(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to a urothelial carcinoma poster session. Dr. Jens Bedke presented an analysis of the phase III CREST trial evaluating immune-mediated adverse events associated with the combination of sasanlimab + Bacillus Calmette-Guérin (BCG).
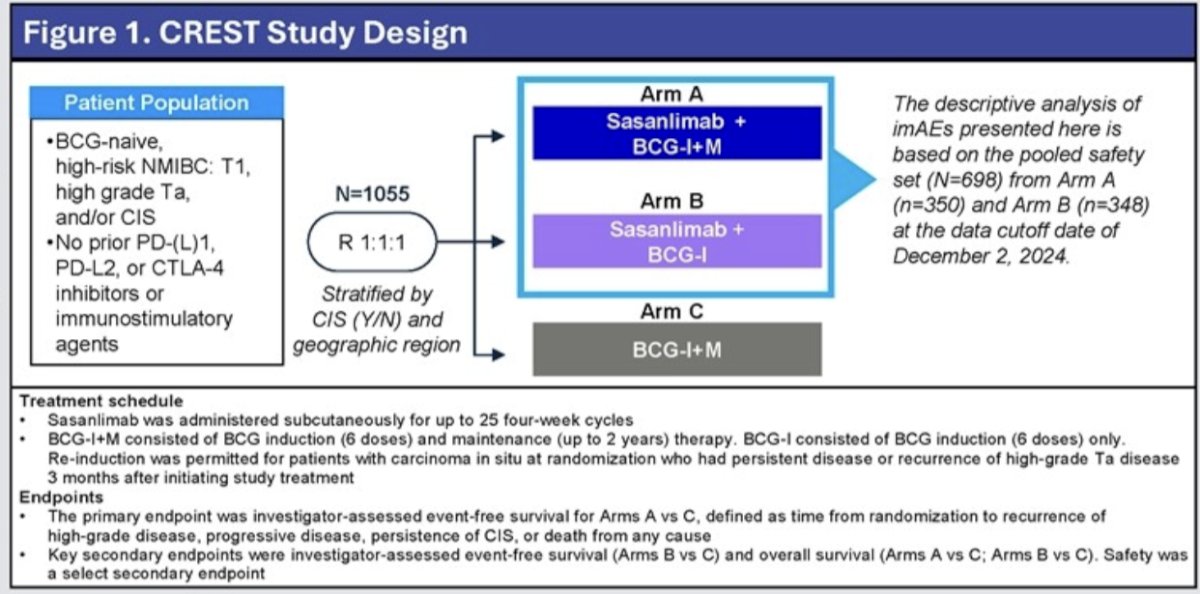
CREST (NCT04165317) is a global, open-label, phase 3, randomized study that showed a statistically significant prolongation of event-free survival for subcutaneous sasanlimab in combination with BCG induction + maintenance (BCG-I+M; Arm A) compared with BCG-I+M alone (Arm C) in patients with high-risk NMIBC (HR: 0.68; 95% CI: 0.49–0.94; one-sided P=0.0095).1
The overall safety profile of sasanlimab in combination with BCG has been previously reported and was consistent with the known safety profile for each individual agent. PD-1/PD-L1 inhibitors, including sasanlimab, are associated with immune-mediated adverse events (imAEs), which may affect various organ systems.2-4 Guidance for monitoring and management of imAEs was included in the CREST protocols. In current clinical practice, the management of imAEs is outlined in product labels and existing guidelines and involves comprehensive diagnostics and treatments, such as corticosteroids and hormonal therapy.5-10
Baseline demographics and disease characteristics of the intent-to-treat population have been reported previously.1 The safety analysis set comprised all patients who were randomized to a treatment arm and received ≥1 dose of a study drug. As of the data cutoff date (December 2, 2024), the safety analysis set consisted of 698 patients: 350 patients in the sasanlimab in combination with BCG-I+M arm and 348 patients in the sasanlimab in combination with BCG-I arm (Figure 1).
