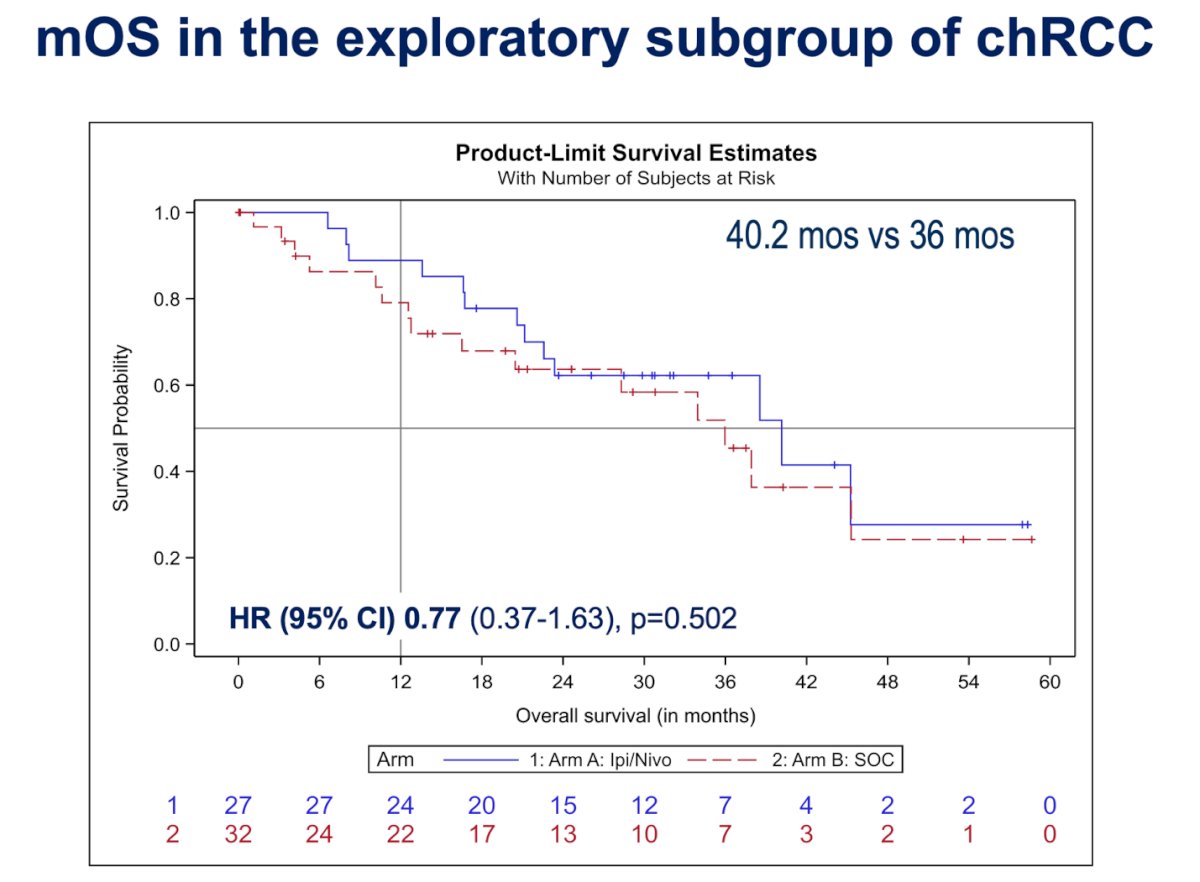
Dr. Ahrens highlighted that in the exploratory subgroup of chRCC, there was no statistically significant difference in median overall survival between treatment arms, with 40.2 months in the nivolumab plus ipilimumab group compared to 36 months in the standard-of-care arm (HR 0.77; 95% CI, 0.37–1.63; p=0.502). When stratified by IMDC risk, patients with favorable risk had a median OS of 44.3 months with Ipi/Nivo versus not estimable in the SOC group, while those with intermediate or poor risk had a median OS of 21.2 months versus 36 months, respectively. Although not statistically significant, the trend favored the experimental arm.
