(UroToday.com) The 2025 ESMO annual meeting featured a urothelial carcinoma proffered paper session and a discussant presentation by Dr. Bradley McGregor discussing two abstracts “ALBAN: A phase 3, randomized, open-label, international study of intravenous atezolizumab and intravesical BCG versus BCG alone in BCG-naïve high-risk, non muscle invasive bladder cancer” by Dr. Morgan Roupret and “Durvalumab in combination with BCG for BCG-naïve, high risk non muscle invasive bladder cancer: final analysis of the phase 3, open-label, randomized POTOMAC trial” by Dr. Maria De Santis.
Dr. McGregor started with a case of a 63-year-old male smoker (30 pack-year history) who presented to his PCP with hematuria, and a CT urogram showing a 2.7 cm bladder mass. A TURBT revealed a T1 urothelial carcinoma without CIS, and a repeat TURBT showed no evidence of disease. The patient asks, “What can I expect from BCG? Should I do more?”
SWOG 85071previously showed that BCG maintenance weekly x3 at months 3, 6, 12, 18, 24, 30, and 36 in patients without disease at 3 months (after induction) had a significant reduction in recurrence (p < 0.0001) and progression (p < 0.04) versus induction alone in 550 randomized patients. However, Dr. McGregor noted that in SWOG 8507, 28% of patients had residual disease and were ineligible for randomization, only 50% of patients with CIS had no disease after induction, and only 16% completed three years of BCG maintenance.
Biologically, it makes sense to pair BCG with immune checkpoint blockade given that PD-L1 expression is increased in BCG-resistant patients. Importantly, the guidelines for management following BCG failure are to recommend cystectomy. The AUA & SUO (2024) guidelines state “In a high risk patient with persistent or recurrent disease with one year following treatment with two induction cycles of BCG or BCG maintenance, a clinician should offer radical cystectomy”, while EAU (2025) states “at the present time, treatments other than radical cystectomy are considered oncologically inferior in patients with BCG-unresponsive disease.”
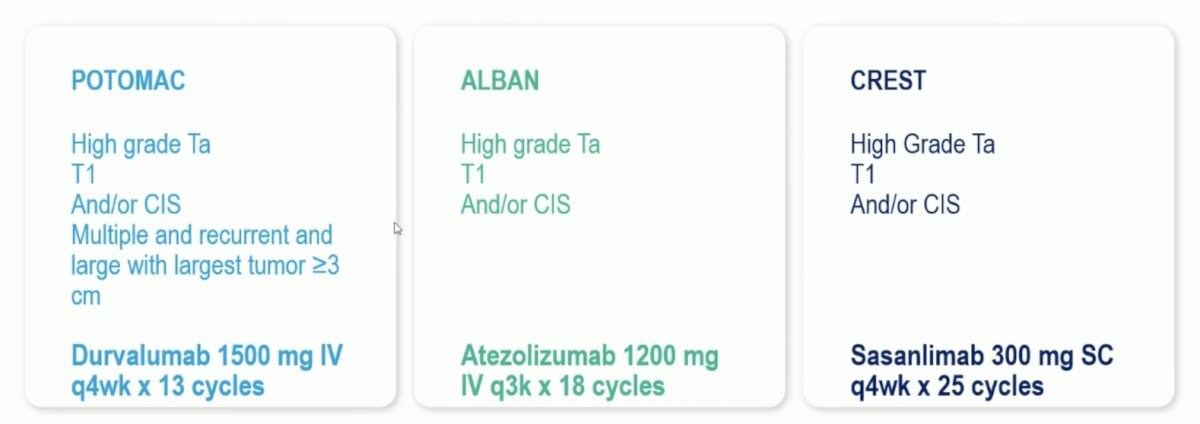
Prior to today’s ALBAN and POTOMAC presentation, Dr. McGregor emphasized that CREST was previously presented at AUA 2025 by Dr. Neal Shore and subsequently published in Nature.2 CREST assessed sasanlimab + BCG in BCG-naïve, high-risk non-muscle invasive bladder cancer. Arm A received sasanlimab administered subcutaneously combined with BCG induction and maintenance, Arm B received sasanlimab with BCG induction only, and Arm C received BCG induction and maintenance alone. The primary endpoint was event-free survival, defined as recurrence of high-grade disease, progressive disease, persistence of CIS, or death from any cause. The risk of experiencing an event-free survival event was 32% lower with sasanlimab + BCG compared to BCG induction and maintenance alone (stratified HR 0.68, 95% CI 0.49–0.94; 1-sided p-value: 0.0095). Dr. McGregor noted that the eligibility criteria were similar between the three trials, although their immune checkpoint inhibitor duration was different:
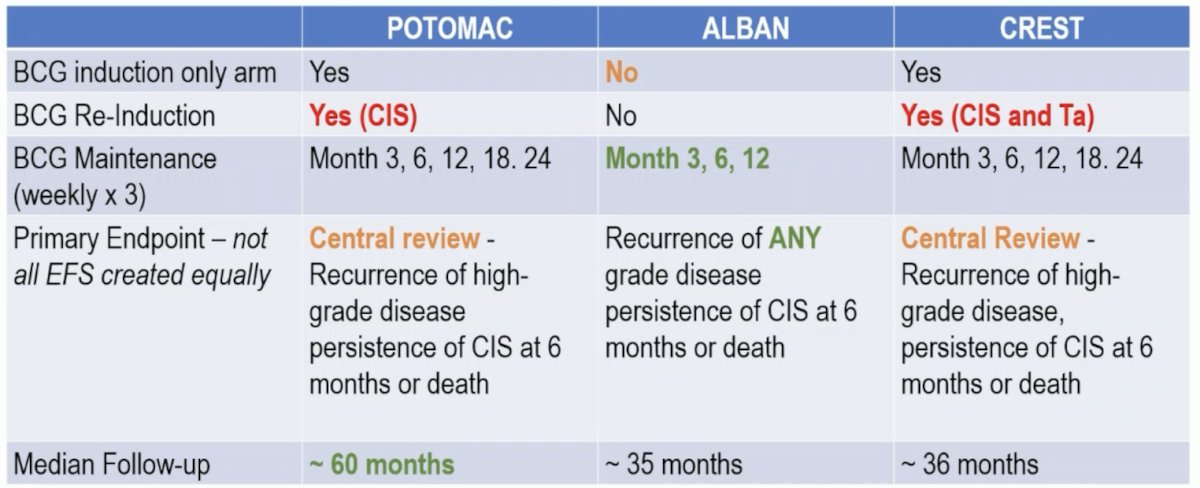
Notably, ALBAN had the highest rate of CIS, but yet the lowest rate of “pure CIS” among the three cohorts. A full comparison of the key aspects of the trial designs is highlighted in the following table, with notably longer follow-up in the POTOMAC trial:
There are several important points regarding CREST and POTOMAC. Of note, systemic immune checkpoint inhibitor therapy is not a replacement for adequate BCG:
