(UroToday.com) The 2025 ESMO annual meeting featured a kidney cancer mini oral session and a discussant presentation by Dr. Laurence Albiges discussing three abstracts “Fruquintinib + sintilimab versus axitinib or everolimus monotherapy as second line treatment in patients with locally advanced or metastatic renal cell carcinoma (RCC): results from phase 3 part of a randomized, open-label, active-controlled phase 2/3 study (FRUSICA-2)” by Dr. Zhenhua Liu, “Phase 1b/2 Trial of Ipilimumab, Nivolumab, and Ciforadenant (Adenosine A2a Receptor Antagonist) in First-line Advanced RCC, a Kidney Cancer Research Consortium Study” by Dr. Kathryn Beckermann, and “Final efficacy data and biomarker analysis from the clear cell cohort of CALYPSO” by Dr. Sara Coca Membribes.
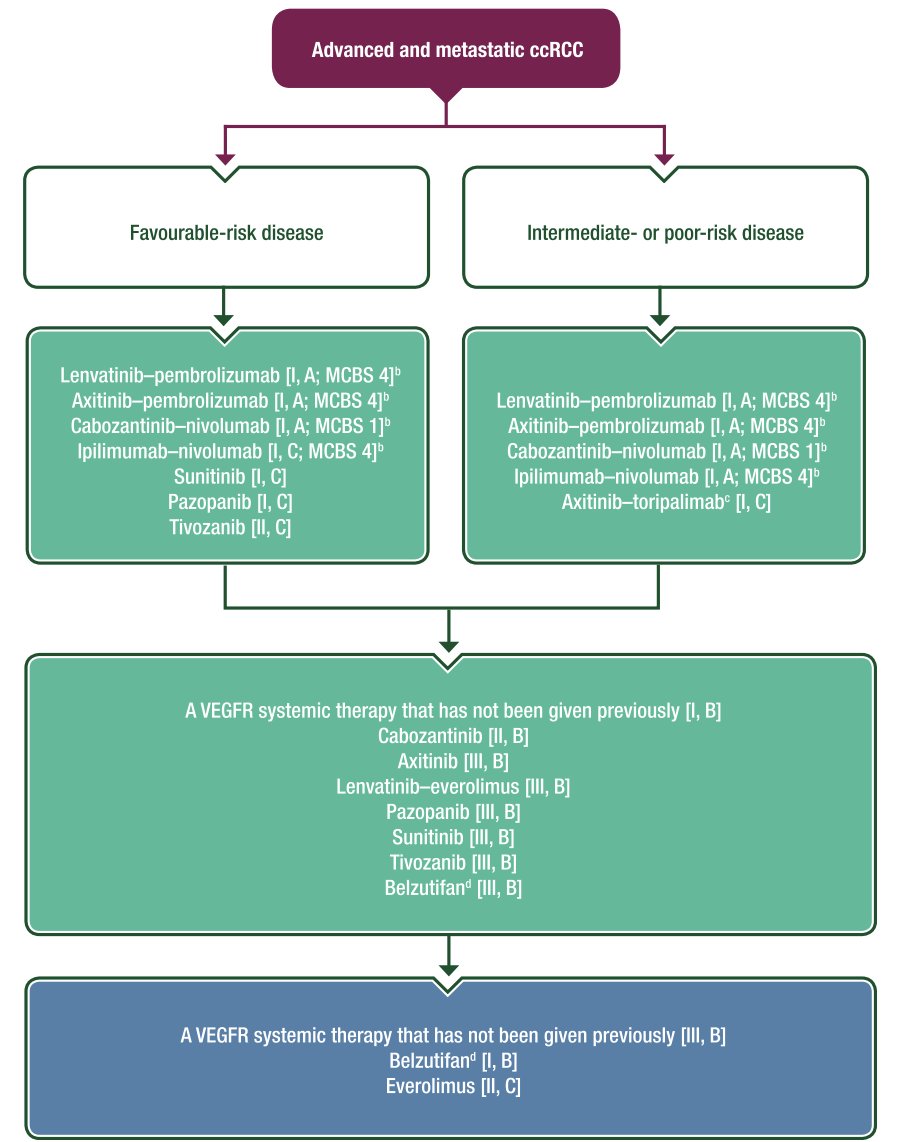
Dr. Albiges started her presentation highlighting the current metastatic RCC landscape according to the ESMO clinical practice guidelines:
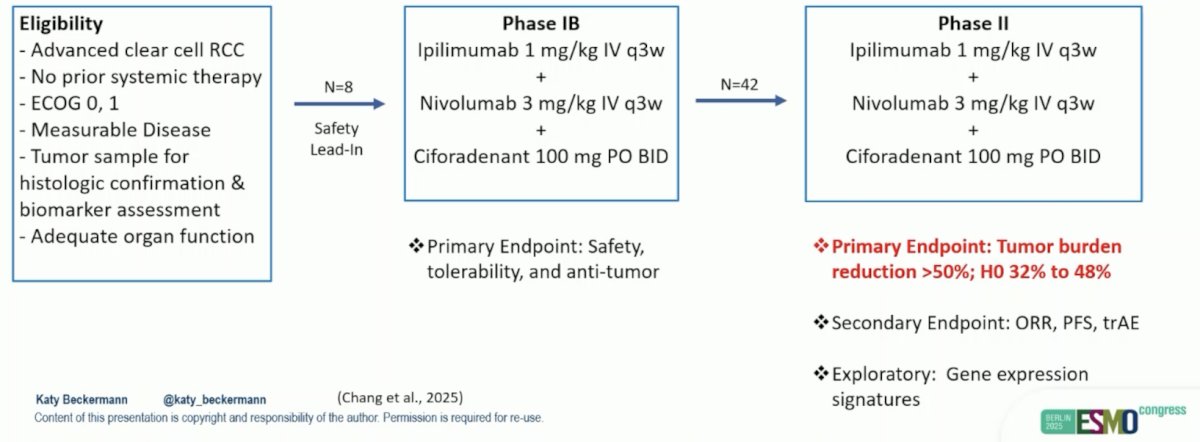
The phase 1b/2 trial of ipilimumab, nivolumab, and ciforadenant in first-line advanced RCC asked the question of whether we can do better than immunotherapy + immunotherapy in first-line treatment. In a phase I study of single-agent ciforadenant (n = 33) and ciforadenant + atezolizumab (n = 35), the response rate for monotherapy was only 3% and was 11% for the combination regimen. In the current trial, eligibility criteria included untreated advanced clear cell RCC, ECOG performance status 0 or 1, and measurable disease by RECIST 1.1. The study included a safety phase 1b lead-in with ciforadenant 100 mg BID orally, nivolumab 3 mg/kg, and ipilimumab 1 mg/kg q3 weeks and a phase 2 dose-expansion. The primary objective was to assess safety and depth of response >50% based on a Bayesian design (H0 32%, H1 48%):
