(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to the Poster Session. Dr. Constantin Rieger presented the poster Cost-Effectiveness Analysis of perioperative Durvalumab plus Platin-based Chemotherapy in muscle invasive bladder cancer.
Dr. Rieger noted that bladder cancer ranks 9th globally, causing ~550,000 new cases and 200,000 deaths annually. About 25% present with MIBC, requiring multimodal therapy. Although NAC with gemcitabine/cisplatin or dd-MVAC improves OS by ~8%, it is used in <20% of eligible patients.1 The NIAGARA trial showed that adding perioperative durvalumab improved 24-month OS (82% vs 75%) and pCR (37% vs 27%).2 Given the high per-patient cost of bladder cancer care, this analysis evaluated the cost-effectiveness of adding durvalumab to standard NAC in the German healthcare system.
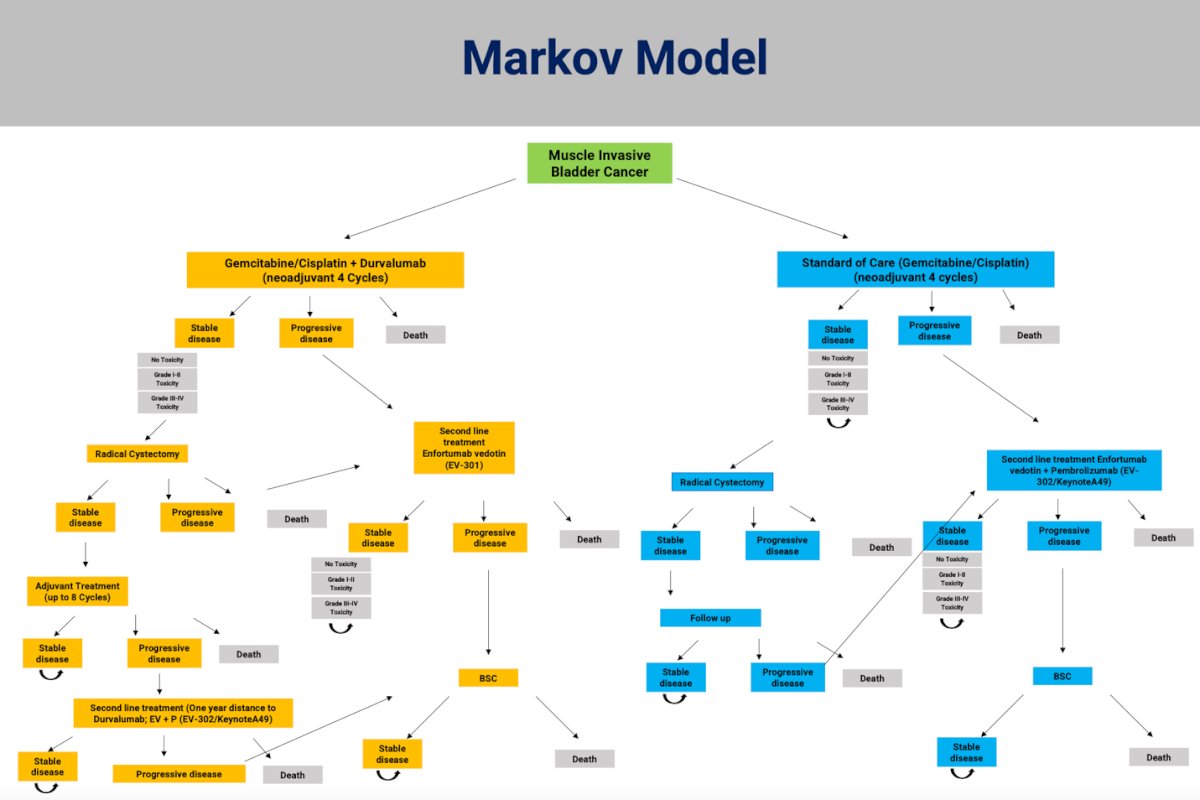
The investigators built a Markov model (Below) to simulate clinical outcomes and economic impact for patients with MIBC treated with neoadjuvant gemcitabine/cisplatin plus durvalumab versus standard gemcitabine/cisplatin alone. The model incorporated transitions between health states including stable disease, progressive disease, and death, accounting for treatment phases such as surgery, adjuvant therapy, and second-line treatment with enfortumab vedotin ± pembrolizumab.