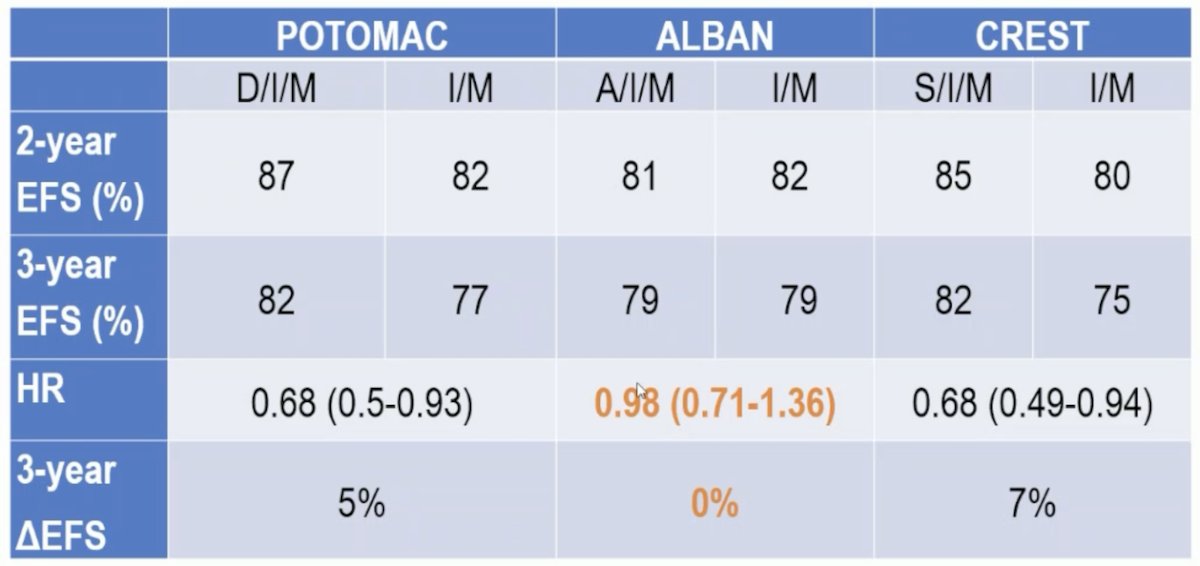
When looking at the key trial results, there was very little differentiation in the absolute difference in 3-year event-free survival between the three trials, whereas for context, the 5-year disease-free survival in patients who had no disease at 3 months was 60% in SWOG 8507:
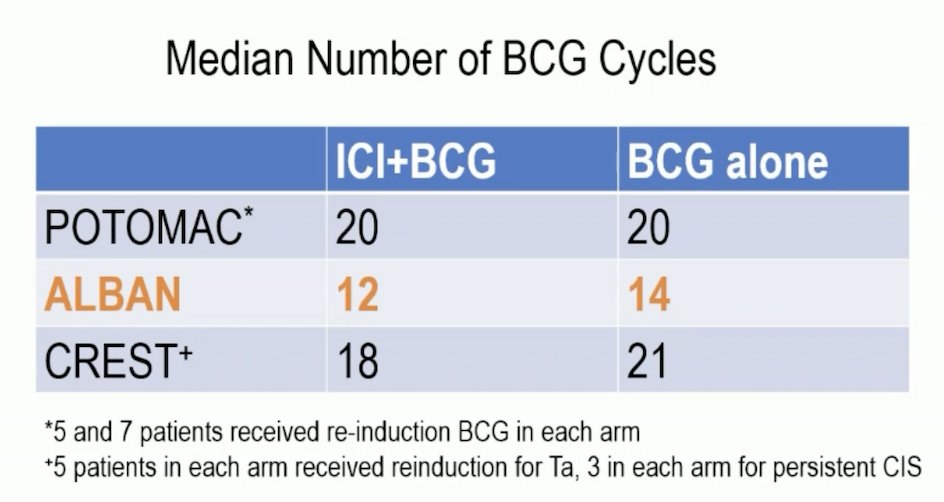
Dr. McGregor also highlighted that there were very low rates of distant recurrence or muscle-invasive disease in any of the trials. One possible explanation for differences in outcomes between trials is the lower median number of BCG cycles received in the ALBAN trial compared to the POTOMAC and CREST trials:
Several additional reasons why outcomes were not significant in ALBAN include:
- A lower-risk population? ALBAN had the highest percentage of CIS, but the lowest T1 and Ta among the other trials
- Persistent CIS at 6 months was uncommon, with only 7/112 patients with persistent CIS as an event
- Shorter BCG duration
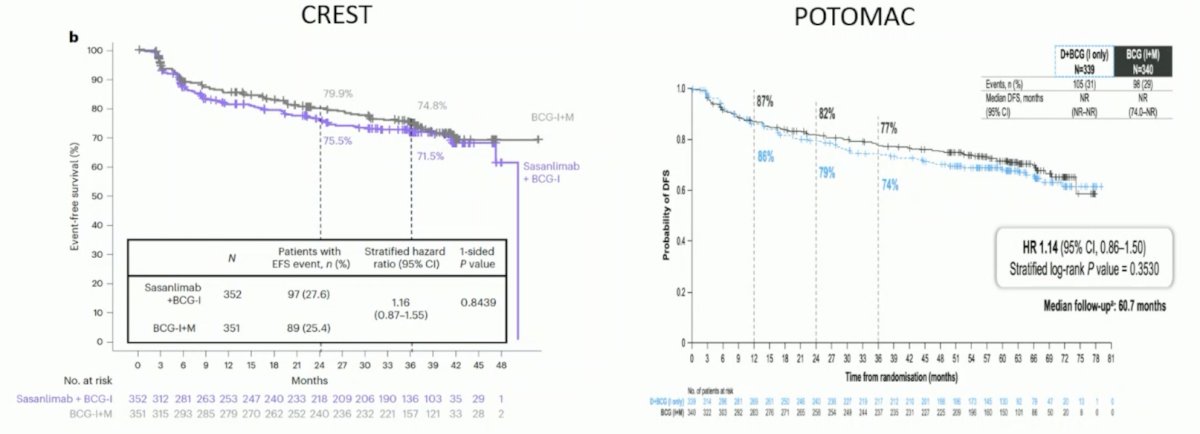
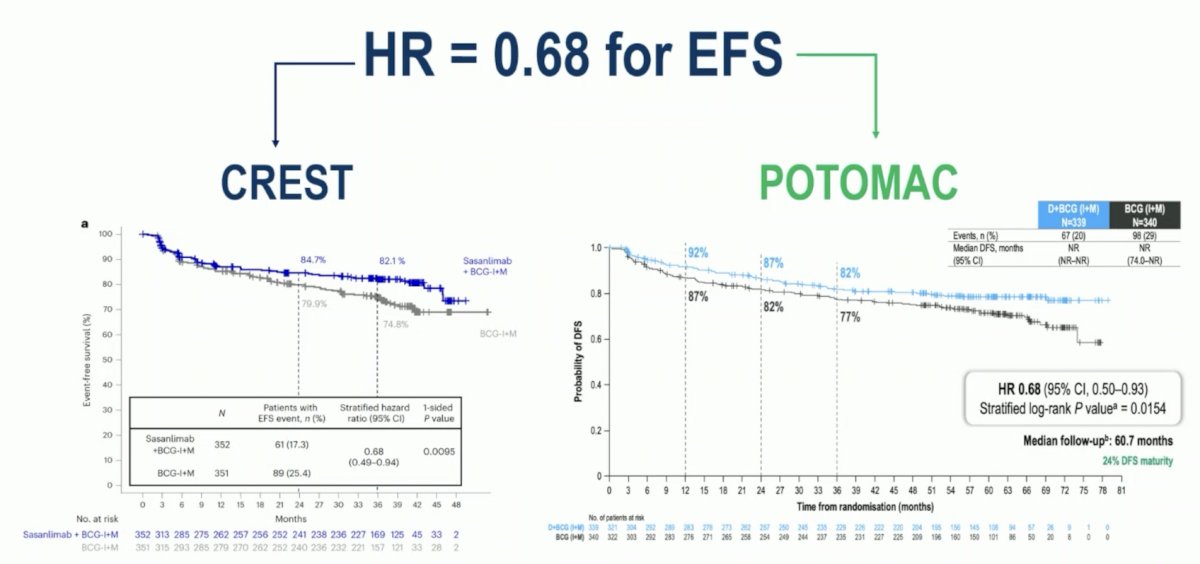