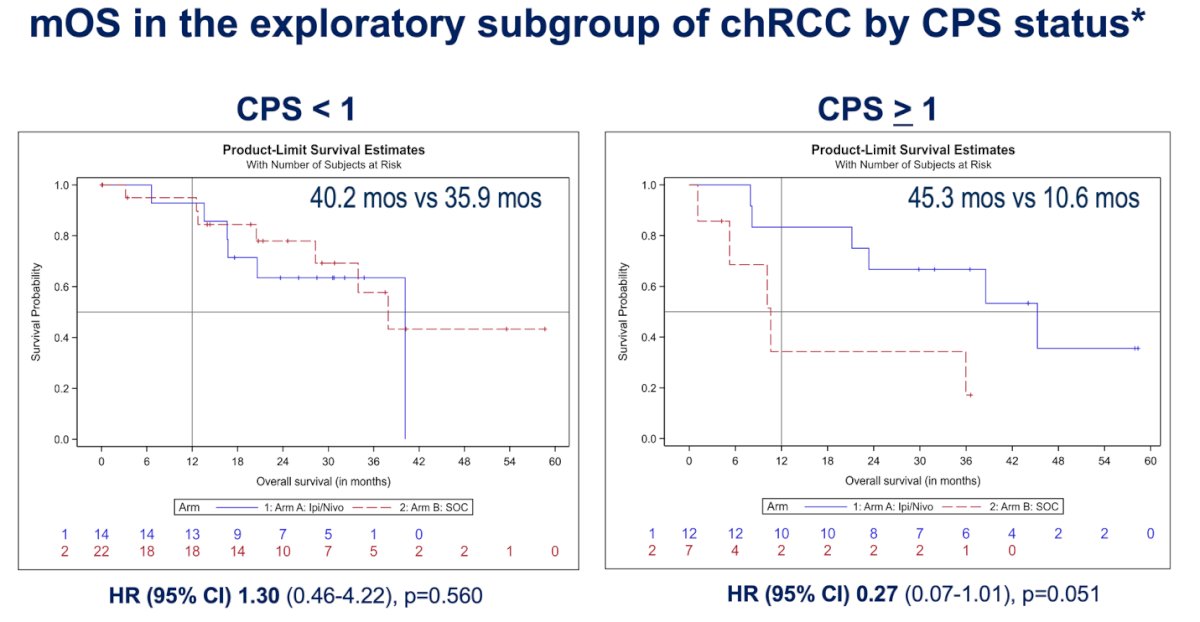
In the exploratory subgroup analysis of chRCC by PD-L1 CPS status, there was a trend favoring nivolumab plus ipilimumab for overall survival. Among patients with CPS <1, median OS was 40.2 months with Ipi/Nivo versus 35.9 months with standard of care (HR 1.30; 95% CI, 0.46–4.22; p=0.560).
In contrast, patients with CPS ≥1 showed a more pronounced separation of survival curves, with median OS of 45.3 months for Ipi/Nivo compared to 10.6 months for SOC (HR 0.27; 95% CI, 0.07–1.01; p=0.051). Although not statistically significant, these findings suggest that PD-L1 expression may enrich for patients more likely to benefit from immunotherapy in the chromophobe RCC population.
