(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress, held in Berlin, Germany, between October 17th and 21st, 2025, was host to a renal and urothelial carcinoma proffered paper session. Dr. James Larkin presented the initial results from RAMPART, an international phase III randomized trial of adjuvant durvalumab monotherapy or in combination with tremelimumab for resected primary renal cell carcinoma (RCC).
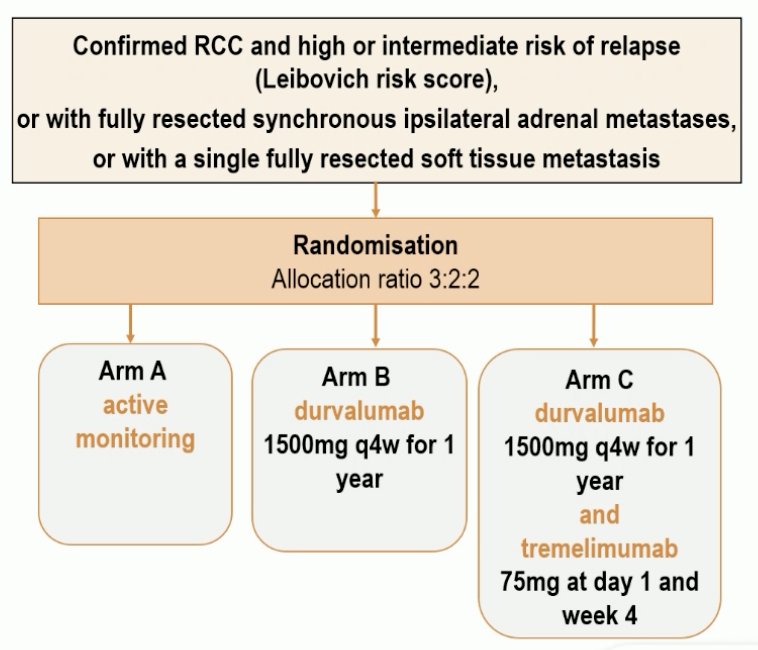
RAMPART employed a multi-arm, multi-stage platform design. Eligible patients were those with confirmed RCC at high or intermediate risk of relapse (Leibovich Score) or with fully resected synchronous ipsilateral adrenal metastases or with a single fully resected soft tissue metastasis. Eligible patients were randomized in a 3:2:2 ratio to:
- Arm A: Active monitoring
- Arm B: Durvalumab 1,500 mg every 4 weeks for 1 year
