(UroToday.com) The 2025 ESMO annual meeting featured a kidney cancer mini oral session and a presentation by Dr. Zhenhua Liu discussing results from the FRUSICA-2 trial assessing fruquintinib + sintilimab versus axitinib or everolimus monotherapy as second line treatment in patients with locally advanced or metastatic renal cell carcinoma (RCC). RCC accounts for approximately 90% of renal malignancies, and patients with metastatic RCC have a dismal prognosis with a 5-year survival rate of approximately 15–20%. Despite immune checkpoint inhibitor + tyrosine kinase inhibitor (TKI) becoming the standard of care as first-line therapy for patients with advanced RCC, TKI monotherapy is still the standard first-line treatment in clinical practice in China. Thus, there is a huge unmet need for these patients after treatment failure with TKI monotherapy.
Fruquintinib is a potent small molecule inhibitor of vascular endothelial growth factor receptor (VEGFR) 1–3, and sintilimab is an anti–PD-1 monoclonal antibody. The combination of fruquintinib with sintilimab showed promising efficacy in RCC patients who had previously received one standard systemic anti-cancer therapy (mainly TKI) in a phase 1b/2 study. FRUSICA-2, a randomized, open-label, active-controlled phase 2/3 study, evaluated the efficacy and safety of fruquintinib + sintilimab versus axitinib or everolimus monotherapy as second line therapy in patients with locally advanced or metastatic RCC. At the ESMO 2025 annual meeting, Dr. Liu and colleagues presented results from the phase 3 portion of the trial.
Eligible patients include those who received one prior VEGFR-TKI therapy and were randomized 1:1 to receive fruquintinib (5 mg, daily, 2 weeks on/1 week off) + sintilimab (200 mg, IV, every 3 weeks), or investigator-selected axitinib (5 mg, BID)/everolimus (10 mg, daily) in 21-day cycles. Randomization was stratified by ECOG performance status and IMDC prognostic risk. The primary endpoint was blinded independent review committee-assessed progression free survival per RECIST 1.1:
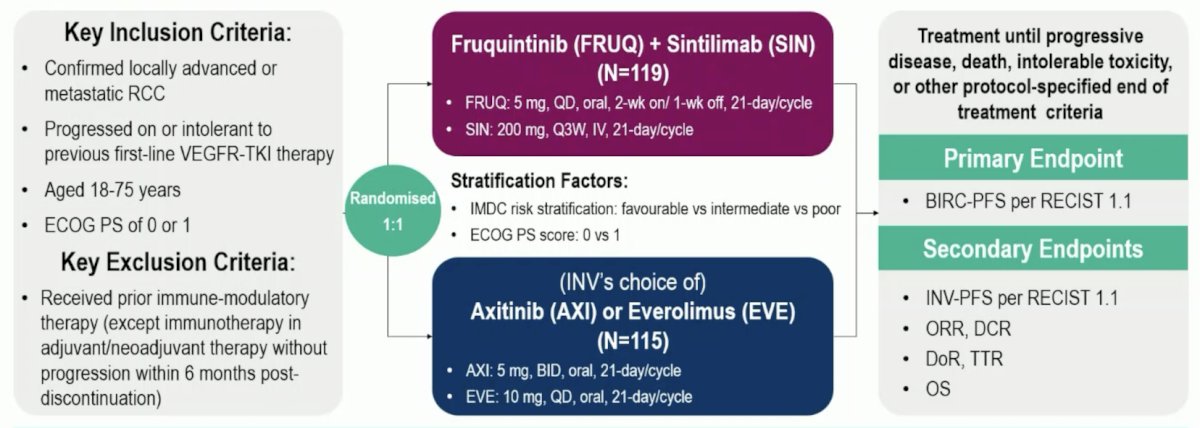
This study had 90% power with 146 blinded independent review progression free survival events in the ITT population, with a one sided alpha = 0.025, assuming a hazard ratio of 0.583. The pre-planned final analysis point was one month after achieving 146 progression free survival events by investigator assessment.
