(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between October 17th and 21st was host to the session Mini Oral session 2: GU tumours, renal & urothelial Dr. Wenxin Xu presented abstract 2594MO - Association of circulating kidney injury molecule-1 (KIM-1) levels with clinical outcomes in advanced renal cell carcinoma (aRCC): Retrospective analysis of COSMIC-313.
Dr. Xu began by highlighting that kidney injury molecule-1 (KIM-1) is a transmembrane protein markedly overexpressed in clear cell renal cell carcinoma (ccRCC) and has emerged as a circulating biomarker with potential applications in early detection, risk stratification, and monitoring for disease recurrence.
In CheckMate-214, an early reduction in circulating KIM-1 levels at three weeks correlated with long-term efficacy among patients treated with first-line immunotherapy (nivolumab plus ipilimumab), but not with VEGFR TKI therapy (sunitinib).1 In the phase 3 COSMIC-313 trial, first-line treatment with cabozantinib plus nivolumab and ipilimumab significantly improved progression-free survival compared to placebo plus nivolumab and ipilimumab in patients with intermediate- or poor-risk advanced ccRCC, while overall survival outcomes were similar between arms. In this context, the investigators evaluated the association between circulating KIM-1 levels and clinical outcomes in COSMIC-313.2
For this analysis, plasma samples were collected at predefined time points: baseline (Week 1, Day 1), Weeks 4, 7, 10, and 14 and analyzed for KIM-1 levels using an enzyme-based electrochemiluminescence assay as shown below. The study design allowed longitudinal assessment of biomarker dynamics during combination immunotherapy (nivolumab + ipilimumab, with or without cabozantinib). The investigators evaluated the relationship between circulating KIM-1 levels and key clinical parameters, including baseline patient and disease characteristics, tumor response, progression-free survival (PFS), and overall survival (OS).
Notably, the investigators examined the relationship between baseline KIM-1 levels and key clinical variables. Baseline concentrations were comparable between treatment arms (nivolumab + ipilimumab vs cabozantinib + nivolumab + ipilimumab). However, patients classified as poor-risk by IMDC criteria, those without prior nephrectomy, and individuals with a greater total sum of target lesion diameters demonstrated significantly higher baseline KIM-1 levels (p < 0.001 across all comparisons) as illustrated below.

