(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress was host to a presidential symposium. Dr. Jun Guo presented the results of a trial of disitamab vedotin + toripalimab (DV+T) versus chemotherapy as 1st line therapy in patients with locally advanced or metastatic urothelial carcinoma (la/mUC) with HER-2 expression.
HER-2 targeted antibody-drug conjugate monotherapy has demonstrated efficacy in the post-chemotherapy setting for HER2-positive urothelial carcinoma and is approved in both China (disitamab vedotin) and the USA (T-DXd).1,2
An ORR of 76.3% and a median PFS of 9.3 months were observed with DV + toripalimab (a humanized anti-PD-1 monoclonal antibody) in patients with previously untreated or chemotherapy-refractory HER2-expressing (IHC 1+, 2+, or 3+) la/mUC based on the previous phase Ib/II RC48-C014 study.3 HER2 expression is highly prevalent in urothelial carcinoma, with HER2 IHC ≥1 + accounting for up to 70% of urothelial carcinoma.4-7
The RC48-C016, an open-label, multicenter, randomized phase III trial, was conducted to evaluate DV+T versus chemotherapy in the 1st line treatment of patients with HER2-expressing la/mUC in China. In this presentation, Dr. Guo reported the prespecified final progression-free survival (PFS) analysis and interim overall survival (OS) analysis.
The study design of RC48-C016 is illustrated below. The key inclusion criteria were as follows:
- Treatment-naïve patients with unresectable locally advanced or metastatic urothelial carcinoma
- IHC 1+, 2+, or 3+
- Eligible for platinum-based chemotherapy
- Excellent performance status
Eligible patients underwent 1:1 randomization to:
- Disitamab vedotin + toripalimab (no set maximum cycles)
- Gemcitabine + cisplatin/carboplatin (maximum: 6 cycles)
The dual primary endpoints were:
- PFS, by blinded independent central review (BICR)
- OS
Secondary endpoints were:
- PFS, investigator-assessed
- Objective response rate (ORR), disease control rate (DCR), and duration of response (DoR)
- BICR and investigator-assessed
- Safety
- Quality of life
- Pharmacokinetics
- Immunogenics

The study flow chart is illustrated below. 811 patients were screened between June 2022 and August 2024. The median follow-up was 18.2 months. 484 patients were randomized to the experimental (n=243) and control arms (n=241).

The baseline patient characteristics are summarized below. The median patient age was 66 years. Notably, 46-51% of patients had upper tract urothelial carcinoma. 52% had visceral metastases. 78% of patients had HER2-3+ expression. 48% were cisplatin ineligible.

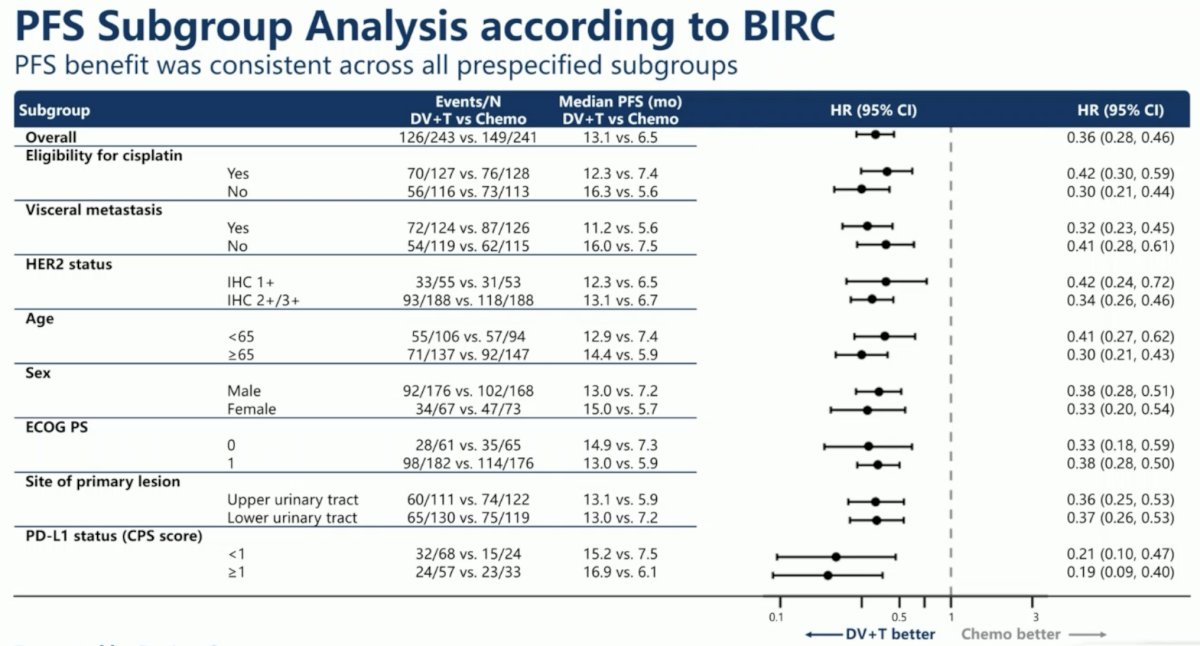
DV+T significantly improved PFS by 64%, compared to chemotherapy (median: 13.1 vs 6.5 months; HR: 0.36, 95% CI: 0.28–0.46, p<0.0001):

Subgroup analyses of PFS demonstrated consistent survival benefits in favor of DV+T across all subgroups, including HER2 expression status (1+ vs 2+/3+).