- Arm C: Durvalumab 1,500 mg every 4 weeks for 1 year + tremelimumab 75 mg at day 1 and week 4

The original planned sample size was 1,750, but this trial was impacted by COVID-19 and the results of the KEYNOTE-564 trial. As such, the new target sample size was adjusted to 750 patients. The primary study outcome was disease-free survival (DFS) with the primary statistical comparison planned between Arms A (active monitoring) and Arm C (durvalumab + tremelimumab).
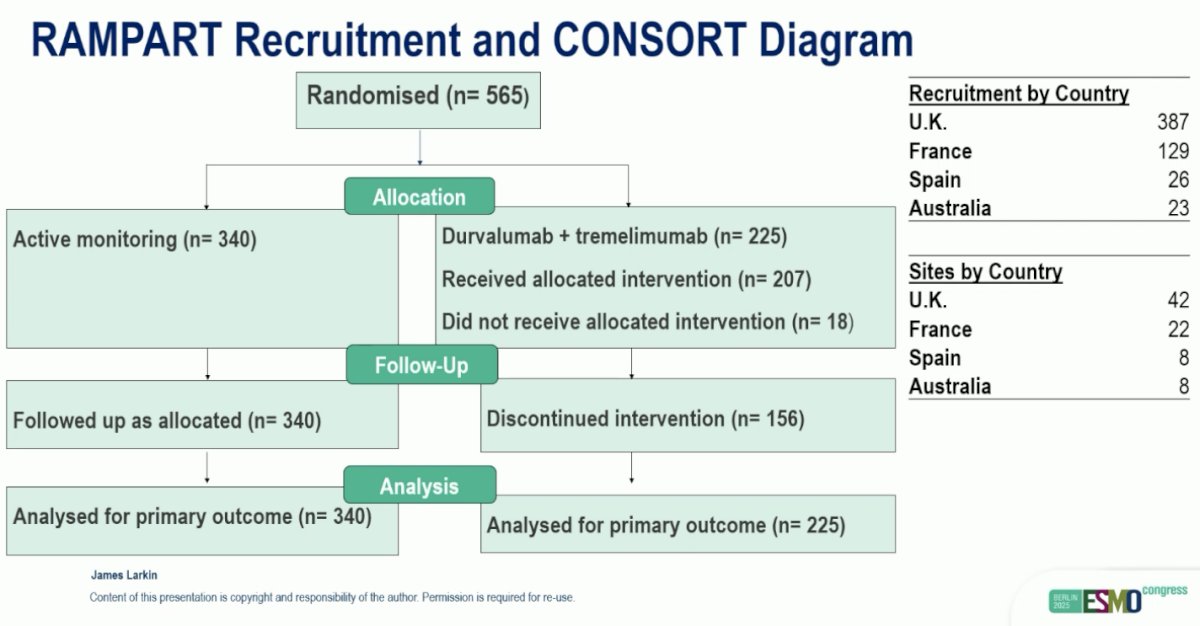
The CONSORT diagram is illustrated below. A total of 340 and 225 patients were randomized to Arms A and C, respectively.
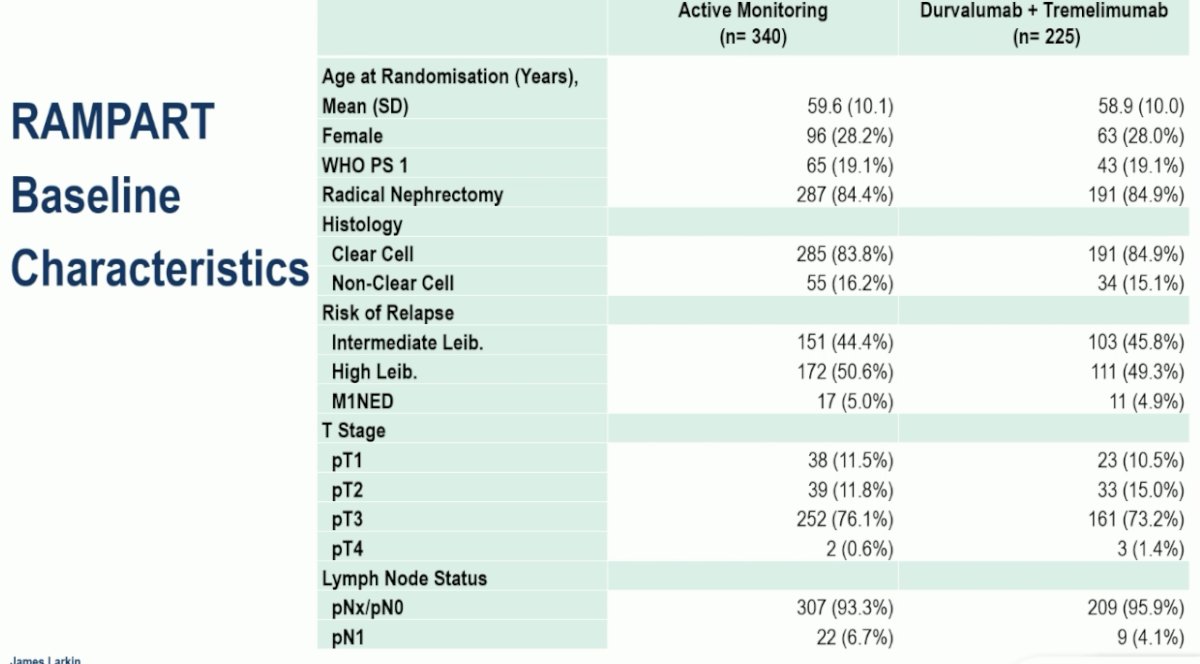
The study arms were well-balanced for baseline characteristics. 16% of patients had non-ccRCC. 45% and 50% of patients were at intermediate and high risks of recurrence, respectively. 5% of enrolled patients were M1 NED.