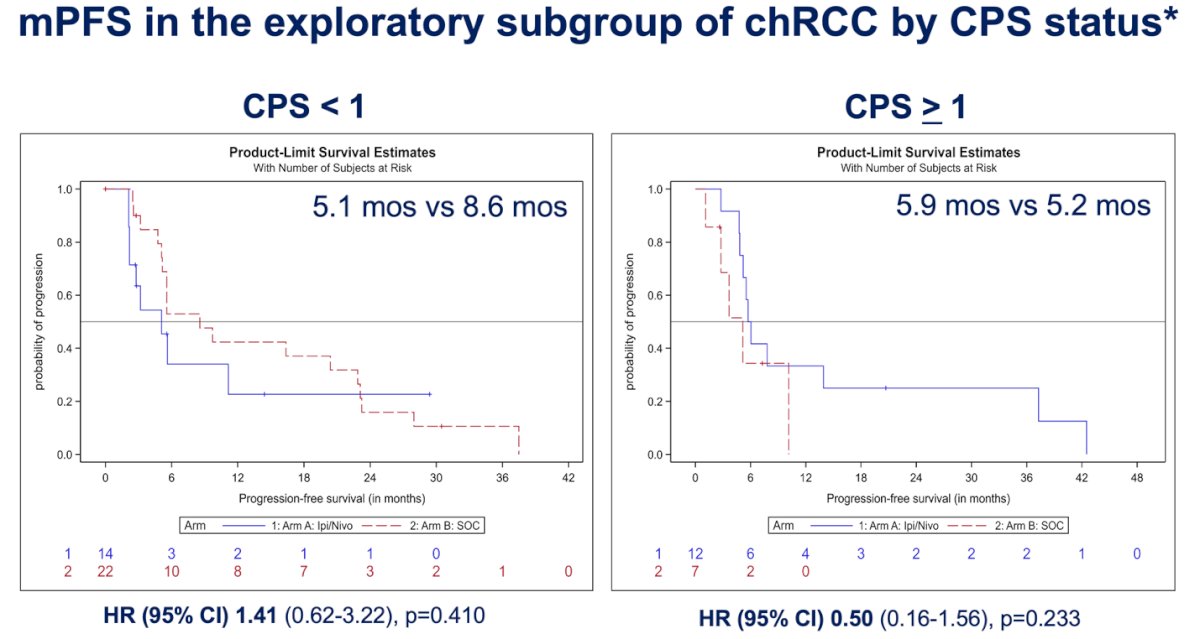
Similarly, the analysis of median progression-free survival (mPFS) in the exploratory chRCC subgroup stratified by PD-L1 CPS status showed no significant differences between treatment arms. Among patients with CPS <1, mPFS was 5.1 months with nivolumab plus ipilimumab versus 8.6 months with standard of care (HR 1.41; 95% CI, 0.62–3.22; p=0.410). In those with CPS ≥1, mPFS was 5.9 months versus 5.2 months, respectively (HR 0.50; 95% CI, 0.16–1.56; p=0.233).
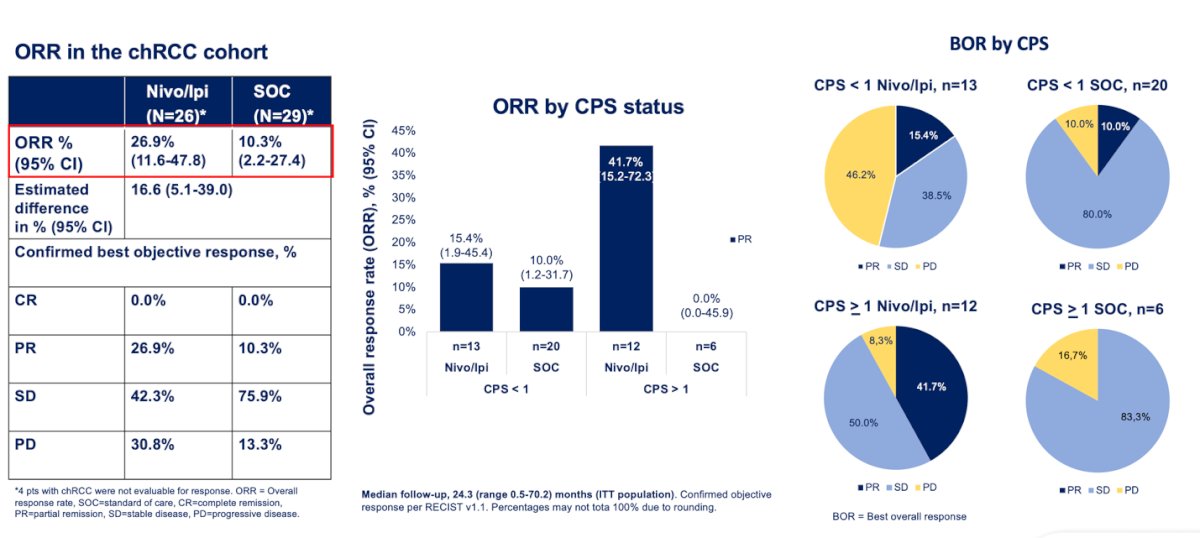
Finally, when evaluating the objective response rate (ORR) in the chromophobe RCC cohort, patients treated with nivolumab plus ipilimumab achieved an ORR of 26.9% (95% CI, 11.6–47.8) compared to 10.3% (95% CI, 2.2–27.4) in the standard-of-care arm, with no complete responses observed. When stratified by PD-L1 CPS status, patients with CPS >1 demonstrated a higher response rate, with 41.7% responding in the experimental arm compared to 0% in the SOC arm. This suggests that PD-L1 expression may enrich for potential benefit from immune checkpoint blockade in chromophobe RCC
Dr. Ahrens concluded her presentation by noting that this exploratory analysis of the chRCC cohort in SUNNIFORECAST:
- Showed a numerically, but not significantly, better median OS with nivolumab plus ipilimumab compared to standard of care (40.2 vs 36 months; HR 0.77, p=0.502).