Both CREST and POTOMAC had identical event-free survival hazard ratios of 0.68:
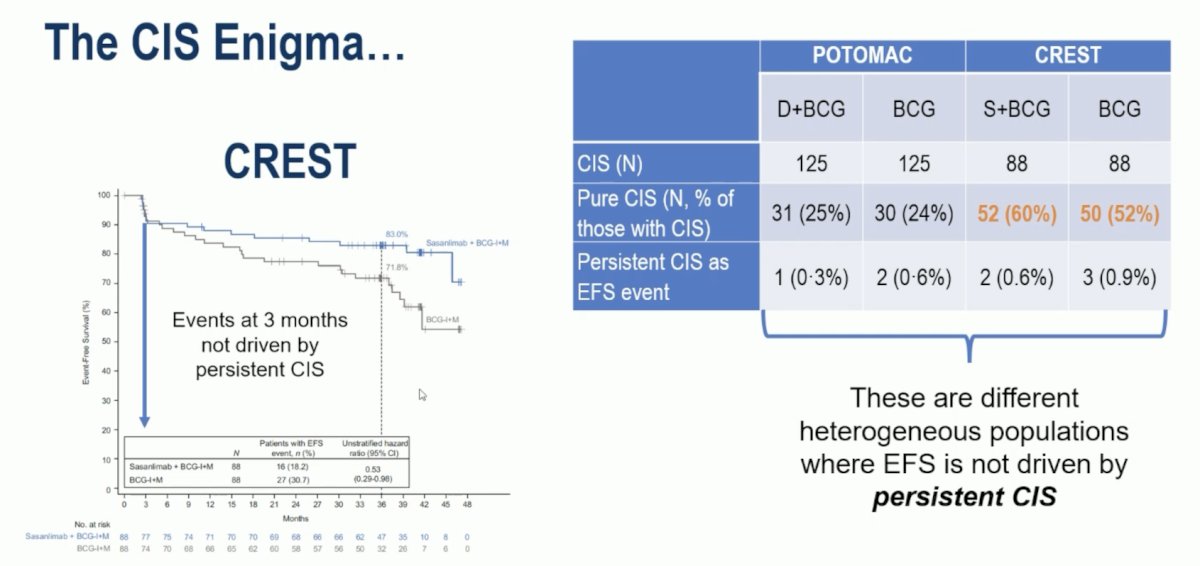
At a high level, the CIS enigma in these trials may be best explained by these being different heterogeneous populations where event-free survival is not driven by persistent CIS:
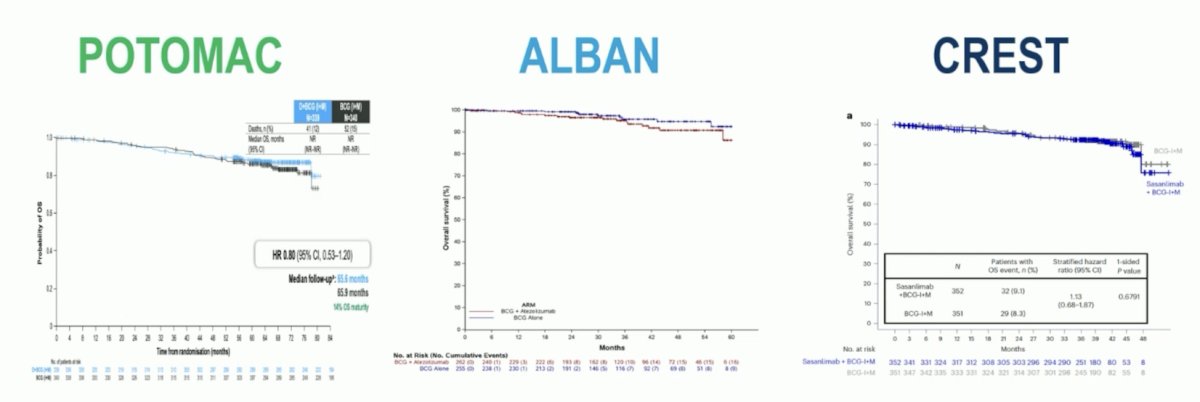
Regardless of event-free survival efficacy, it is important to note that there was no detrimental effect on overall survival across all 3 trials (with the longer follow-up in POTOMAC noteworthy):
Despite no detriment to overall survival, there appears to be a toxicity downside for these patients. For example, in CREST:
- 18% had a thyroid disorder
- 3.4% had adrenal insufficiency
- 2.3% had hypophysitis
- 2% had diabetes mellitus
- 0.6% had myasthenia gravis
- There were 2 treatment-related deaths (in the sasanlimab induction arm)
- 20% of patients needed steroids
Dr. McGregor notes that there are several unanswered questions from bladder preservation guidelines in muscle invasive disease, but applicable to the BCG high risk non muscle invasive bladder cancer population:
- How can we elucidate patients' understanding of endpoints?