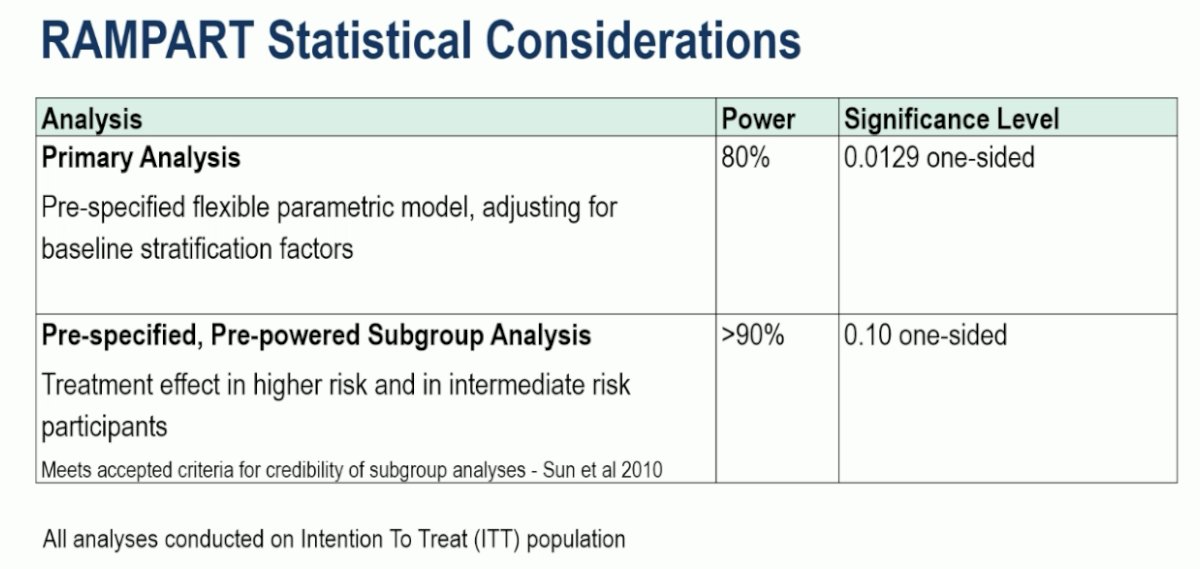
The RAMPART statistical considerations were as follows:
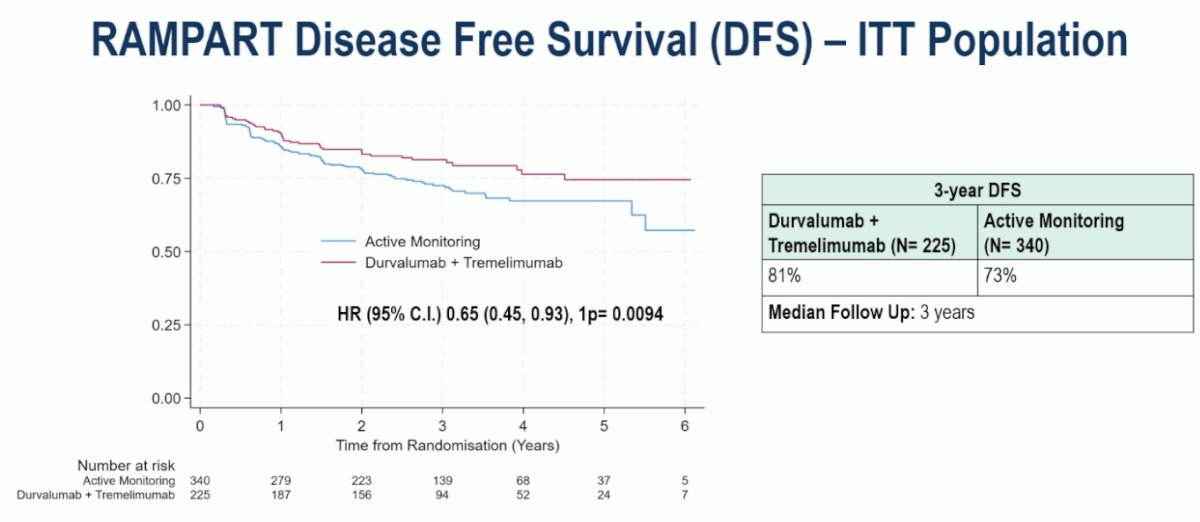
In the intent-to-treat (ITT) population, at a median follow-up of three years, the combination of durvalumab + tremelimumab significantly prolonged DFS, compared to active monitoring (3-year DFS: 81% vs 73%; HR: 0.65, 95% CI: 0.45–0.93, p<0.01):