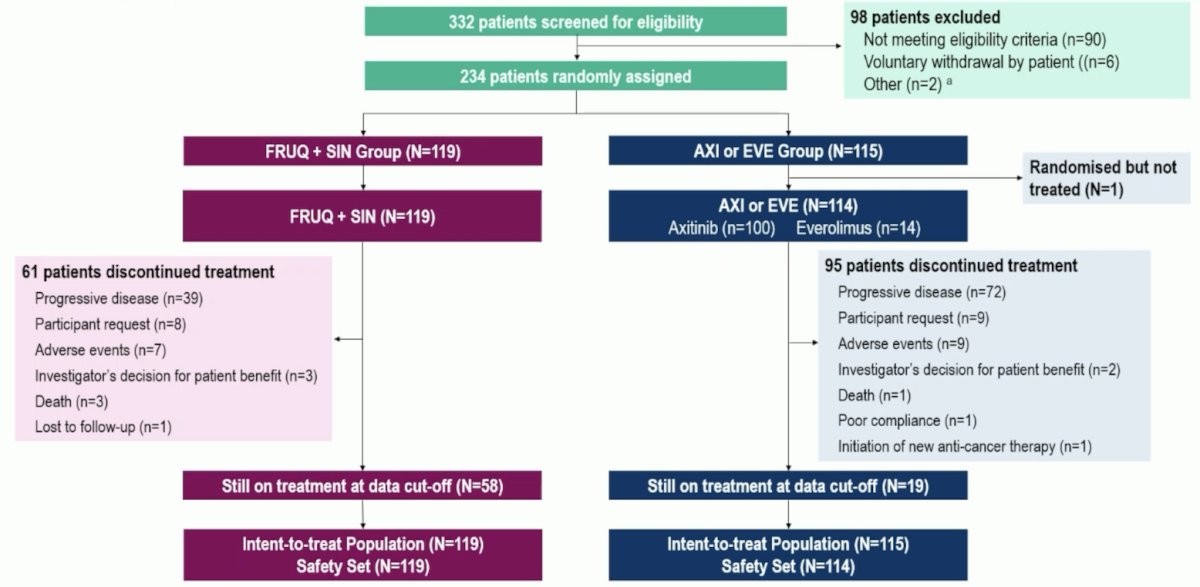
Between October 2022 and December 2023, 234 patients were randomly assigned to the fruquintinib + sintilimab or axitinib or everolimus groups (119 versus 115; 101 on axitinib, but 1 untreated):
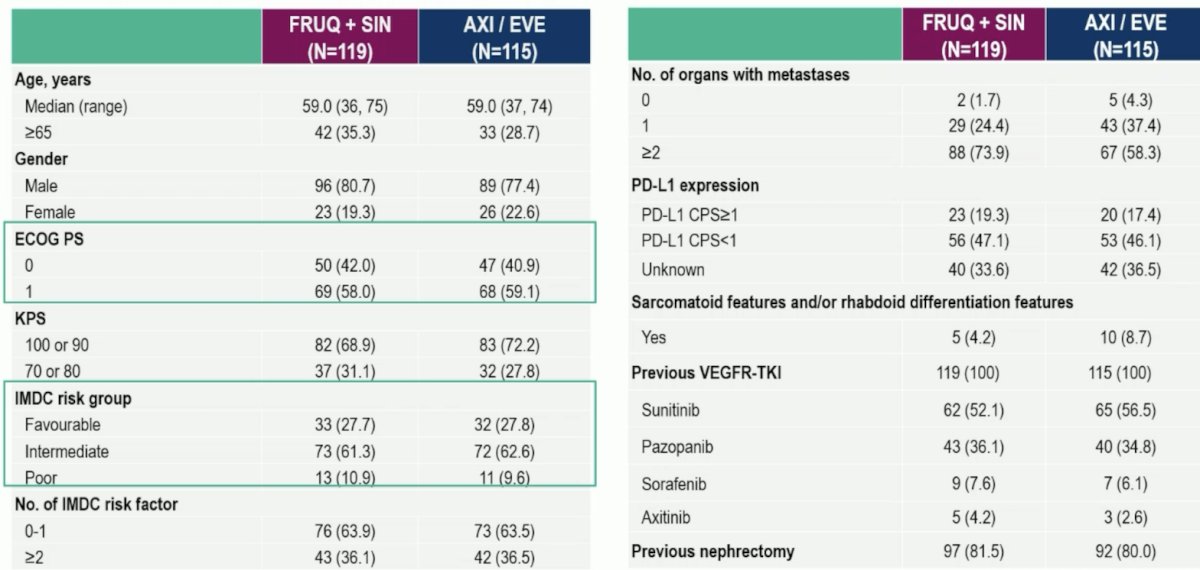
The baseline characteristics were well balanced between groups:
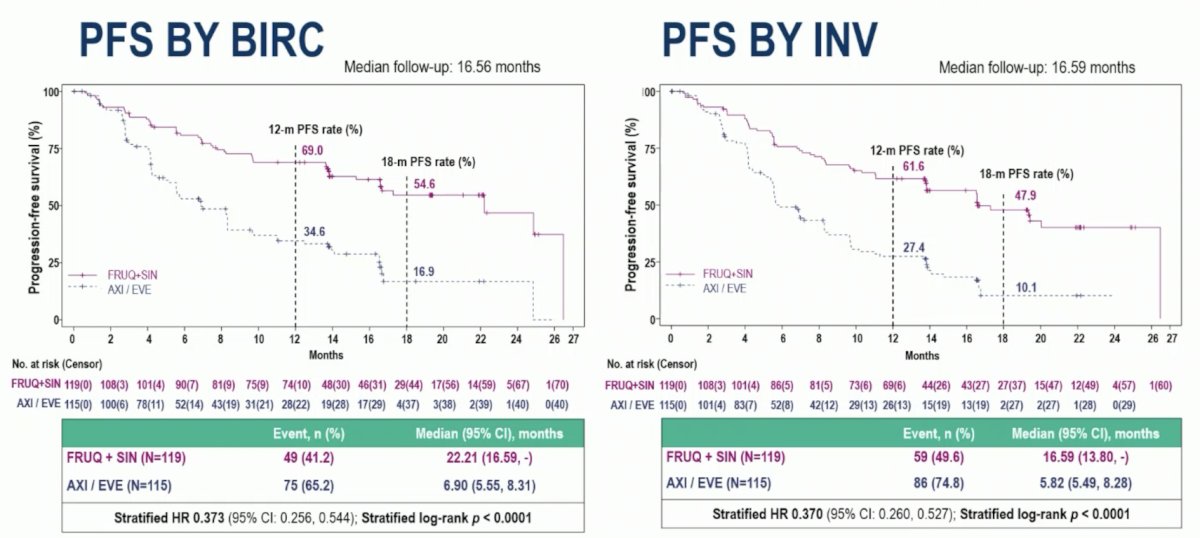
At the progression free survival final analysis cutoff (February 17, 2025), with 16.56 months median of follow up, fruquintinib + sintilimab significantly prolonged the blinded independent review committee-assessed median progression free survival (22.21 versus 6.90 months, stratified HR 0.373, 95% CI 0.256-0.544 stratified log-rank p < 0.0001) compared to axitinib or everolimus, as well as progression free survival by investigator assessment (16.59 versus 5.82 months, stratified HR 0.370, 95% CI 0.260-0.527 stratified log-rank p < 0.0001):
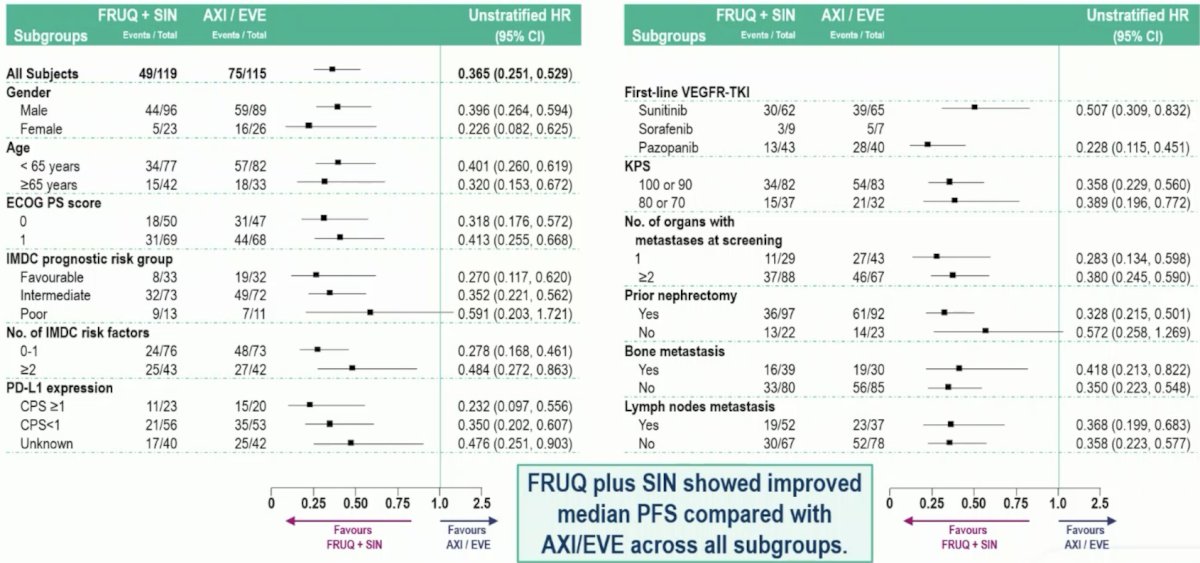