The cost-effectiveness acceptability curve demonstrated that adding durvalumab to gemcitabine/cisplatin was cost-effective in 76.5% of simulations at a willingness-to-pay threshold of €100,000 per QALY, increasing to 94.2% at €150,000.

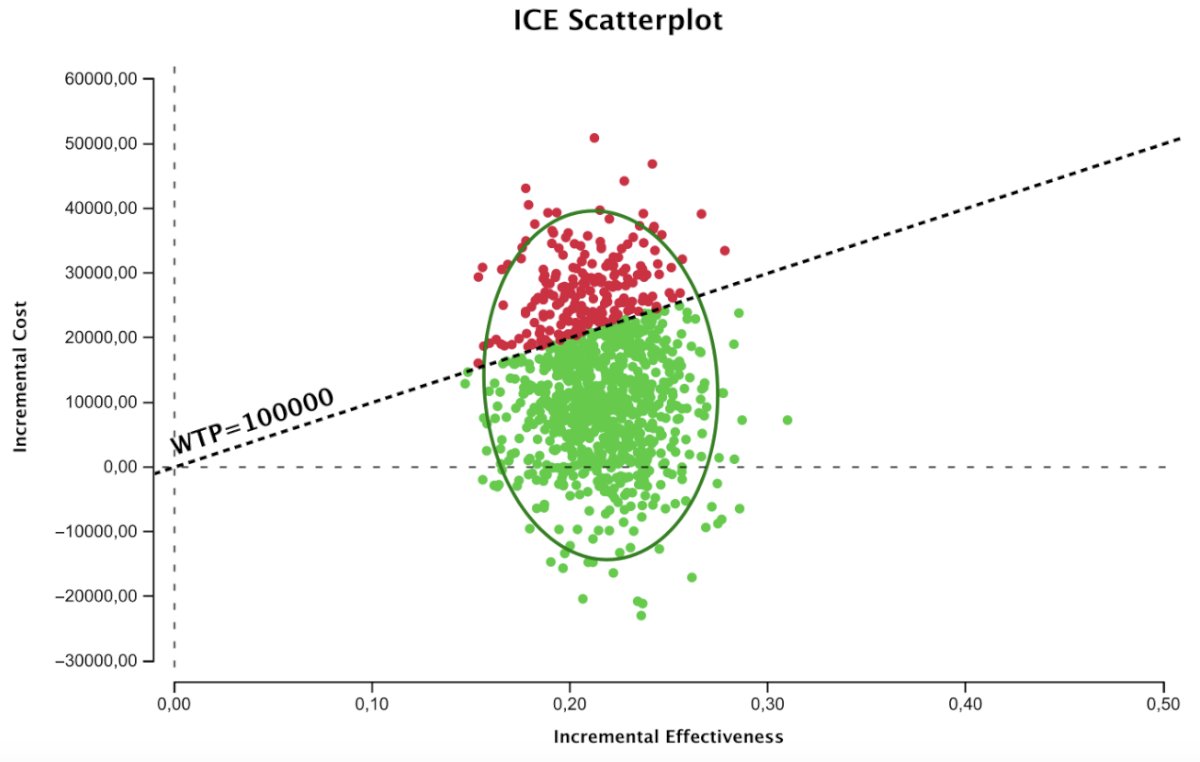
The ICER scatterplot, based on 1,000 simulations, showed that gemcitabine/cisplatin plus durvalumab had an incremental cost of €13,162 and an incremental benefit of 0.21 QALYs, resulting in an ICER of €61,006 per QALY gained. Green points represent scenarios in which the combination was cost-effective within the 95% confidence ellipse.