Moreover, higher baseline circulating KIM-1 levels were associated with worse OS across both treatment cohorts (Figure Below). When stratified by quartiles of baseline KIM-1 concentration, patients in the highest quartile (Q4) experienced inferior OS compared with those in lower quartiles, both in the nivolumab + ipilimumab arm and in the cabozantinib + nivolumab + ipilimumab triplet arm.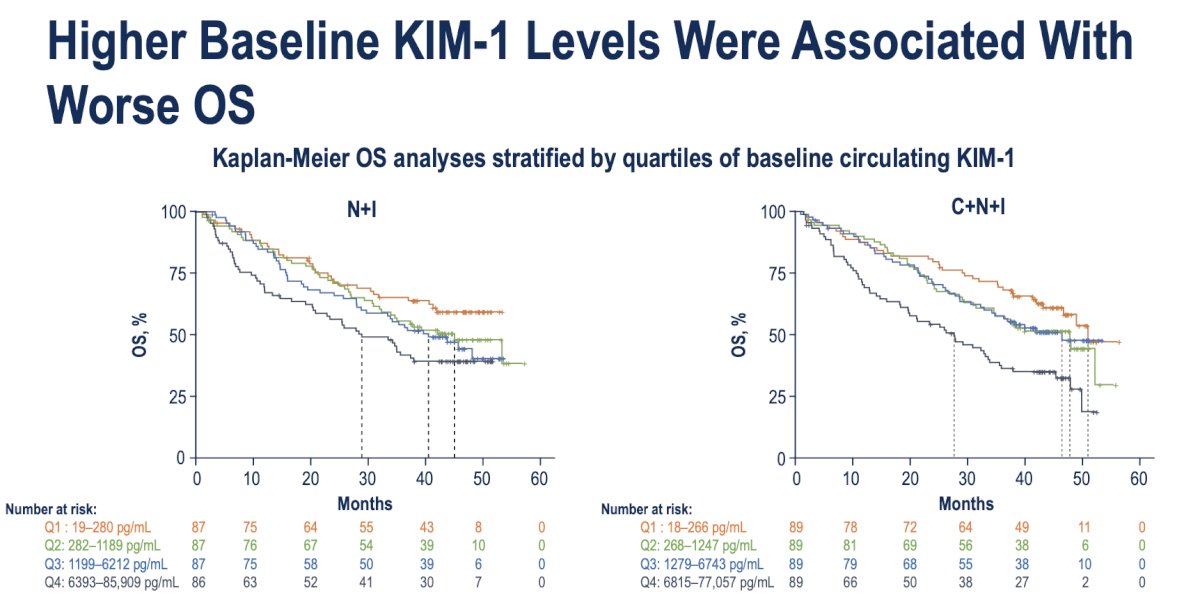
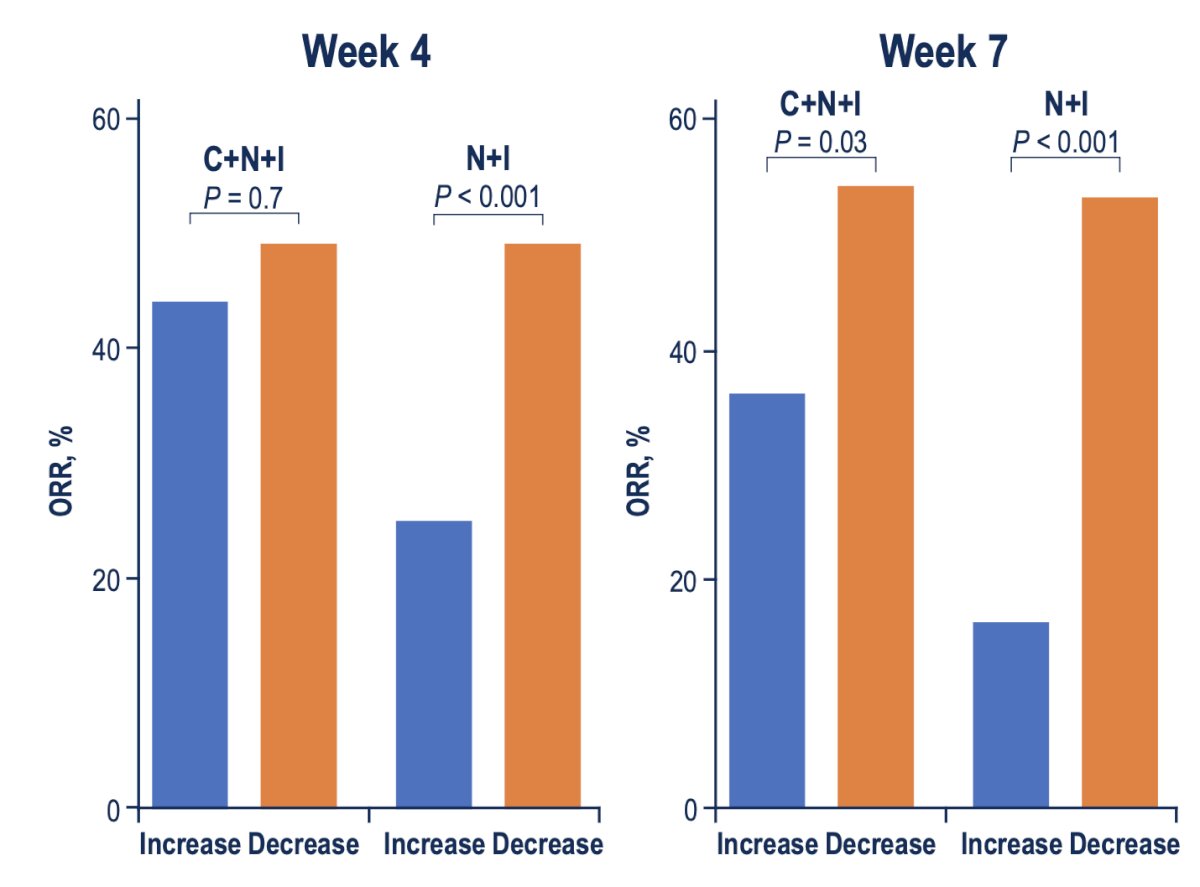
A decline in circulating KIM-1 levels from baseline was associated with improved treatment response. In patients treated with nivolumab plus ipilimumab, a significant association was observed between KIM-1 reduction and higher objective response rates (ORR) at both Week 4 and Week 7 (p < 0.001). Among those receiving the triplet regimen of cabozantinib, nivolumab, and ipilimumab, this association became evident at Week 7 (p = 0.03).
Furthermore, looking at time-to-event outcomes, reductions in KIM-1 levels over time were associated with improved PFS across both treatment arms, as shown in the table below. In patients receiving nivolumab plus ipilimumab, a decrease in KIM-1 at Weeks 4, 7, 10, and 14 was strongly associated with longer PFS (all p < 0.01) and OS Similarly, in the cabozantinib, nivolumab, and ipilimumab arm, KIM-1 decline correlated with better PFS at Weeks 7, 10, and 14, but not with OS. These findings suggest that early and sustained reductions in KIM-1 may serve as a pharmacodynamic biomarker of therapeutic efficacy, reflecting treatment-driven tumor regression and improved disease control.

Lastly, Dr. Xu highlighted that decreases in circulating KIM-1 levels at Week 7 were closely associated with reductions in target lesion size among patients treated with nivolumab plus ipilimumab. Most patients demonstrating radiographic tumor shrinkage also exhibited a corresponding decline in KIM-1, reinforcing its potential as a dynamic biomarker of on-treatment response.

Dr. Xu concluded the presentation with the following key takeaways:
- Patients with higher baseline KIM-1 levels typically presented with greater tumor burden, IMDC poor-risk features, and were less likely to have undergone prior nephrectomy.
- Among those treated with nivolumab plus ipilimumab, a decrease in KIM-1 levels from baseline was significantly associated with improved objective response rate, progression-free survival, and overall survival.
- The association between KIM-1 dynamics and clinical outcomes was less pronounced in patients receiving the triplet regimen of cabozantinib, nivolumab, and ipilimumab
- These findings likely reflect the distinct mechanisms of action between immune checkpoint inhibitors and VEGFR-targeted therapies.
Presented by: Wenxin Xu, MD, Medical Oncologist, Dana-Farber Cancer Institute, Boston, MA, United States of America
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.
Related content: KIM-1 Biomarker Evaluated for Association with Outcomes in Advanced RCC Treatment - Wenxin Xu
References:
- Motzer RJ, Tannir NM, McDermott DF, Arén Frontera O, Melichar B, Choueiri TK, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018;378(14):1277–1290.
- Choueiri TK, Powles T, Burotto M, Escudier B, Bourlon MT, Zurawski B, et al. Nivolumab plus ipilimumab with or without cabozantinib in previously untreated advanced renal cell carcinoma (COSMIC-313): a multicentre, double-blind, randomised, phase 3 trial. Lancet Oncol. 2023;24(12):1274–1288.