(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between October 17th and 21st, 2025 was host to a renal and urothelial carcinoma proffered paper session. Dr. Cristina Suarez Rodriguez presented the late-breaking abstract from KEYMAKER-U03 Substudy 03A, which evaluated 1st line pembrolizumab-based regimens for advanced clear cell renal cell carcinoma (ccRCC).
First-line triplet regimens adding novel mechanisms of action to standard doublet therapy may be a promising approach for advanced ccRCC. Potential candidates for these regimens include therapies targeting:
- CTLA-4 (e.g., quavonlimab [qmab])
- LAG-3 (e.g., favezelimab [Fave])
- TIGIT (e.g., vibostolimab [Vibo])
The potent and selective HIF-2a inhibitor belzutifan is a treatment option for advanced
RCC following prior anti-PD-(L)1 and VEGFR-TKI therapy and may be a highly suitable candidate for novel triplet therapy in the first-line setting.1
Substudy 03А (NCT04626479) of the umbrella phase 1/2 KEYMAKER-U03 trial was designed to evaluate novel pembrolizumab-based regimens in the first line setting for participants with advanced ccRCC. The study employed an adaptive design in which experimental arms were added and/or inactivated on a rolling basis with a continuous enrolling reference arm. The experimental arms each had a safety lead-in phase of 10 patients (40 total).
The study design of KEYMAKER-U03 Substudy 03A (NCT04626479) is illustrated below.
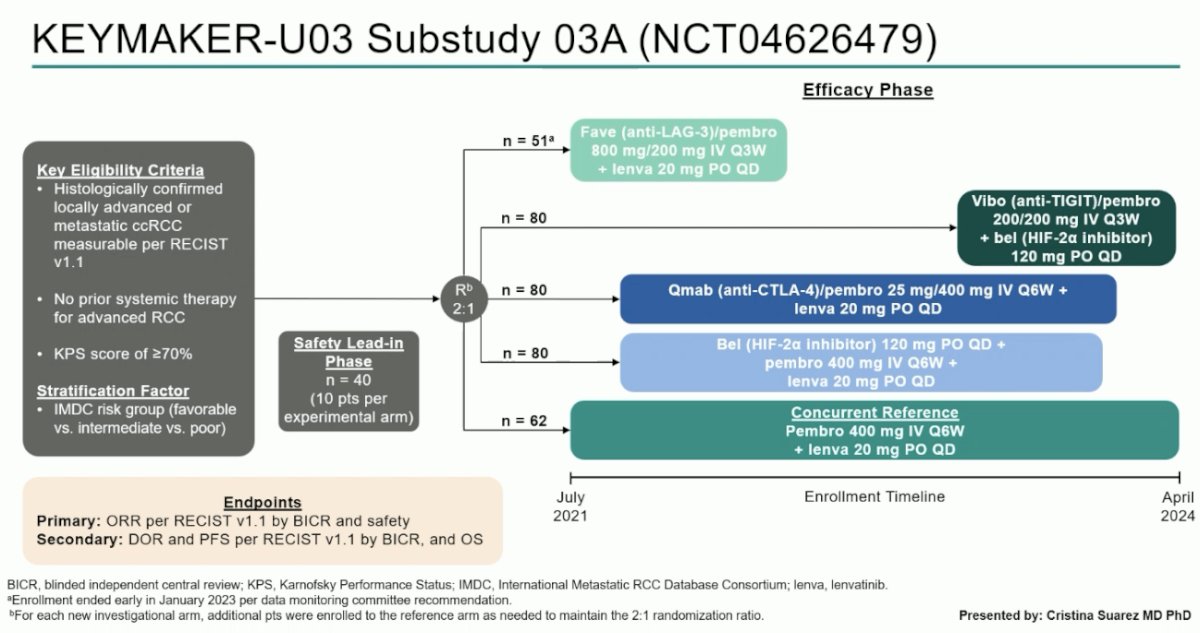
Eligible participants were those with histologically confirmed locally advanced or metastatic ccRCC with no prior systemic therapy for advanced RCC and excellent performance status. The 1st phase of the trial was a safety lead-in with 10 patients per experimental arm.
Following the lead-in phase, patients were randomized 2:1 as follows:
- Reference arm: Pembrolizumab (400 mg IV Q6W) + lenvatinib (20 mg PO daily)
- Experimental arms (open for enrollment at varying timepoints)
- Fave (anti-LAG-3)/Pembrolizumab (800 mg/200 mg IV Q3W) + lenvatinib (20 mg PO daily)
- Vibo (anti-TIGIT)/pembrolizumab (200/200 mg IV Q3W) + belzutifan (HIF-2α inhibitor; 120 mg PO daily)
- Qmab (anti-CTLA-4)/pembrolizumab (25/400 mg IV Q6W) + lenvatinib (20 mg PO daily)
- Belzutifan (120 mg PO daily) + pembrolizumab (400 mg IV Q6W) + lenvatinib (20 mg PO daily)
The study endpoints were as follows:
- Primary:
- Objective response rate (ORR) per RECIST v1.1 by blinded independent central review (BICR)
- Safety
- Secondary:
- Duration of response (DOR)
- Progression-free survival (PFS) per RECIST v1.1 by BICR
- Overall survival (OS)
The statistical methods were as follows:
- Primary efficacy endpoint: ORR estimate of each arm
- ORR and 95% Cls were calculated using Clopper-Pearson methodology
- Secondary efficacy endpoints: PFS, OS, DOR estimates for each arm
- Medians and landmark rates for DOR, PFS, OS, and associated 95% Cls were estimated via Kaplan-Meier methodology
- All efficacy comparisons between arms were exploratory, and the study was not powered for formal hypothesis testing
- Efficacy was assessed in all randomized patients
- HRs were ad hoc and estimated against concurrently randomized patients in the reference arm (pembro plus lenva)
- Safety was assessed in all patients who received ≥1 dose
The baseline patient characteristics are summarized by treatment arm. Overall, 68% of patients had IMDC intermediate-risk disease, and 58-70% had a prior nephrectomy.