- Does event-free survival correlate with cystectomy-free survival?
- Is cystectomy free survival the ultimate endpoint?
- What are the surveillance costs and therapy/monitoring patient burden?
- What is the loss of bladder function secondary to treatment?
- Who will benefit from further bladder-sparing strategies?
Indeed, there is more to come, specifically the BRIDGE trial, which will help us position gemcitabine + docetaxel into the treatment paradigm.
Looking back at the patient case from the beginning of the presentation, Dr. McGregor notes that we can tell the patient the following points today:
- Modern TURBT and BCG outcomes are markedly superior to the original study
- 3-year event-free survival among all patients given BCG was ≥ 75%
- The addition of durvalumab for one year or sasanlimab for 2 years in high-risk patients improves the chance of not having a recurrence of high-risk disease at 3 years 5–7% with a 20–30% chance of grade 3 toxicities
- A similar trial with atezolizumab showed no benefit, possibly due to differences in the BCG schedule and/or the patients enrolled
- The effect of any of these combinations on cystectomy-free survival remains unknown, and we have multiple trials exploring options should BCG not work
Dr. McGregor concluded his discussant presentation with the following take-home messages:
- Adequate BCG therapy represents a high bar – with modern TURBT and BCG delivery, we have dramatically improved outcomes
- Immune checkpoint blockade is NOT a replacement for BCG
- The presence of CIS represents a heterogeneous patient population
- Adding immune checkpoint blockade to BCG is not a “slam dunk.”
- There is a clear improvement in event-free survival in two well-conducted large trials with 2 years of BCG therapy
- We need to weigh toxicities – short and long term, with the degree of benefit and potential for salvage therapies
- Are there biomarkers to help choose?
Presented by: Bradley A. McGregor, MD, Dana-Farber Cancer Institute, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
References:
- Lamm DL, Blumenstein BA, Crissman JD, et al. Maintenance bacillus Calmette-Guerin immunotherapy for recurrent TA, T1, and carcinoma in situ transitional cell of the bladder: A randomized Southwest Oncology Group Study. J Urol. 2000;163:1124-1129.
- Shore ND, Powles TB, Bedke J, et al. Sasanlimab plus BCG in BCG-naïve, high-risk non-muscle invasive bladder
Durvalumab in Combination with BCG for BCG-naive, High-Risk, Non-Muscle-Invasive Bladder cancer (POTOMAC): Final Analysis of a Randomised, Open-Label, Phase 3 Trial.
ALBAN (GETUG-AFU 37): A Phase 3, Randomized, Open-Label, International Trial of Intravenous Atezolizumab and Intravesical Bacillus Calmette-Guérin (BCG) Versus BCG Alone in BCG-Naive High-Risk, Non-Muscle Invasive Bladder Cancer (NMIBC).
ESMO 2025: ALBAN: A Phase 3, Randomized, Open-Label, International Study of IV Atezolizumab and Intravesical BCG versus BCG Alone in BCG-Naïve High-Risk NMIBC