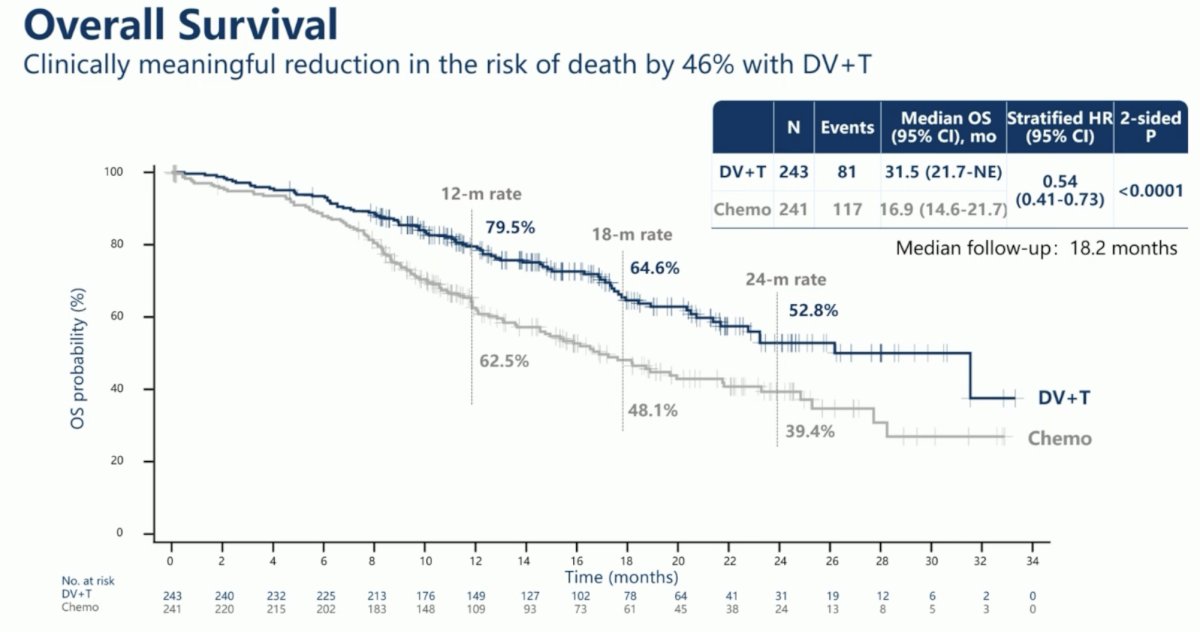
The combination of DV+T significantly reduced the risk of any-cause death by 46% (median: 31.5 vs 16.9 months; HR: 0.54, 95% CI: 0.41–0.73, p<0.0001):
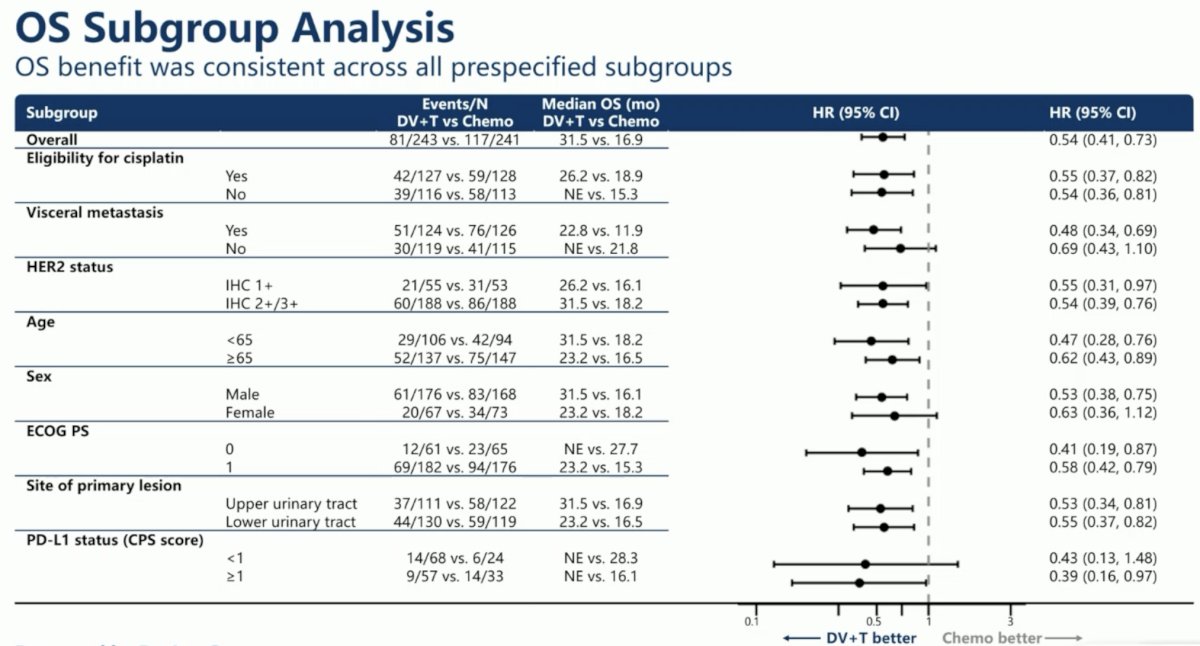
Subgroup analysis of OS demonstrated significant benefits in favor of DV+T across all