The ORR was highest in the reference arm of pembrolizumab + lenvatinib – 81%. The ORRs in the other four arms were as follows:
- Fave (anti-LAG-3) + pembrolizumab + lenvatinib: 63%
- Vibo (anti-TIGIT) + pembrolizumab + belzutifan: 43%
- Qmab (anti-CTLA-4) + pembrolizumab + lenvatinib: 71%
- Belzutifan (HIF-2α inhibitor) + pembrolizumab + lenvatinib: 78%
- Highest complete response (CR) overall: 13%

A comparison of efficacy survival outcomes (DOR, PFS, & OS) between the experimental arms including Fave, Vibo, and Qmab and the reference demonstrated no significant differences.



However, in the comparison of the reference arm with the experimental arm of belzutifan + pembrolizumab + lenvatinib, patients in the experimental arm were found to have superior:
- DOR:
- Median: 33.4 vs 25.6 months
- 12 months: 92% vs 55%
- PFS:
- Median: 32 vs 21 months (HR: 0.45, 95% CI: 0.25–0.83)
- 24 months: 67% vs 45%
- OS:
- Median: Not reached in either arm
- 24 months: 86% vs 67%
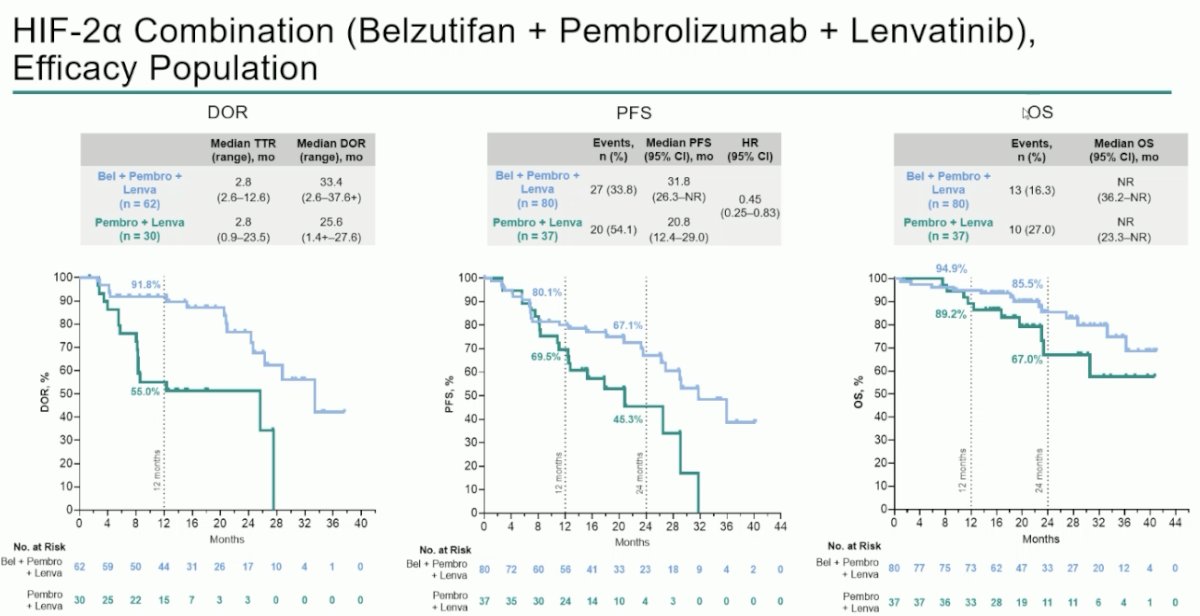
The key efficacy data are summarized in the table below:
 \
\
The arm with the highest incidence of grade ≥3 treatment-related adverse events (TRAEs) was the fave (anti-LAG-3) intensification arm (87% versus 69–73%). TRAEs leading to study treatment discontinuation and serious TRAEs were similarly highest in the fave intensification arm (38% and 36%, respectively). The corresponding incidences of TRAEs leading to treatment discontinuation and serious TRAEs in the belzutifan intensification arm were 24% and 22%, respectively, and lower than those observed in the reference arm (30.6% for both).

The most common grade ≥3 TRAE observed in the lenvatinib arms was hypertension, whereas anemia was the most common grade ≥3 TRAE in the belzutifan arms. No new safety signals were observed.