All analyses are descriptive, and data from both treatment arms containing sasanlimab in combination with BCG are presented as pooled data. imAEs are presented in categories, which include a cluster of MedDRA Preferred Terms representing similar clinical symptoms or syndromes. Safety assessments consisted of monitoring and documenting AEs and laboratory abnormalities throughout the treatment and up to 90 days post-final dose (safety assessment period), with clinical and laboratory assessments conducted at least every 4 weeks. imAEs were classified as imAEs by the sponsor, and each category has been characterized by maximum severity according to NCI CTCAE version 5.0.
ExposureIn the safety analysis set, BCG-I was completed by 96–97% of all patients in Arms A–C. The median number of BCG-M doses received was 12 for sasanlimab in combination with BCG-I+M arm (Arm A) and 15 for the BCG-I+M arm (Arm C).
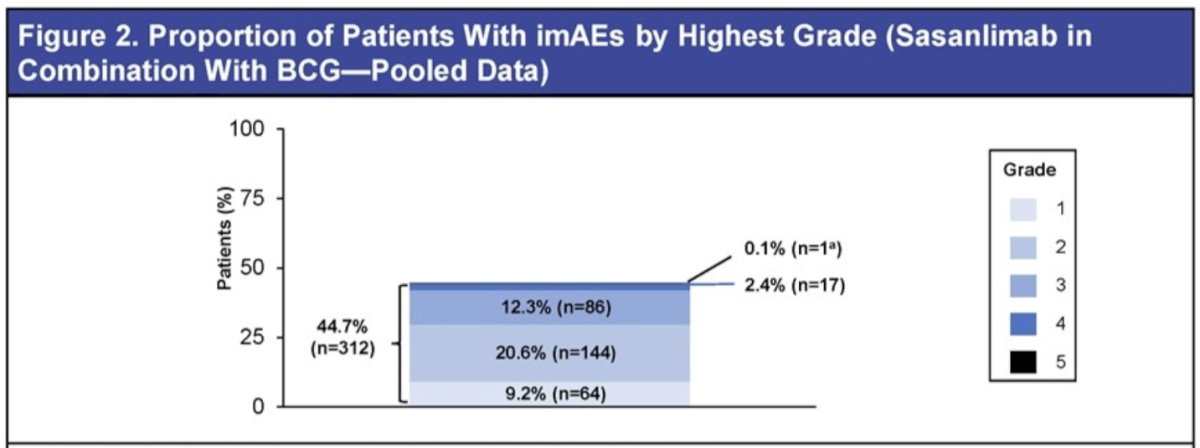
Frequency and severity of imAEsThe rates of imAEs were similar between the sasanlimab in combination with BCG-I+M arm (any grade: 42.6%; grade ≥3: 15.7%) and the sasanlimab in combination with BCG-I arm (any grade: 46.8%; grade ≥3: 14.1%). imAEs of any grade were reported in 44.7% of patients in the pooled population (Figure 2).