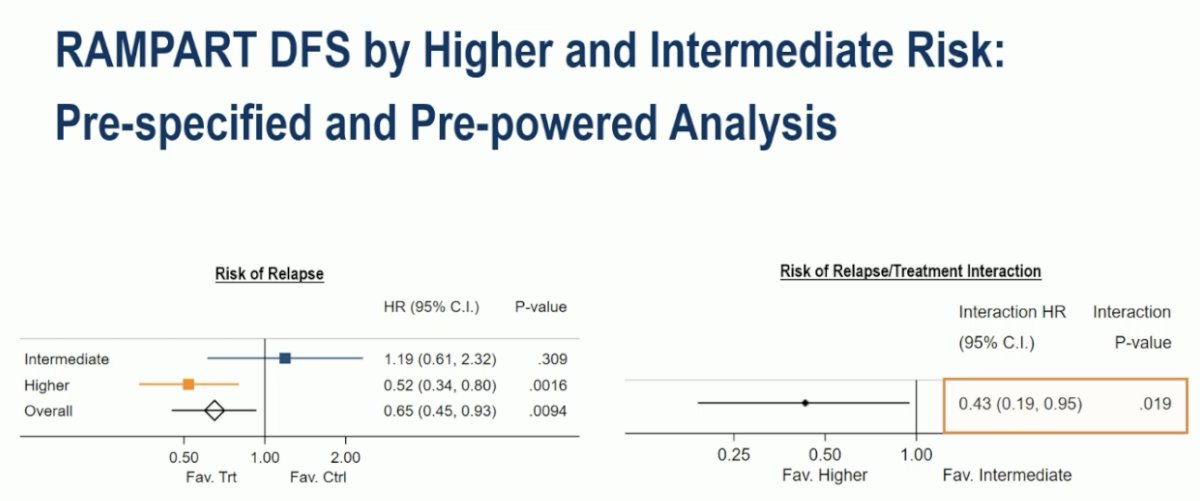
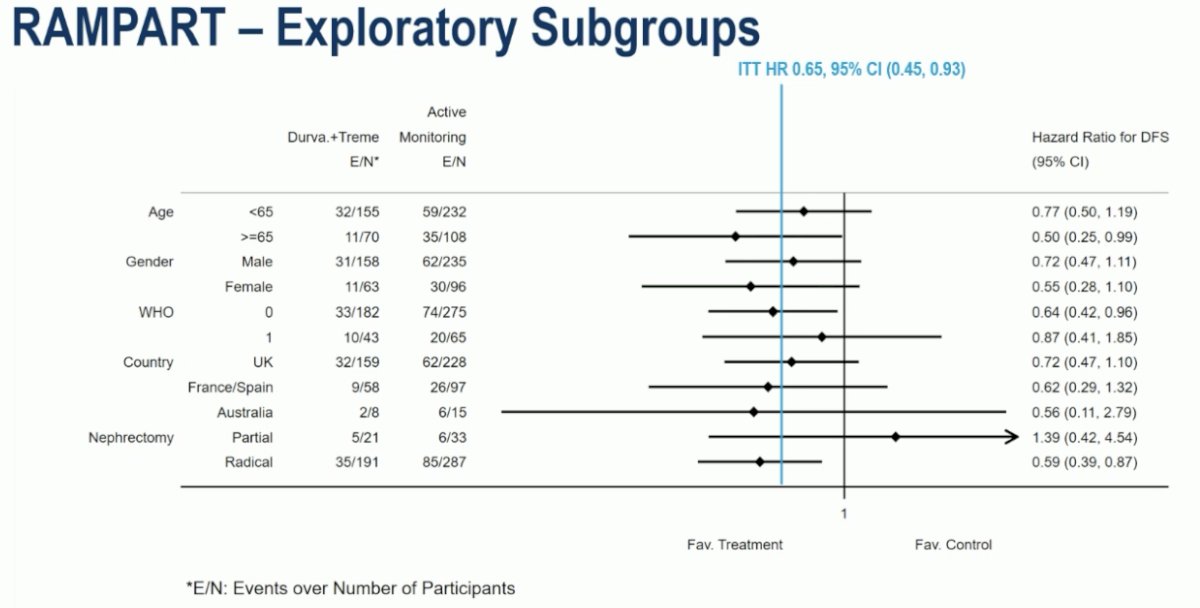
The pre-specified subgroup analyses demonstrated that the DFS benefit was limited to patients at higher risk of relapse (HRs 0.52 vs 1.19; p-value for interaction=0.019):
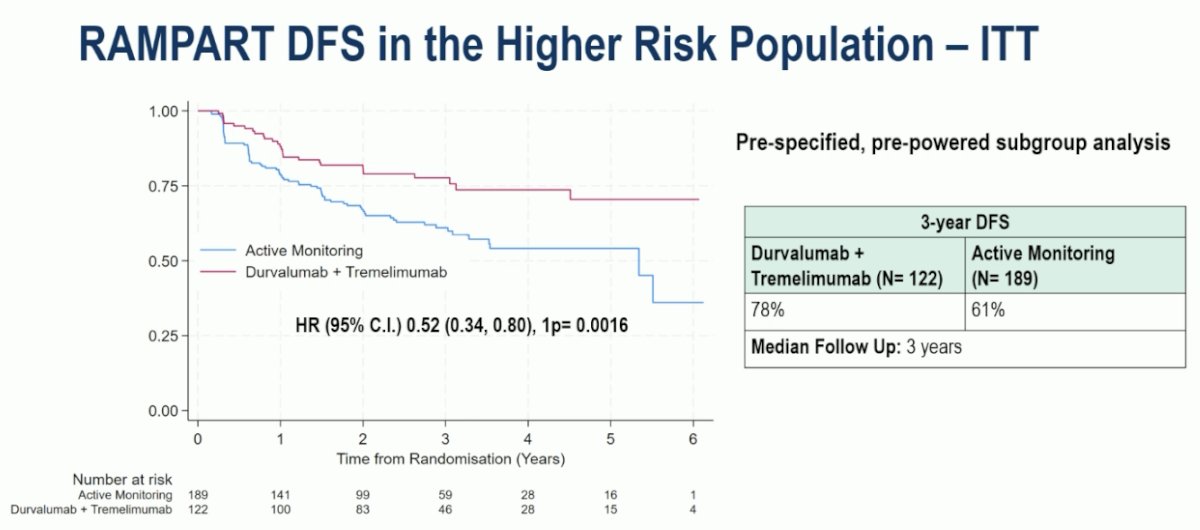