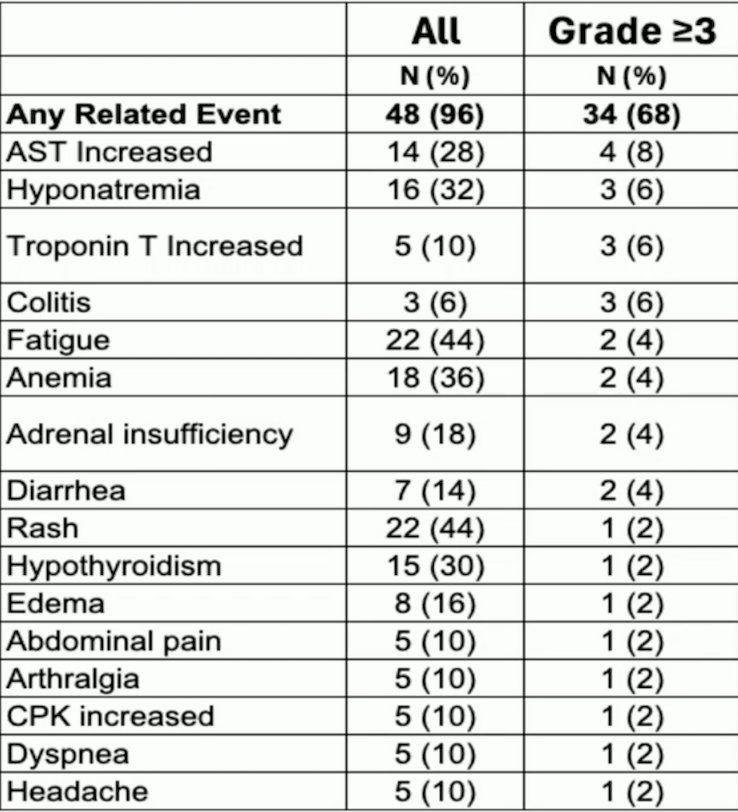
The grade 3 or higher adverse event rate was 68% with the most common all-grade treatment-related adverse events being fatigue, rash, AST and ALT increase, and hyponatremia. One patient died of immune checkpoint inhibitor overlap syndrome. Treatment discontinuation secondary to toxicity occurred in 5 patients (10%):
Dr. Albiges emphasized that the observed safety profile is close to nivolumab + ipilimumab, with no additional toxicity. From an efficacy standpoint, the median follow-up is 9.4 months, during which 17 patients (34%) achieved >50% tumor shrinkage, and the objective response rate was 46% (95% CI 33%, 60%):
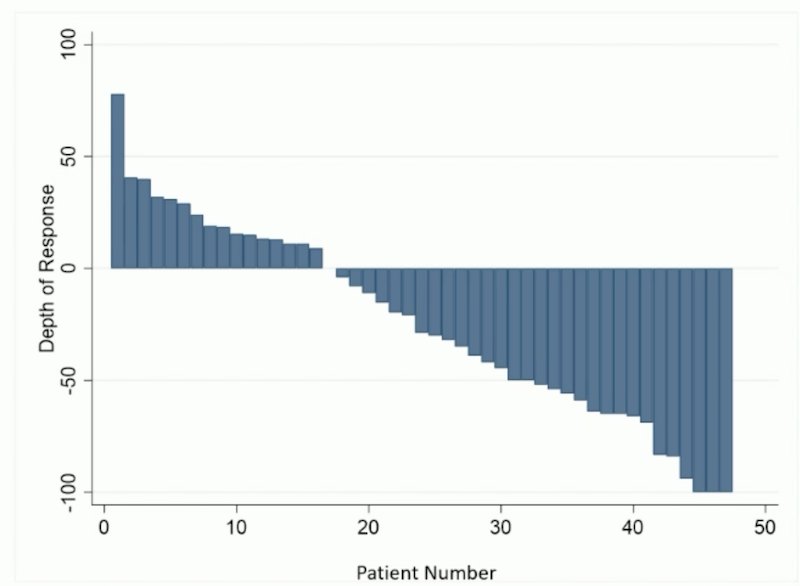
There were 16% of patients who had progressive disease as the best response, and the median progression-free survival was 11.0 months (95% CI 7.1, 13.8). Dr. Albiges notes that there was limited follow-up for objective response rate and progression-free survival, and that the results appear similar to nivolumab + ipilimumab. Ultimately, the current adenosine pathway inhibitor has not demonstrated enough activity in metastatic RCC, but there are currently other efforts to enhance the IO-IO response. These include: an adaptive design (PDIGREE), triplet with VEGFR-TKI (MK6482-012), triple with HIF inhibitor (eVOLVE-RCC02), and microbiome intervention:

Next, Dr. Albiges discussed second-line therapy and whether there is a role for combination therapy post-VEGFR-TKI failure. Looking at data from France, this situation of VEGFR-TKI monotherapy still exists, with ~34%-66% VEGFR-TKI monotherapy use in 2020, improving to 22%-24% in 2021, and improving further to 17% in 2022. Similar data has also been reported in the UK, with the following figure highlighting changes in first-line treatment options over time in all IMDC risk groups and poor and intermediate IMDC risk groups:1
![Next, Dr. Albiges discussed second-line therapy and whether there is a role for combination therapy post-VEGFR-TKI failure. Looking at data from France, this situation of VEGFR-TKI monotherapy still exists, with ~34%-66% VEGFR-TKI monotherapy use in 2020, improving to 22%-24% in 2021, and improving further to 17% in 2022. Similar data has also been reported in the UK, with the following figure highlighting changes in first-line treatment options over time in all IMDC risk groups and poor and intermediate IMDC risk groups [1]:](/images/com-doc-importer/234-esmo-2025/esmo-2025-kidney-cancer-discussant-can-we-combine-more-in-line-1-and-line-2/image-5.jpg)
What should the control group be in the IO-naïve situation? The following highlights the trial designs for FRUSICA-2 and CALYPSO:
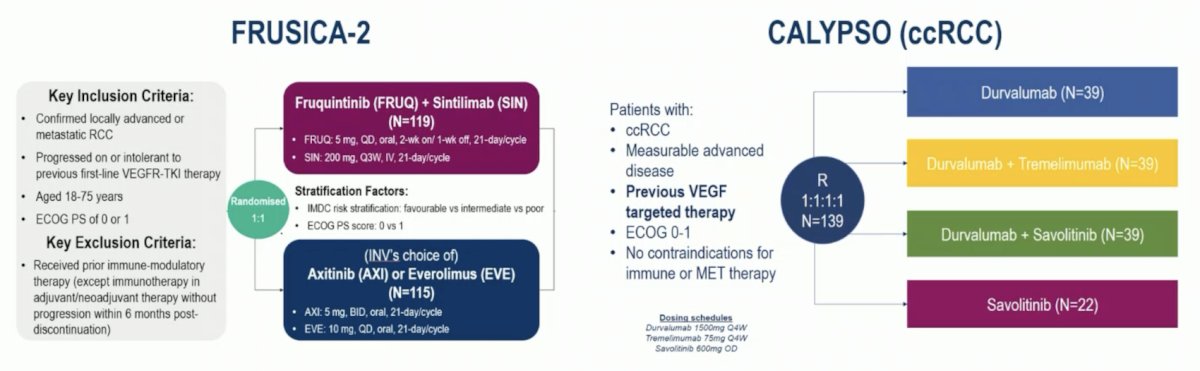
Endpoints in this clinical scenario are also important, which include a primary endpoint of blinded independent central review of progression-free survival in FRUCISCA-2 and confirmed response rate in CALYPSO:

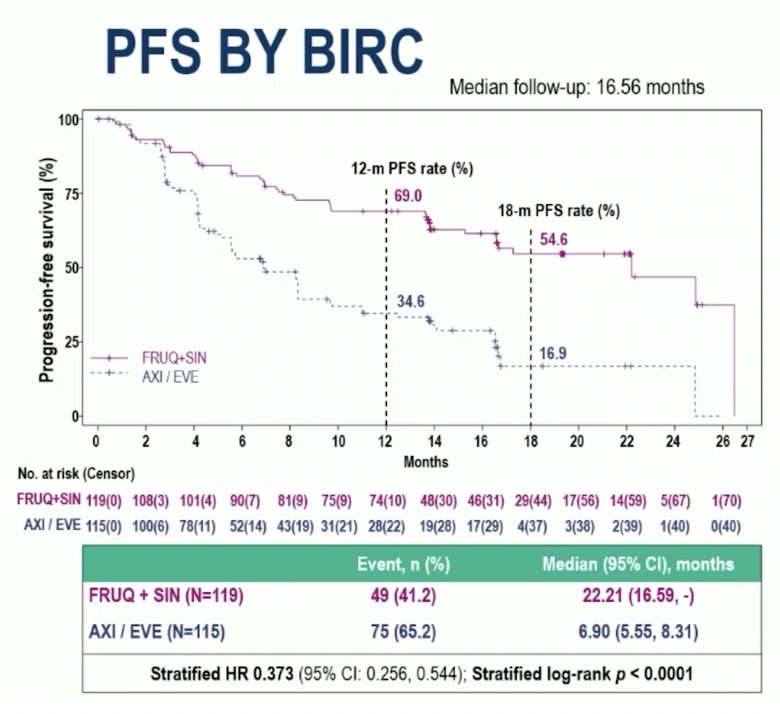