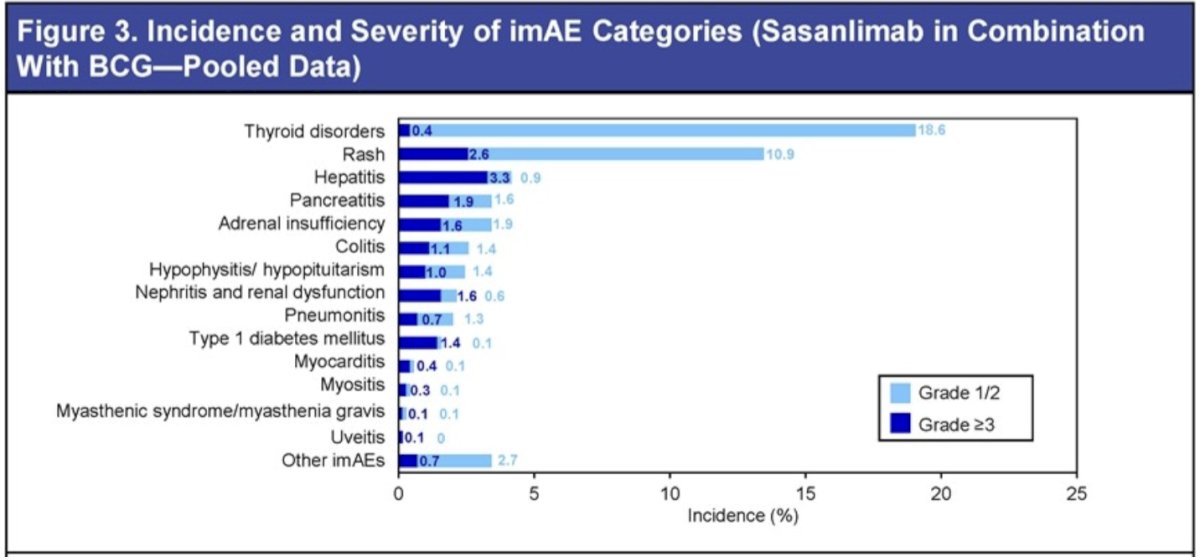
Serious imAEs and imAEs leading to hospitalization occurred in 11.2% and 10.3% of patients, respectively. The most common any-grade imAEs by category were thyroid disorders (19.1%) and rash (13.5%), and the most common grade ≥3 imAEs by category were hepatitis (3.3%) and rash (2.6%).
The median time to first onset of any-grade imAE was 16.1 weeks.
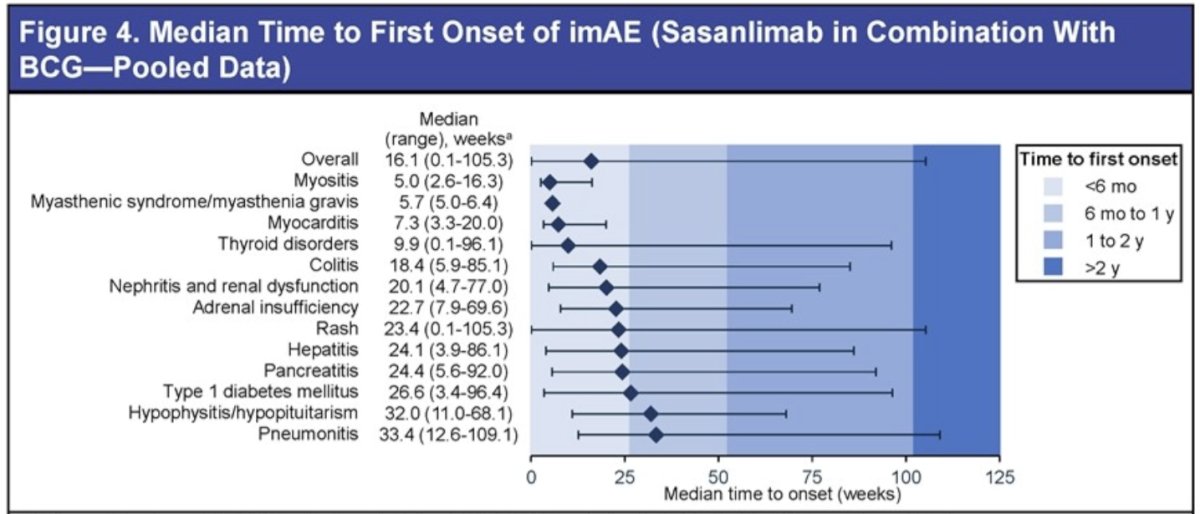
The median time to first onset was <6 months for most imAE categories, with all categories having a median time to first onset <1 year.