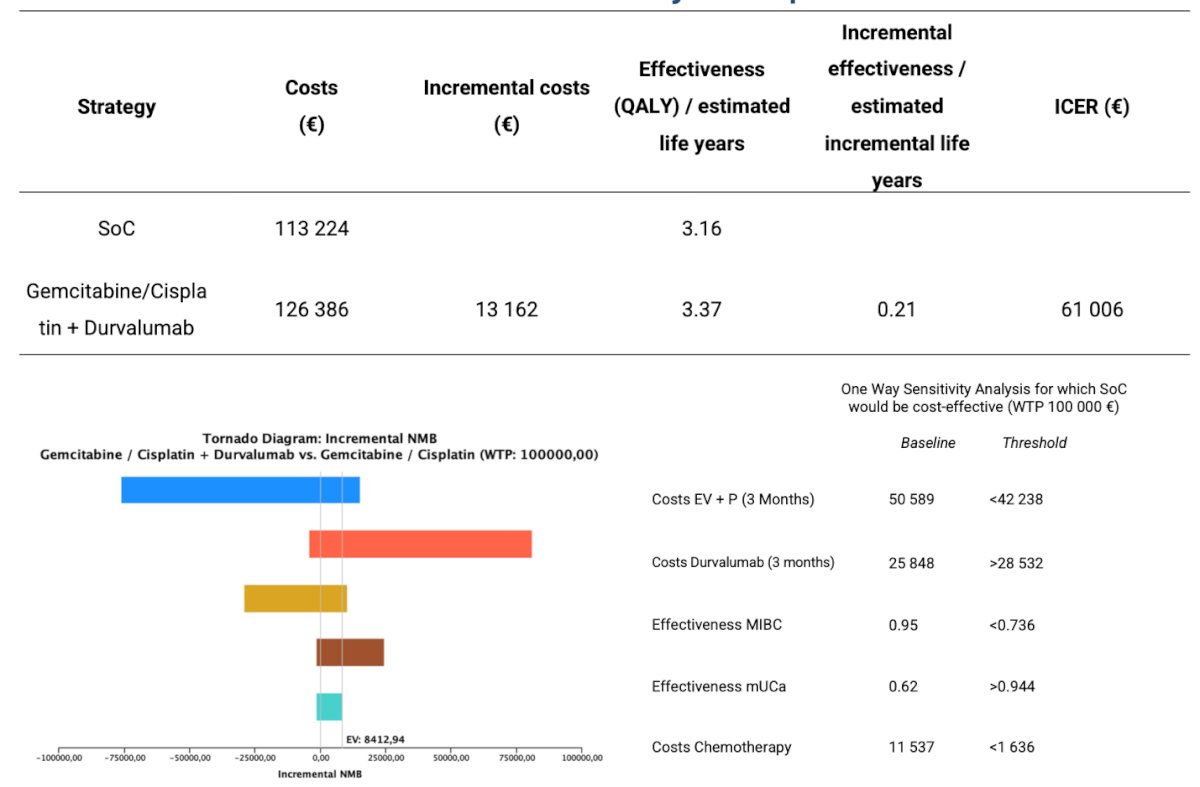
Lastly, the base-case analysis estimated average costs of €113,224 for standard gemcitabine/cisplatin and €126,386 for gemcitabine/cisplatin plus durvalumab. The incremental cost of €13,162, combined with an additional 0.21 QALYs gained, resulted in an ICER of €61,006 per QALY indicating that durvalumab plus Gem/Cis is cost-effective within commonly accepted thresholds.
Dr Rieger concluded their presentation with the following key messages:
- Durvalumab + Gem/Cis was cost-effective in 76.5% of simulations at a willingness-to-pay (WTP) threshold of €100,000/QALY.
- Incremental cost: €13,162; incremental benefit: 0.21 QALYs; ICER: €61,006/QALY.
- The main cost driver was metastatic treatment with enfortumab vedotin + pembrolizumab.
- Even modest survival gains substantially reduced downstream metastatic costs.
- Results highlight the economic and clinical value of preventing progression to metastatic disease.
- Cost-effectiveness applies only to comparison versus Gem/Cis alone, not against MVAC or nivolumab-based regimens.
- Future directions include biomarker-driven (such as ctDNA-guided) adjuvant strategies to refine treatment selection and minimize overtreatment.
Presented by: Constantin Rieger, MD, Department of Urology, Universitäsklinikum Köln, 50937 Cologne, Germany
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Reference:
- Grossman HB, Natale RB, Tangen CM, Speights VO, Vogelzang NJ, Trump DL, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003;349(9):859-66.
- Powles T, Sridhar SS, Loriot Y, Rosenberg JE, Bellmunt J, Hussain SA, et al. Perioperative durvalumab plus neoadjuvant gemcitabine and cisplatin in muscle-invasive bladder cancer. N Engl J Med. 2024;390(15):1389-1400.