subgroups, including HER2 expression status (1+ vs 2+/3+).
The ORR, assessed by BICR, favored DV+T (76% vs 50%). Notably, the complete response (CR) rate in the DV+T arm was only 4.5%.

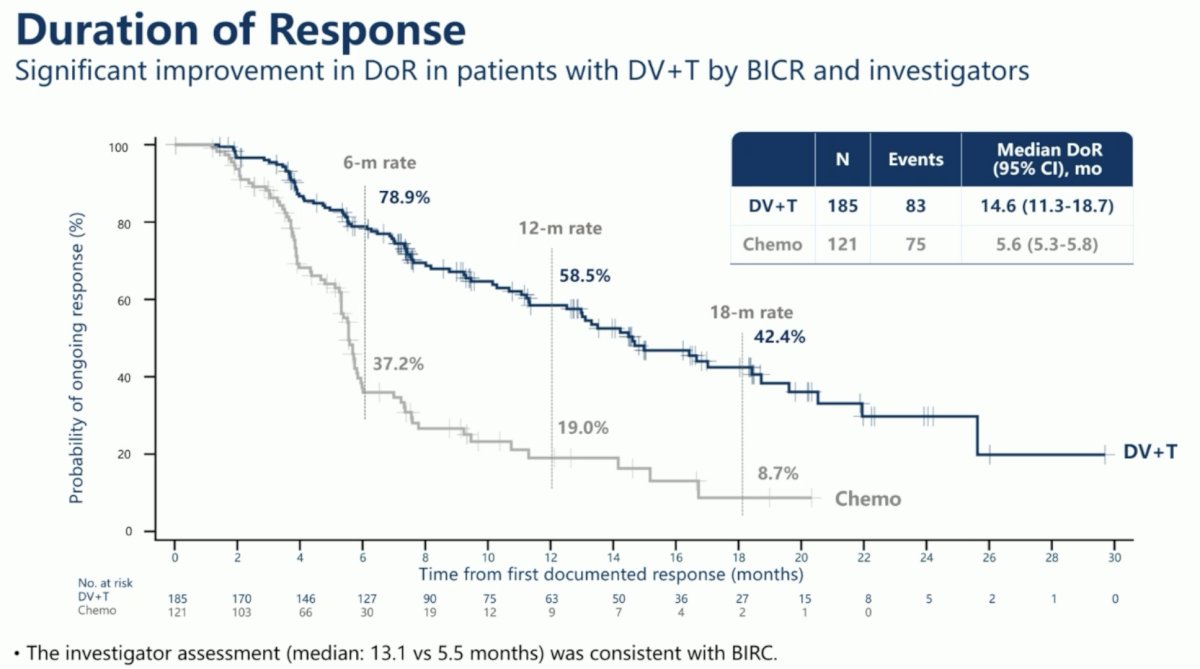
The duration of response was 14.6 months in the DV+T arm versus 5.6 months with chemotherapy.