When assessing the patient disposition of FRUSICA-2, Dr. Albiges notes that a 30% screening failure rate seemed quite high to her, and questions remain as to whether patients after progressive disease in the control arm received a PD-1 inhibitor and how this may affect the overall survival analysis. In FRUSICA-2, at the progression-free survival final analysis cutoff, with 16.56 months median of follow up, fruquintinib + sintilimab significantly prolonged the blinded independent review committee-assessed median progression-free survival (22.21 versus 6.90 months, stratified HR 0.373, 95% CI 0.256-0.544, stratified log-rank p < 0.0001) compared to axitinib or everolimus:
Fruquintinib + sintilimab had an objective response rate of 60.5% versus 24.3% (OR 4.622, p < 0.0001) for axitinib or everolimus by blinded independent central review:

For reference, the benchmark objective response rate in this disease space is the METEOR trial (cabozantinib versus everolimus), which reported an objective response rate of 21%.2 Additional benchmarks include KEYNOTE-146 (lenvatinib + pembrolizumab), which reported an objective response rate of 59%,3 and the KEYMAKER-U03 Substudy 03B (lenvatinib + belzutifan), which reported an objective response rate of 46.9% (ASCO GU 2025). For FRUSICA-2, Dr. Albiges notes that progression-free survival and overall survival require further follow-up and that the control arm should include access to PD-1 inhibitors.
With regards to CALYPSO, this study design allows exploration of the contribution of each component, albeit with sample size limitations. Given the IO naïve profile, it is a distinct study population from OMNIVORE, FRACTION RCC, TITAN RCC, or HCRN. CALYPSO was a multinational, open-label, randomized phase II study in patients with advanced RCC previously treated with VEGF-targeted therapy but naïve to immune checkpoint and MET