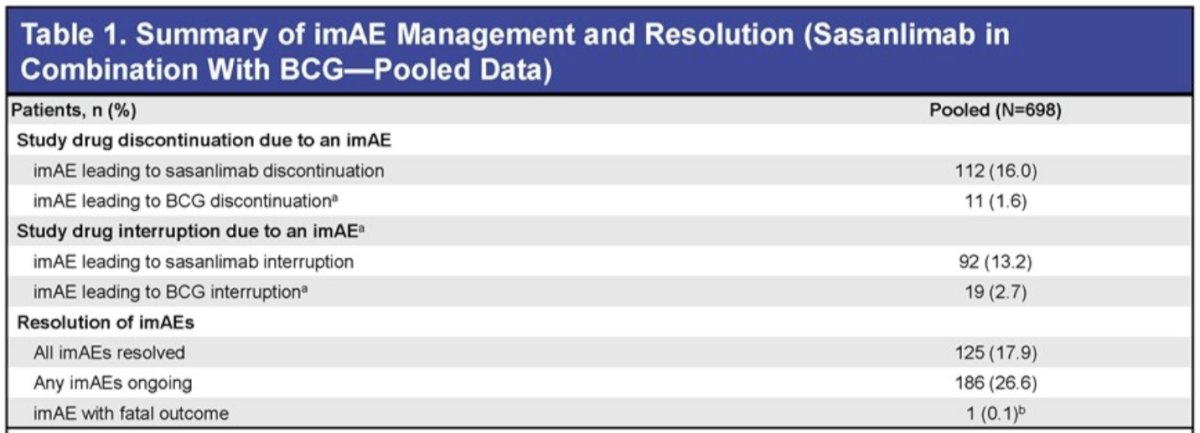
Dose modification for imAEsimAEs led to interruption of sasanlimab in 13.2% of patients and BCG in 2.7% of patients. The most common reasons for interruption of sasanlimab were:
- Thyroid disorder (4%)
- Rash (3%)
- Pancreatitis (1.6%)
The most common reasons for BCG interruption were:
- Colitis (0.7%)
- Pancreatitis (0.4%)
- Pneumonitis (0.4%)
Permanent discontinuation of sasanlimab due to imAEs occurred in 16% of patients, and permanent discontinuation of BCG occurred in 1.6% of patients. The most common reasons for discontinuation of sasanlimab were:
- Rash (3%)
- Hepatitis (2.7%)
- Adrenal insufficiency (1.6%)
The most common reasons for BCG discontinuation were rash (0.6%) and hepatitis (0.3%).
Overall, 44.6% of patients with an imAEs received corticosteroids, including 24.7% who received ≥40 mg total daily prednisolone dose equivalent. A high proportion of patients with adrenal insufficiency (100%) and hypophysitis/hypopituitarism (94.1%) received corticosteroids.
Immune suppressants, excluding corticosteroids, were used in 10 patients (3.2%), including 4 with rash, 2 with hepatitis, 1 with nephritis and renal dysfunction, 1 with myositis, and 2 with other imAEs.
Thyroid replacement therapy was required for 73.7% of patients with an immune-mediated thyroid disorder. All 11 patients with immune-mediated type 1 diabetes required insulin.