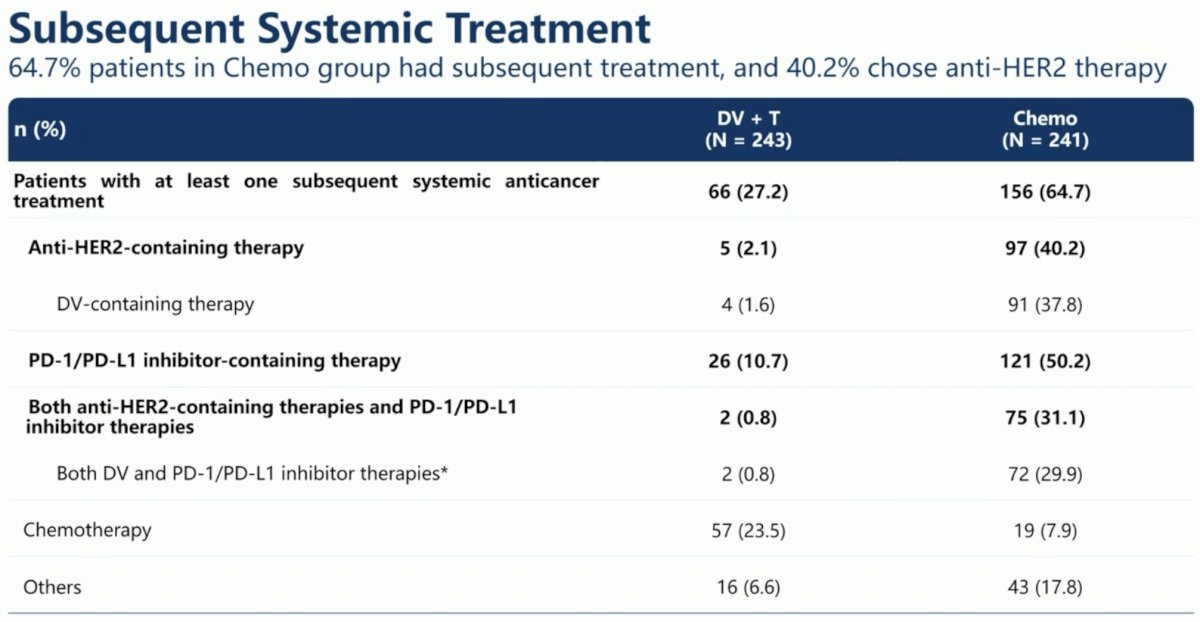
65% of patients in the chemotherapy group received subsequent systemic treatment, compared to 27% of patients in the DV+T arm. As expected, a higher proportion of patients in the chemotherapy arm received subsequent anti-HER-2-containing (40% vs 2%) and PD-1/PD-L1 inhibitor therapies (50% vs 11%).
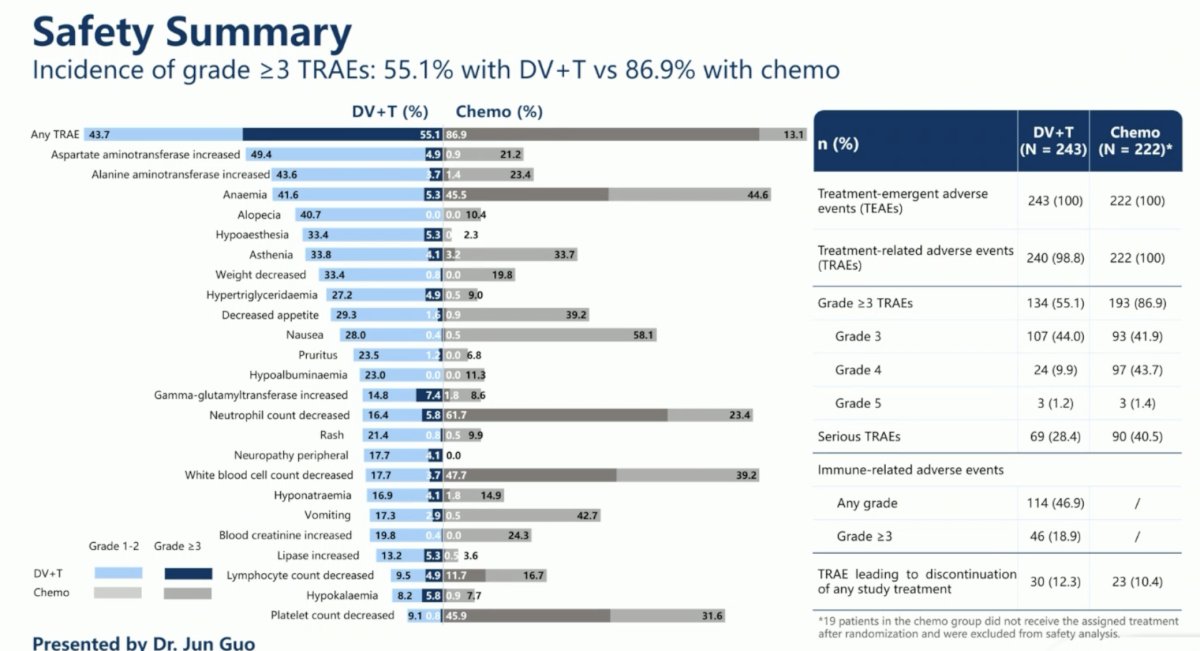
Patients in the DV+T arm had a lower incidence of grade ≥3 treatment-related adverse events (TRAEs; 55% vs 87%). Serious TRAEs were observed in 28% and 41% of patients in the DV+T and chemotherapy arms, respectively. TRAEs leading to study treatment discontinuation were observed in 12.3% and 10.4% of patients, respectively.
Dr. Guo concluded as follows:
- The Phase III RC48-C016 study demonstrated for the first time the superiority of an anti-HER2 antibody drug conjugate plus an anti-PD1 inhibitor in a biomarker-selected patient population with locally advanced or metastatic urothelial carcinoma
- Disitamab vedotin + toripalimab led to a clinically meaningful and statistically significant prolongation of PFS and OS versus platinum-based chemotherapy in patients with previously untreated HER2-expressing locally advanced or metastatic urothelial carcinoma
- PFS (per BIRC): median, 13.1 versus 6.5 months; HR, 0.36 (95% CI: 0.28-0.46); P<0.0001.
- OS: median, 31.5 versus 16.9 months; HR, 0.54 (95% Cl: 0.41-0.73); P<0.0001
- PFS and OS benefits were consistent across HER expression levels and other prespecified subgroups
- The safety profile of DV+T was consistent with that of each agent and overall was more favorable than that of platinum-based chemotherapy.
- Incidence of grade ≥ 3 TRAEs: 55% with DV+T vs 87% with chemotherapy