Fruquintinib + sintilimab also improved progression free survival across all subgroups:
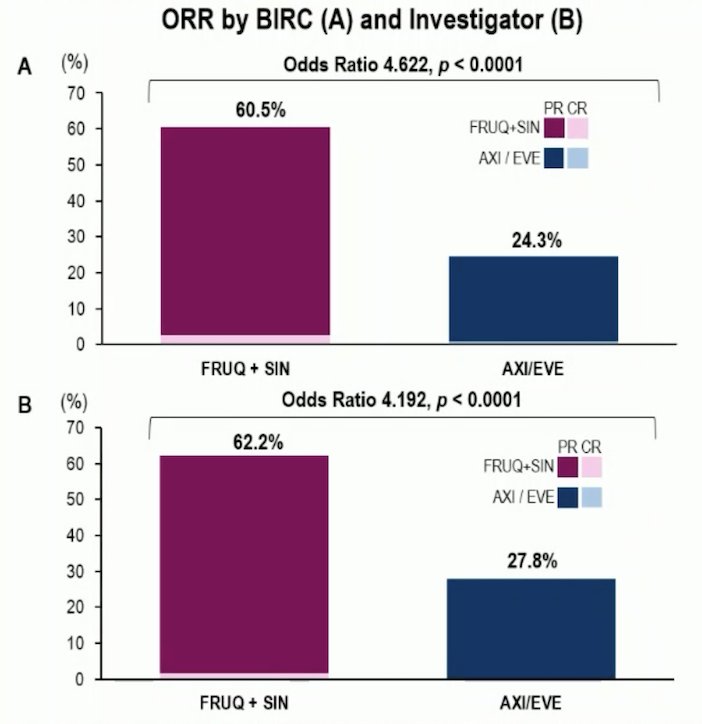
Fruquintinib + sintilimab had an objective response rate of 60.5% versus 24.3% (OR 4.622, p < 0.0001) for axitinib or everolimus by blinded independent central review, as well as 62.2% and 27.8% (OR 4.129, p<0.0001), respectively, by investigator assessment:
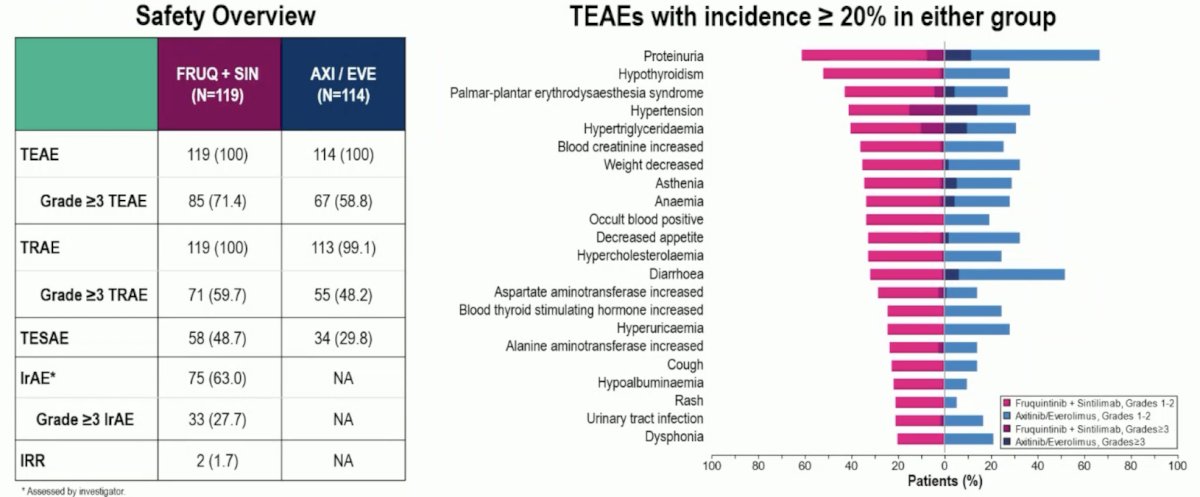
The median duration of response was 23.69 months for fruquintinib + sintilimab versus 11.33 months for axitinib or everolimus. Overall survival data were evolving with data maturity of ∼20% at this data cutoff date, and efficacy benefits were observed in patients regardless of IMDC prognostic risk. The incidences of grade ≥3 treatment emergent adverse events (71.4% versus 58.8%), treatment emergent adverse events leading to treatment discontinuation (17.6% versus 9.6%), and fatal treatment emergent adverse events (4.2% versus 4.4%) were comparable between the groups:
Dr. Liu concluded this presentation discussing results from the FRUSICA-2 trial with the following take home points:
- Fruquintinib + sintilimab demonstrated superior clinical benefits compared to axitinib or everolimus in patients with advanced or metastatic RCC post-VEGFR-TKI:
- The progression free survival improvement was 22.2 months versus 6.9 months by blinded independent central review (HR 0.373, p<0.0001)
- The objective response rate benefit was 60.5% versus 24.3% by blinded independent central review (OR 4.622, p<0.0001)
- The safety profile of fruquintinib + sintilimab was tolerable, and consistent with the known profiles of each individual treatment
- Fruquintinib + sintilimab combination therapy could be a new second line treatment for patients with advanced RCC
Presented by: Zhenhua Liu, Sichuan Clinical Research Center for Kidney and Urologic Diseases, West China Hospital, Sichuan University, Chengdu, China
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between September 17th and 21st.