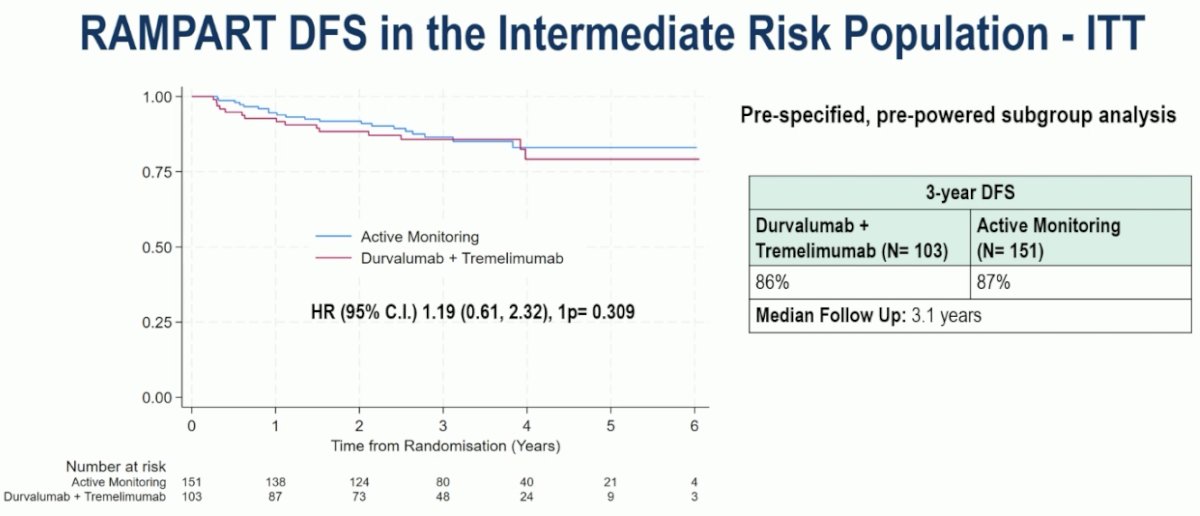
This is further visualized in the Kaplan Meier curves below – 1st one demonstrates DFS for durvalumab + tremelimumab versus active monitoring in the high-risk group, and the 2nd demonstrates the DFS comparison in the intermediate-risk group:
Subgroup analyses demonstrated a consistent DFS benefit in favor of adjuvant therapy.