- DV+T offers a valuable new treatment option and represents a potential new standard of care for the 1st line treatment of patients with HER2-expressing locally advanced or metastatic urothelial carcinoma.
Presented by: Jun Guo, MD, Peking University Cancer Hospital & Institute, Beijing, China.
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:- Sheng X, Wang L, He W, et al. Efficacy and safety of trastuzumab deruxtecan in patients with HER2-expressing solid tumors: primary results from the DESTINY-PanTumor02 phase II trial. J Clin Oncol. 2024; 42(12):1391–1402.
- Meric-Bernstam F, Makker V, Oaknin A, et al. Efficacy and safety of trastuzumab deruxtecan in patients with HER2-expressing solid tumors. J Clin Oncol. 2024; 42(1):47–58.
- Zhou L, Yang KW, Zhang S, et al. Disitamab vedotin plus toripalimab in patients with locally advanced or metastatic urothelial carcinoma (RC48-C014): a phase Ib/II dose-escalation and dose-expansion study. Ann Oncol. 2025; 36(3):331–339.
- Koshkin VS, Schafer JM, Scherrer E, et al. Testing and interpretation of human epidermal growth factor receptor 2 protein expression and ERBB2 gene amplification in advanced urothelial carcinoma. JCO Precis Oncol. 2025; 9:e2400879.
- Zhou L, Shao Z, Liu Y, et al. HER2 Expression Associated with Clinical Characteristics and Prognosis of Urothelial Carcinoma in a Chinese Population. Oncologist. 2023; 28(8):e617–e624.
- Uzunparmak B, Haymaker C, Raso G, et al. HER2-low expression in patients with advanced or metastatic solid tumors. Ann Oncol. 2023; 34(11):1035–1046.
- Zhu X, Chan E, Turski ML, et al. HER2 overexpression in urothelial carcinoma with GATA3 and PPARG copy number gains. Oncologist. 2024; 29(8):e1094–e1097.