inhibitors. Patients were randomized to durvalumab, savolitinib, durvalumab + tremelimumab, or durvalumab + savolitinib. Over a median follow-up of 40 months, there was no progression-free survival or overall survival benefit for durvalumab + tremelimumab over durvalumab. Additionally, CALYPSO showed no predictive role of PD-L1 for CTLA+PD1.
So, does combination therapy make sense after first-line VEGFR-TKI single-agent failure?
- This situation still exists
- A PD-1 backbone should be the comparator for these trials
- Current data mostly support a sequencing strategy
- A randomized phase III trial is unlikely to be conducted, given that the standard of care in first-line treatment has evolved
Presented by: Laurence Albiges, MD, PhD, Gustave Roussy, Villejuif, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
References:
- Frazier R, McGrane JM, Challapalli A, et al. Real-world patterns of treatment and response in metastatic renal cell carcinoma: a multicentre UK-wide review with UK Renal Oncology Collaborative (UK ROC). ESMO Real World Data Digit Oncol. 2024;3.100027.
- Choueiri TK, Escudier B, Powles T, et al. Cabozantinib versus Everolimus in Advanced Renal-Cell Carcinoma. N Engl J Med 2015;373(19):1814-1823.
- Lee CH, Yogesh Shah A, Rao A, et al. Lenvatinib plus Pembrolizumab following immune checkpoint inhibitor treatment in patients with metastatic clear cell renal cell carcinoma: Results from Study 111/KEYNOTE-146. Eur Urol. 2024 Nov;86(5):470-473.
Novel Pembrolizumab-Based Treatments as First-Line Therapy in Advanced Clear Cell Renal Cell Carcinoma: Substudy 03A of the Open-Label, Umbrella Platform, Phase I/II KEYMAKER-U03 Trial.