Dr. Suarez Rodriguez concluded as follows:
- The observed efficacy and safety of pembrolizumab + lenvatinib were confirmatory of prior observations for this combination
- Belzutifan + pembrolizumab + lenvatinib and quavonlimab/pembrolizumab + lenvatinib had similar ORR compared with pembrolizumab + lenvatinib as first-line therapy in patients with previously untreated advanced ccRCC
- Responses were potentially less favorable with favezelimab/pembrolizumab + lenvatinib and vibostolimab/pembrolizumab + belzutifan compared with pembrolizumab + lenvatinib
- Belzutifan + pembrolizumab + lenvatinib, but not the other investigative arms, may have been associated with a higher proportion of CRs, prolonged DOR, and prolonged PFS compared with pembrolizumab + lenvatinib
- The duration of follow-up was insufficient to detect long-term contributions to OS
- Safety findings for all investigative regimens were generally consistent with the safety profiles of the individual drugs
- Belzutifan + pembrolizumab + lenvatinib and quavonlimab/pembrolizumab + lenvatinib are currently being explored in the fully enrolled, randomized phase 3 LITESPARK-012 study
Presented by: Cristina Suarez Rodriguez, MD, PhD, Attending Physician, Vall d'Hebron University Hospital, Barcelona, Spain
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Reference:
- Choueiri TK, Powles T, Peltola K, et al. Belzutifan versus everolimus for advanced renal-cell carcinoma. N Engl J Med. 2024; 391(8):710–721.
KEYMAKER-U03 Substudy Compares Four Combinations to Standard Therapy - Cristina Suárez
Novel Pembrolizumab-Based Treatments as First-Line Therapy in Advanced Clear Cell Renal Cell Carcinoma: Substudy 03A of the Open-Label, Umbrella Platform, Phase I/II KEYMAKER-U03 Trial.