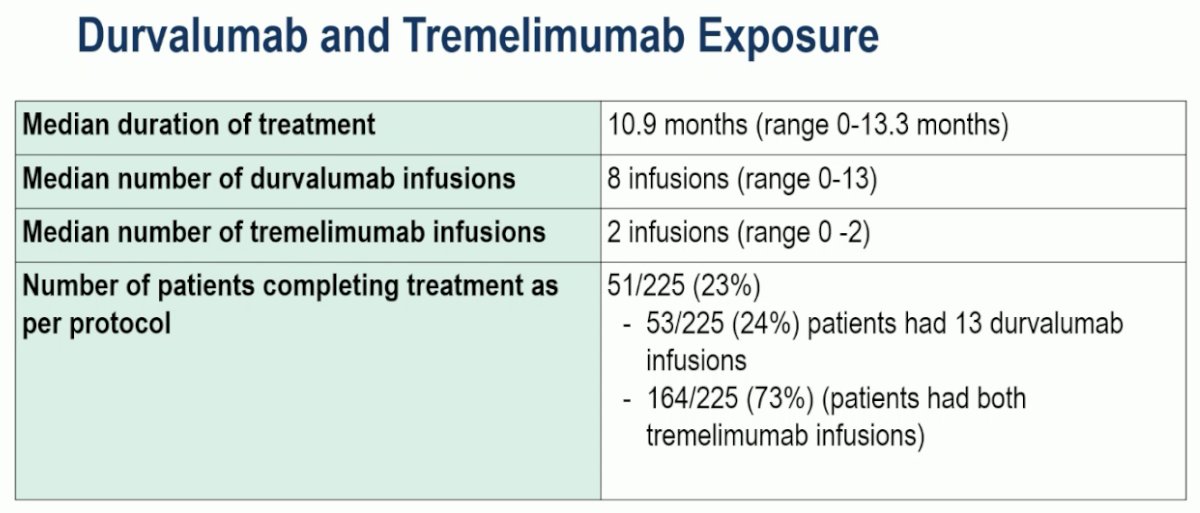
With regards to durvalumab and tremelimumab exposure, only 23% of patients completed all 13 durvalumab infusions.
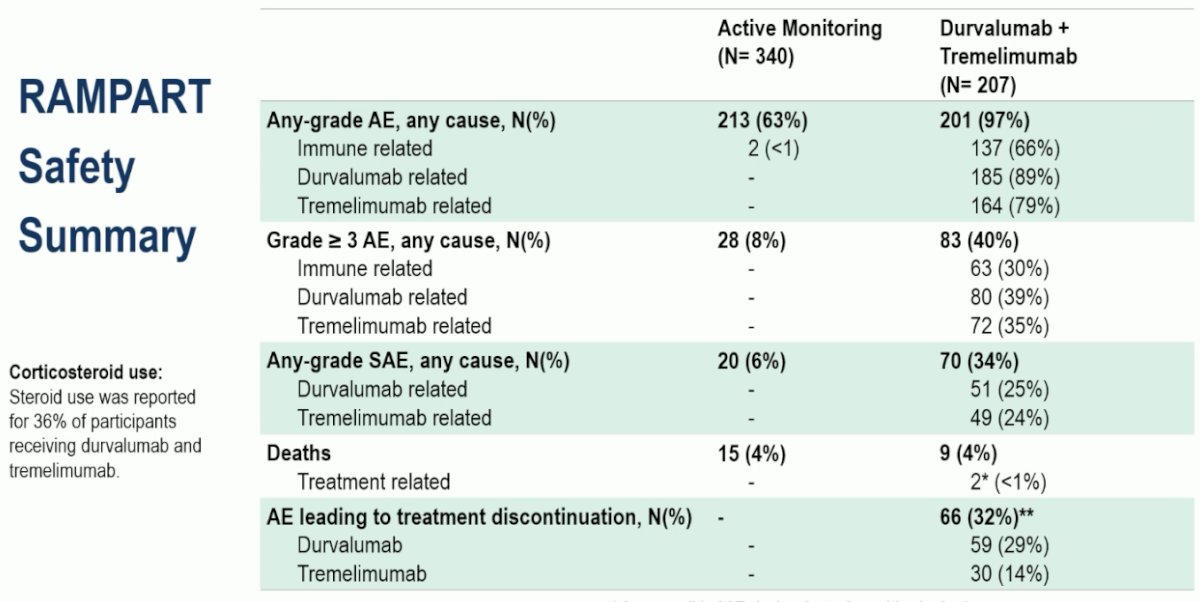
Grade ≥3 adverse events (AEs) were observed in 40% of patients in the durvalumab + tremelimumab arm, compared to 8% in the active monitoring arm. AEs leading to treatment discontinuation were observed in 32% of patients in the durvalumab + tremelimumab arm. There were 15 deaths in the active monitoring arm, compared to 9 in the adjuvant arm.
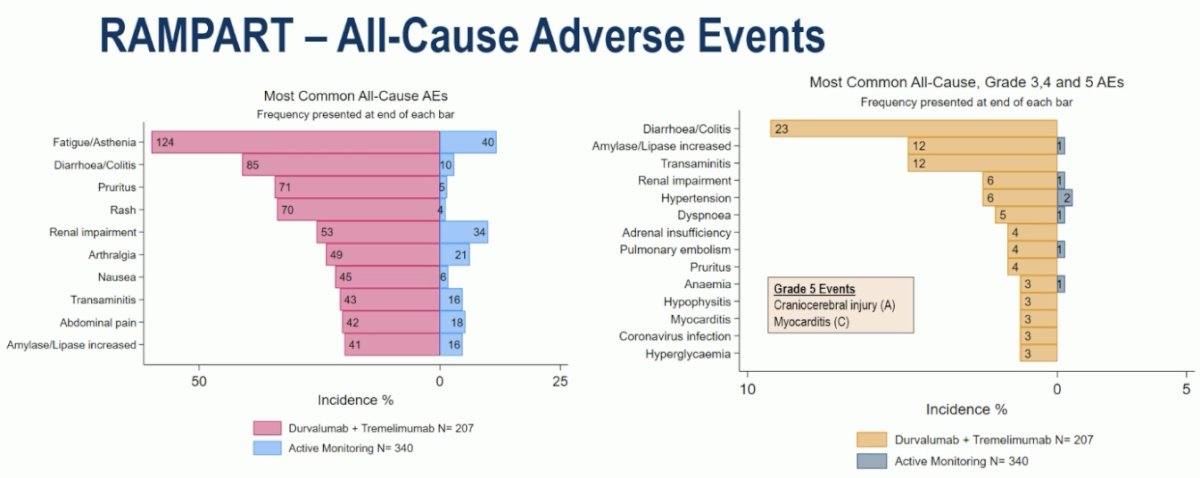
The most common grade ≥3 adverse events in the adjuvant durvalumab + tremelimumab arm were diarrhea/colitis (23%), increased amylase/lipase (12%), and transaminitis (12%).
From a quality-of-life standpoint, the primary outcome assessment was the change in overall health and quality of life from baseline to 15 months, with no statistically significant or clinically meaningful difference observed between the two arms at Month 15.


Dr. Larkin concluded as follows:
- Adjuvant therapy with durvalumab and tremelimumab following RCC resection improved disease-free survival
- There is good evidence that the effect is largely driven by the effect in the higher-risk population
- Safety findings were consistent with the known profiles of durvalumab and tremelimumab
- There was no difference in overall health and quality of life (OHQL) at month 15
- The results of adjuvant durvalumab monotherapy versus active monitoring comparison are expected in 2026
Presented by: James Larkin, PhD, FRCP, F Med Sci, The Royal Marsden NHS Foundation Trust, London, UK
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025