- Nearly 34% of patients had dedifferentiated histology, consistent with sarcomatoid features.
- Patients with CPS >1:
- Demonstrated a trend toward improved survival (HR 0.27; 95% CI, 0.07–1.01) and prolonged median OS (45.3 vs 10.6 months) favoring nivolumab/ipilimumab over SOC.
- Achieved a higher ORR (partial response 41.7% vs 0%; no complete responses) with I/N compared to SOC.
- Patients with CPS <1:
• Showed a trend toward longer median PFS when treated with SOC (8.6 vs 5.1 months; p=0.410). - These findings support the role of immune checkpoint inhibitor–based therapy in chromophobe RCC and suggest PD-L1 testing may have value in guiding treatment decisions for this subgroup.
Presented by: Marit Ahrens, MD, Department of Hematology and Oncology, University Hospital Frankfurt, Goethe University Frankfurt am Main, Frankfurt, Germany
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.
References:
- Beck SDW, Patel MI, Snyder ME, Kattan MW, Motzer RJ, Reuter VE, Russo P. Effect of papillary and chromophobe cell type on disease-free survival after nephrectomy for renal cell carcinoma. Ann Surg Oncol. 2004;11(1):71–77.
- Volpe A, Novara G, Antonelli A, Bertini R, Billia M, Carmignani G, et al. Chromophobe renal cell carcinoma (RCC): oncological outcomes and prognostic factors in a large multicentre series. BJU Int. 2012;110(1):76–83.
- Tannir NM, Plimack E, Ng C, Tamboli P, Bekele BN, Xiao L, et al. A phase 2 trial of sunitinib in patients with advanced non–clear cell renal cell carcinoma. Eur Urol. 2012;62(6):1013–1019.
- Matrana MR, Baiomy A, Campbell MT, Shetty A, Teegavarapu P, Tannir NM. Outcomes of patients with chromophobe renal cell carcinoma treated with targeted therapy. Clin Genitourin Cancer. 2017;15(2):e205–e208.
- Martínez Chanzá N, Xie W, Asim B, et al. Cabozantinib in advanced non–clear-cell renal cell carcinoma: A multicentre, retrospective, cohort study. Lancet Oncol. 2019;20(4):581–590.
- Lee CH, Voss MH, Carlo MI, Chen YB, Xu W, Patil S, et al. Phase II trial of cabozantinib in patients with advanced non–clear cell renal cell carcinoma and clear cell renal cell carcinoma with sarcomatoid differentiation. J Clin Oncol. 2022;40(21):2333–2341.
- Albiges L, Powles T, Staehler M, Bex A, Choueiri TK, Grünwald V, et al. Nivolumab plus cabozantinib versus sunitinib for first-line treatment of advanced renal cell carcinoma: extended follow-up from CheckMate 9ER. Lancet Oncol. 2023;24(8):881–891.
- Tykodi SS, Geynisman DM, Choueiri TK, et al. Nivolumab monotherapy or combination therapy in patients with non–clear cell renal cell carcinoma: Results from CheckMate 920. J Immunother Cancer. 2022;10(2):e003844.
- Motzer RJ, Jonasch E, Agarwal N, et al. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Kidney Cancer. Version 1.2026. July 24, 2025.
- Powles T, Escudier B, Porta C, Bex A, Motzer RJ, Grünwald V, et al. ESMO Clinical Practice Guidelines: Renal cell carcinoma. Ann Oncol. 2024;35(8):692–706.