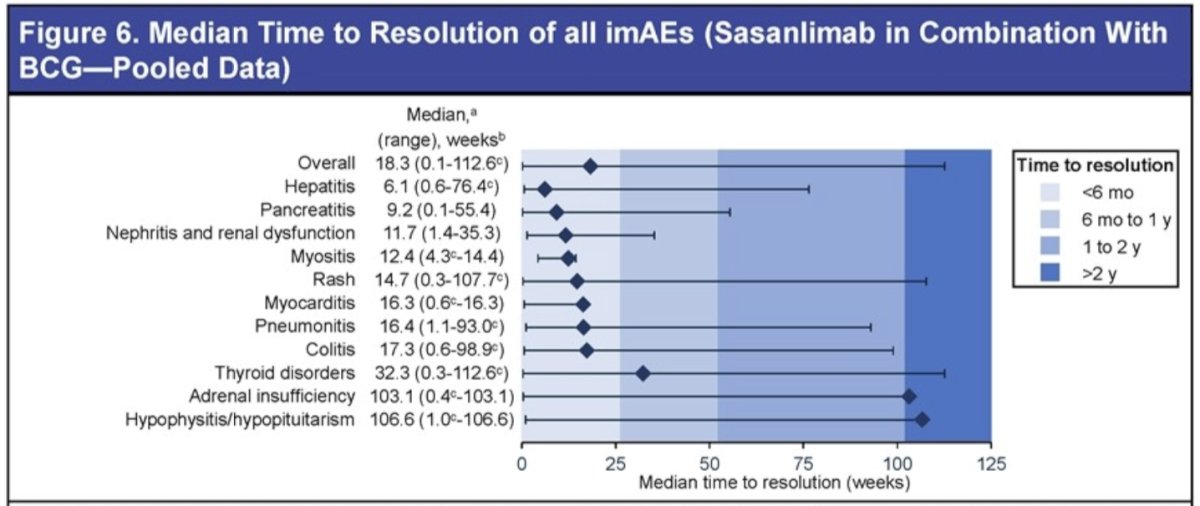
Outcomes of imAEsAt the data cutoff date, 17.9% of patients had all imAEs resolved, 26.6% of patients had ≥1 ongoing imAE, and 1 patient (0. 1%) had an imAE with a fatal outcome. The overall median time to resolution across all imAE categories was 18.3 weeks. imAE categories with the longest median time to resolution were hypophysitis/hypopituitarism, adrenal insufficiency, and thyroid disorders.
Dr. Bedke concluded as follows:
- Sasanlimab in combination with BCG showed a safety profile consistent with both the anti-PD-1/PD-L1 drug class and BCG
- No increased risk of either immune-mediate adverse events associated with sasanlimab or BCG-related adverse events was observed with the combination
- Immune-mediate adverse events were mostly grade 1 or 2
- For most immune-mediate adverse events categories, the median time to first onset was within the first 6 months of treatment initiation, and most resolved within 6 months of onset.
- Immune-mediate adverse events were effectively managed in line with standard guidelines, including treatment modifications (interruptions and discontinuations) and corticosteroids and/or hormonal therapy
Presented by: Jens Bedke, MD, Professor, Department of Urology and Eva Mayr-Stihl Cancer Center, Klinikum Stuttgart, Stuttgart, Germany
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
- Shore ND, Rosenberg JE, Tagawa ST, et al. Pembrolizumab plus enfortumab vedotin in advanced urothelial carcinoma. Nat Med. 2025; 31(10):2806-2814
- Yan T, Zhang Y, Liu X, et al. Mechanistic insights into checkpoint inhibitor toxicities. Front Pharmacol. 2025; 16:1519082.
- Sonpavde GP, Agarwal N, Galsky MD, et al. Emerging biomarkers and future directions in immunotherapy toxicity. Future Oncol. 2021; 17(20):2545-2558.
- Mavadia A, Patel H, Khan S, et al. Toxicity profiles of novel immunotherapy
- Thompson JA, Schneider BJ, Brahmer JR, et al. Management of immunotherapy-related toxicities: NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2019; 17(3):255-289.
- Schneider BJ, Naidoo J, Santomasso BD, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol. 2021; 39(36):4073-4126.
- Haanen J, Obeid M, Spain L, et al. Management of toxicities from immunotherapy: ESMO clinical practice guideline. Ann Oncol. 2022; 33(12):1217-1238.
- Brahmer JR, Abu-Sbeih H, Ascierto PA, et al. Society for Immunotherapy of Cancer (SITC) consensus recommendations on managing toxicities. J Immunother Cancer. 2021; 9(6):e002435.
- US Food and Drug Administration. Accessed September 16, 2025. https://labels.fda.gov/
- European Medicines Agency. Accessed September 16, 2025. https://www.ema.europa.eu/